Article Text

Abstract
Objectives Cardiovascular diseaseand heart failure (CHF) are leading causes of death in systemic lupus erythematosus (SLE). The underlying mechanisms for increased CHF in SLE are unclear but myocardial inflammation and lupus myocarditis (LM) may play a role. We propose that 18F-fluorodeoxyglucose–positron emission tomography (18F-FDG–PET)/CT can help diagnose LM.
Methods This report describes eight patients with presumed LM; five patients were evaluated due to active cardiorespiratory symptoms and three patients were participating in a pilot study to determine the prevalence of subclinical myocarditis in SLE. Clinical characteristics, laboratory and cardiac testing including electrocardiography (ECG), transthoracic echocardiogram (TTE), coronary artery evaluation as well as 18F-FDG–PET/CT imaging are discussed.
Results Four patients were African American and the others were Hispanic. Half presented with chest pain; 37% had dyspnoea and 25% were asymptomatic. The median SLE Disease Activity Index (SLEDAI-2K) was 5 (2–18) and SLICC Damage Index (SDI) 0.5 (0–5). The median troponin level was 0.08 ng/mL (0–0.9). The most common ECG findings were non-specific ST-T wave abnormalities (n=5). Fifty per cent of the patients had a decreased ejection fraction on TTE and all patients had diffuse myocardial FDG uptake on 18F-FDG–PET/CT consistent with myocardial inflammation.
Conclusion This case series is the first to describe the use of 18F-FDG–PET/CT in the diagnosis of LM and discuss the clinical characteristics and cardiac findings of eight patients with LM supporting the role for cardiac 18F-FDG–PET/CT in its diagnosis.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease characterised by autoantibody-mediated systemic injury resulting in heterogeneous manifestations. Throughout the course of the disease, cardiac involvement occurs in over 50% of patients with SLE1–3 and every structure of the heart can be affected. Notably, cardiovascular disease (CVD) has become the leading cause of death in SLE.4 Epidemiological studies estimate a 2–9-fold increased risk of cardiovascular events in patients with lupusof all age groups with an increased prevalence of myocardial infarction, stroke and heart failure compared with the general population.5–8 Importantly, the excess in CVD seen in SLE is only partially accounted for by traditional CVD risk factors and SLE itself is an independent risk factor for CVD.9–13
Although the underlying mechanisms leading to CVD in lupus remain unclear, persistent systemic and local inflammation are the main proposed contributing factors.14–18 Lupus myocarditis (LM) is a recognised complication of SLE with a prevalence reported to be as high as 57% based on postmortem studies,19–21 and a 10% mortality described in case series at 3-year follow-up.22 However, the diagnosis of myocarditis in SLE remains challenging in clinical practice. LM is currently diagnosed clinically, supported by abnormalities noted on electrocardiograms (ECG) and transthoracic echocardiograms (TTE). As ECG and TTE findings are not sensitive or specific for myocarditis, the accuracy of this diagnosis is limited. Endomyocardial biopsies are considered the gold standard for diagnosing myocarditis, yet they are not routinely performed due to the related risk of the invasive procedure and associated potential sampling error. Furthermore, the sensitivity and specificity of the procedure in LM is unknown.23–25 As such, non-invasive imaging techniques to diagnose, characterise and provide prognostic data for LM have become a research priority.26 To date, studies using non-invasive imaging such as cardiac MRI (cMRI) have suggested that clinical diagnostic criteria for LM underdiagnose cases and that many patients with SLE have subclinical myocardial inflammation.27 28
Positron emission tomography (PET)/CT has emerged as a novel imaging modality for active inflammation, currently being evaluated in several rheumatic diseases.29–32 The ability of FDG to accumulate in inflammatory cells has made it a useful tool in measuring inflammation, and in particular in sarcoid myocarditis 18F-FDG–PET/CT is a more sensitive diagnostic test than cMRI.33–37 Given the lack of data on 18F-FDG–PET/CT imaging in the evaluation of myocardial inflammation in SLE, we describe eight patients with active myocardial inflammation on 18F-FDG–PET/CT scanning consistent with LM.
Methods
Patients
Eight patients with SLE are described in this case series. Five patients were diagnosed during their admission at Columbia University Medical Center, June 2014–March 2016 for cardiorespiratory symptoms. The remaining three patients were diagnosed as part of a pilot study of 10 participants to identify the prevalence of myocarditis in patients with SLE without clinical CVD. All patients were 18 years of age or older and met the 1997 American College of Rheumatology (ACR) classification criteria for SLE.38 The study was approved by the Columbia University Institution Review Board.
Outcome measure
18F-FDG PET/CT Myocardial uptake. Imaging was performed on an MCT 64 PET/CT scanner (Siemens Medical Solutions USA,Knoxville, Tennessee, USA). A low-dose CT transmission scan (120 kV, 25 mA) was obtained for attenuation correction of PET data. All patients were on a carbohydrate-free diet for 24 hours. Patients were injected with 10±0.1 mCi of 18F-FDG intravenously using an antecubital or dorsal forearm catheter. A list mode 3D PET scan was acquired for 10 min following a 90 min uptake period post-18F-FDG injection. Non-gated attenuation-corrected images were reconstructed yielding 3 mm effective resolution. Corridor 4DM software was used to visually assess myocardial 18FDG uptake as well as semiautomatically quantify mean radiotracer uptake in the myocardium. Quantification of inflammation by 18F-FDG PET/CT involved measurement of standardised uptake values (SUV) in the myocardium.
Clinical covariates
Demographics, comorbidities and smoking history were self-reported and collected from questionnaires and patient interview. Hypertension was defined as a systolic BP of ≥140 mm Hg, diastolic BP of ≥90 mm Hg at the time of the evaluation or antihypertensive medication use. Diabetes was defined as glycated haemoglobin (HbA1c) greater than 6.4% or use of diabetes medications. All medications were documented from patient interview and medical records. SLE disease duration was defined as the duration in years from the date of physician diagnosis. SLE disease activity was calculated using the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K).39 Disease damage was determined by the calculation of the Systemic Lupus International Collaborating Clinics (SLICC) damage index for SLE (SDI).40
Coronary artery disease (CAD)
In four patients, CAD was evaluated by the Agatston coronary artery calcium score.41 The remaining four patients underwent cardiac catheterisation.
Electrocardiography (ECG)
Twelve-lead ECGs (25 mm/s paper speed and 10 mm/mV amplitude) were performed and interpreted by board-certified cardiologists.
Transthoracic echocardiogram (TTE)
TTEs were performed by trained registered cardiac sonographers using conventional GE machines with commercially available software. End-diastolic and end-systolic frames, five anatomical landmarks (septal, lateral, anterior and inferior mitral annulus and apex of the left ventricle (LV)) were manually identified, and a semiautomated endocardial border detection was performed, followed by LV endocardium tracking throughout the cardiac cycle. LV end-diastolic and end-systolic volumes were indexed by body surface area. Doppler, 3-D echocardiography and contrast agents were used at the discretion of the sonographer. A normal ejection fraction (EF) was defined as >50%.
Laboratory covariates
Autoantibodies including antinuclear antibodies, anti-SSA/Ro, anti-SSB/La, anti-ds-DNA, anti-Smith, anti-RNP, antiphospholipid antibodies and other pertinent laboratories including complement levels (C3, C4), erythrocyte sedimentation rate (ESR), high-sensitivity C reactive protein, troponin and pro-beta-natriuretic peptide (pro-BNP) levels, were performed at the clinical laboratory at New York Presbyterian Hospital and the Core Laboratory of the Columbia University Irving Institute for Clinical and Translation Research.
Results
Patientscharacteristics
Patient demographics, clinical and SLE characteristics and supportive tests are depicted in table 1. Fifty per cent of the patients were Hispanic and 50% were African American. Six were women (75%). The mean age of the patients was 43 years and mean disease duration was 11 years. One patient had both diabetes and hypertension. One patient was a current smoker, two patients were prior smokers and five were never smokers. Five of the patients had major organ involvement: four had a diagnosis of lupus nephritis, one of which was active at the time of the diagnosis of myocarditis; one had neuropsychiatric lupus (NPSLE) in the past. None of the patients had antiphospholipid antibody syndrome.
Patient characteristics and case description
Clinicalpresentation
Four patients complained of chest pain, one of dyspnoea, one had both chest pain and dyspnoea and two did not have any cardiac or respiratory symptoms. Five patients were diagnosed at the time of admission for acute lupus flare and cardiac symptoms; the other three were participants in a study to evaluate the prevalence of subclinical myocarditis and on further questioning one patient acknowledged shortness of breath (table 1).
Disease activity and pertinentlaboratories
The median SLEDAI-2K was 5 (2–18) and the SLICC SDI score was 0.5 (0–5). Median C3 level was 84 (64–91) and C4 was 13 (11–27). ESR was elevated in six patients with a median level of 27 (8–52) and an elevated high-sensitivity CRP was noted in five patients with a median of 3 (0.5–17). Troponin and pro-BNP levels were significantly elevated in one patient (table 1).
Cardiac testing
The most common ECG findings were non-specific ST-T wave abnormalities (n=5) and sinus tachycardia (n=5). Right bundle branch block (n=2) and left atrial dilatation (n=1) were also noted. On TTE, half of the patients had a decreased EF. The mean EF was 41% (20%–60%). Three patients had pericardial effusions and two patients had global hypokinesis. Three of the four patients evaluated by Agatston coronary artery calcium scoring had a measurement of 0; the remaining patient had a score of 17, not clinically significant for atherosclerosis. The other four patients underwent coronary artery catheterisation: three had angiographically normal coronary arteries and one had 70% stenosis of the left anterior descending artery and 100% occlusion of the first diagonal branch (D1); the latter was diagnosed with a non-ST elevation myocardial infarction (NSTEMI) in addition to active myocarditis. However, the contribution of the D1 branch occlusion versus the active myocarditis to the troponin elevation and depressed EF could not be accurately ascertained (table 1). One patient had an endomyocardial biopsy that showed non-specific changes: preserved myocardial fibres with mild hypertrophic changes and increased cellular organelles consistent with non-specific mild myocardial hypertrophy.
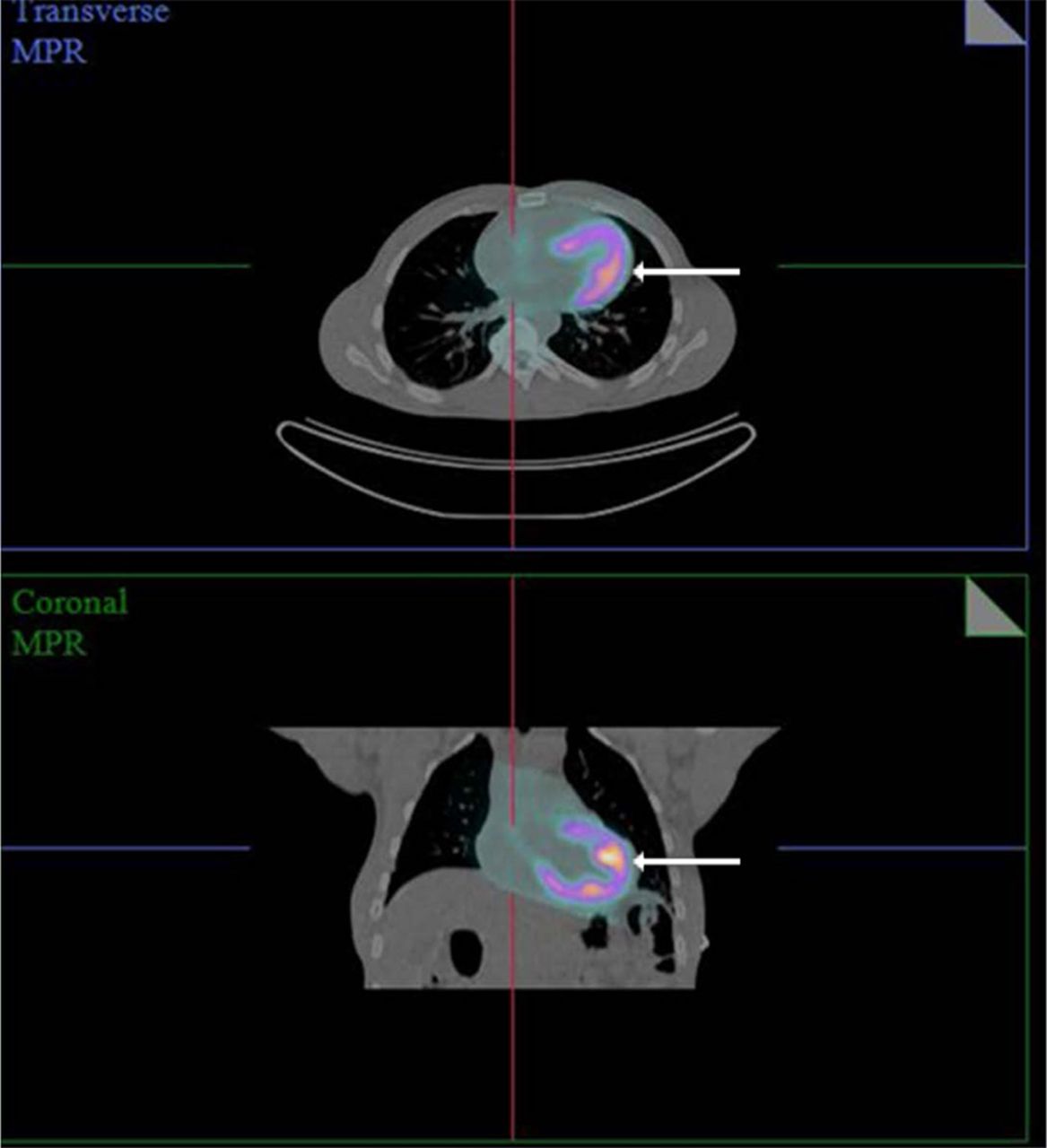
On 18F-FDG–PET/CT imaging, all patients had diffuse myocardial uptake consistent with diffuse inflammation and suggestive of a diagnosis of myocarditis, including the patient with a concomitant NSTEMI (figure 1).

{kind=link}
18F-fluorodeoxyglucose positron emission tomography/CT showing diffuse myocardial FDG uptake (arrows) on a transverse and coronal view in a patient with SLE described in this series. FDG, fluorodeoxyglucose; SLE, systemic lupus erythematosus.
Treatment
All patients were treated with high-dose steroids (1 mg/kg of prednisone). One patient also received 3 days of pulse solumedrol intravenous (1000 mg). All patients were treated with immunosuppressive therapy: 7/8 with mycophenolate mofetil with a goal dose of 3 g per day in divided doses; 1/8 with cyclophosphamide at 500 mg/m2 intravenous monthly due to coexisting lupus nephritis which had been previously non-responsive to mycophenolate mofetil (table 1).
Follow up
Two patients had follow-up 18F-FDG–PET/CT imaging: one had no myocardial uptake after 5 months, while the other showed persistent diffuse uptake/inflammation but with decrease in FDG uptake by an SUV factor of 3 at 13 months. Five had a follow-up TTE within 6–8 months: mean EF was 57% (range 50%–60%) and all had normal wall motion. Two of these five patients had impaired LV relaxation of unclear significance (present on initial TTE). One patient was lost to follow-up (table 1).
Discussion
This case series describes eight patients with 18F-FDG–PET/CT myocardial uptake suggestive of LM. The clinical presentation and characteristics of our patients with LM were non-specific and variable, emphasising the need for additional sensitive testing for LM and supporting a role for cardiac 18F-FDG–PET/CT for the early diagnosis and prompt treatment of this condition.
CVD is the leading cause of death in SLE.4 It has been estimated that patients with SLE aged 35–44 have a greater than 50-fold increased relative risk of myocardial infarction compared with age matched controls, and that in general, patients with SLE have up to a 7–10-fold greater relative risk of angina, myocardial infarction and stroke.8 10 13 42 This excess in cardiovascular risk is not fully explained by the increase in traditional risk factors, suggesting that SLE-specific factors play a central role.12
The increased cardiovascular risk in SLE is considered multifactorial and potentiated by a combination of systemic and local inflammation.14–18 In idiopathic subclinical myocarditis, local inflammation and endothelial activation lead to microvascular disease and dysfunction, promoting accelerated atherosclerosis.43 While LM is a recognised complication of SLE, its true prevalence is unknown as its diagnosis remains challenging. A recent case series of 29 patients with LM reported a 10% mortality at 3-year follow-up, stressing the importance of recognising and treating this lupus manifestation. 22 Currently, LM is diagnosed based on clinical suspicion, abnormalities of ECG and echocardiograms44–47 and lack of an alternative diagnosis. Zawadowski et al 46 described 24 patients with LM and similar to our findings, the most common ECG abnormalities were non-specific ST changes (70%) and sinus tachycardia (63%), while 78% had a reduced EF on TTE. However, these findings are non-specific for LM. Although endomyocardial biopsy is considered the gold standard, its use in LM is unclear and it has been noted to have poor sensitivity and specificity. Sampling error and interventional risk often outweigh the benefits of the procedure23 25 resulting in ambiguity in both the diagnosis and treatment of this condition.
A recent interest has emerged in investigating the utility of non-invasive imaging techniques to further characterise myocarditis in lupus. Refined imaging modalities are more sensitive and inform on cardiac morphology and function and help assist in prognostication.24 26 Two recent studies have assessed the cMRI findings of patients with lupusin association with disease activity. Mavrogeni et al studied patients with active SLE without specific cardiovascular complaints and compared their findings to a commonly used clinical criteria for the diagnosis of acute myocarditis. While 5/20 patients with SLE fulfilled clinical criteria for myocarditis, cMRI was found to be positive in 16/20. Interestingly, of those with cMRI-proven myocarditis who underwent endomyocardial biopsy, only 3/7 had positive immunohistology.27 In addition, Zhang et al compared patients with inactive SLE (SLEDAI <3) with healthy controls using T2 time values on T2 cMRI mapping sequences,28 which have been shown to detect myocardial oedema and have high sensitivity and specificity for acute inflammation detection (94 and 97%, respectively).24 Despite being clinically quiescent, the SLE group was found to have T2 times significantly higher than controls suggesting the occurrence of subclinical myocarditis in patients with clinically inactive SLE with preserved myocardial contractility.28 Our study reflects Zhang’s findings in that our case series includes patients with SLE without cardiac symptoms that were found to have active myocardial uptake on FDG PET. While data on treating subclinical myocarditis are lacking, the two patients in our series without active cardiac symptoms were treated with steroids and immunosuppressants based on the acknowledgement of the borderline normal EFs, expert opinion and patient preference. Although the clinical implications of subclinical myocarditis in lupus remain unknown, these findings raise awareness for the need of additional identifiers of patients with SLE at risk for development of myocarditis as well as longitudinal follow up to evaluate its prognosis and associated risk for the development of cardiovascular events.
The use of 18F-FDG–PET/CT in cardiovascular inflammatory diseases has been best described in the setting of sarcoidosis. Comparable to LM, cardiac sarcoid involvement can be subclinical and have non-specific findings on ECG and echocardiogram.48 49 In cardiac sarcoidosis, FDG-PET has been shown to have equivalent or higher sensitivity to delayed enhancement cMRI in detecting active lesions.50 By targeting the increased glucose uptake of infiltrating granulocytes and tissue macrophages, FDG PET/CT has been shown to delineate inflammation with high sensitivity. Hence, the myocardial FDG uptake of the patients described in this series is likely to represent cardiac inflammation. Additional advantages of 18F-FDG–PET/CT imaging include its feasibility for patients with renal dysfunction and metal implants and having shorter time-frames than MRI studies. Furthermore, 18F-FDG–PET/CT provides quantitative measures of inflammation in the form of SUV that allow objective interval change assessments.51
To our knowledge, this is the first case series of lupus myocardial inflammation diagnosed by 18F-FDG–PET/CT scanning. Limitations include the small sample size, lack of pathological confirmation and lack of follow-up 18F-FDG PET/CT for all cases.
In conclusion, we describe a case series of patients with lupus with myocardial 18F-FDG–PET/CT uptake consistent with LM. Observational studies are needed to evaluate the sensitivity, specificity and overall clinical impact of this imaging modality in LM.
References
Footnotes
AA and LG-P are joint senior authors.
Contributors All authors contributed to all phases of the manuscript writing.
Funding Funding for this project was provided in part by the Rheumatology Research Foundation Scientist Development Award CU13-2392 (LGP).
Competing interests None declared.
Patient consent Not required.
Ethics approval Columbia University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data statement All available data can be obtained by contacting the corresponding author.