Article Text

Abstract
Objective Systemic lupus erythematosus (SLE) features high frequency of cardiovascular disease (CVD) and fluctuating complement levels. The clinical trial Atherosclerosis Prevention in Pediatric Lupus Erythematosus (APPLE) aimed to evaluate whether atorvastatin treatment reduced the progression of atherosclerosis in 221 patients with childhood-onset SLE (cSLE), using carotid intima media thickness (CIMT) as surrogates. We leveraged APPLE biorepository and trial data to investigate the relationship between complement and CVD in cSLE.
Methods Gene copy numbers (GCNs) for total C4, C4A and C4B were measured by TaqMan-based real-time PCR and Southern blotting, and analysed with laboratory and clinical parameters through Student’s t-test and χ2 analyses. Effects of total C4, C4A and C4B GCNs on the response to placebo or atorvastatin treatment and progression of CIMT were examined by regression analyses.
Results At baseline, C4 protein levels strongly correlated with GCNs of total C4 (p=1.8×10−6). Each copy of C4 gene increased mean serum C4 by 3.28 mg/dL. Compared with those without hypertension (N=142), individuals with hypertension demonstrated significantly elevated serum levels for C4 and C3 at baseline and serially (C4: P=5.0×10−25; C3: P=5.84×10−20). Individuals with ≥2 C4B genes had 2.5 times the odds of having hypertension (p=0.016) and higher diastolic blood pressure (p=0.015) compared with those with C4B deficiency. At the study end, subjects with ≥2 C4B and atorvastatin treatment had significantly slower increase in CIMT compared with those treated with placebo (p=0.018).
Conclusions cSLE with hypertension had elevated serum levels of C4 and C3 and higher GCN of C4B; cSLE with ≥2 C4B genes would benefit from statins therapy to prevent atherosclerosis.
- atherosclerosis
- atorvastatin
- gene copy number variation
- hypertension
- complement C4 and C3
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Individuals with systemic lupus erythematosus (SLE) are at high risk for experiencing a major adverse cardiovascular event in their lifetimes. Their risk for myocardial infarction is 9–50 times higher than that of the general population.1 Consequently, cardiovascular disease (CVD) is thought to be responsible for one-third of all deaths in patients with SLE.1 This subclinical process begins early in children, whose disease course is generally characterised by higher disease activity and longer duration than those with the adult-onset form of SLE.2 The relationship between systemic inflammation and atherosclerosis has been demonstrated in the general population3 and is at least partially mediated by the complement system. Increased serum concentrations of the C3 complement protein, for example, are proposed risk factors for human myocardial infarction.4 5 Under physiological conditions, the complement system protects a host by promoting immune complex (IC) solubilisation and clearance.6–8 In a patient with active SLE, however, excessive ICs are produced, some of which are proatherogenic.9 Inherited or homozygous deficiencies in any of the early components in the classical complement activation pathway (ie, C1q, C1s, C1r and C4) almost always result in an SLE phenotype early in life.10–13
Variations in gene copy number (GCN) of complement C4 also affect the development of SLE. The human C4 gene is located in the human leukocyte antigen class III region on chromosome 6. Each chromosome 6 contains one to five copies of C4 genes, allowing an individual to inherit between 2 and 10 copies of total C4 in a diploid genome.14 15 The most common GCN for total C4 is four, and for both C4A and C4B is two.14 Each copy of C4 gene encodes for one of two isotypes, acidic C4A or basic C4B. Variations at four amino acid residues between C4A and C4B, PCPVLD 1101–6 LSPVIH, result in activated C4B having a faster reaction rate but shorter half-life than activated C4A, as well as decreased binding affinity for peptide antigens such as those found on ICs.16–18 Individuals with childhood-onset SLE (cSLE) are more likely to have fewer copies of total C4 than those with adult SLE.19 We hypothesise that the relative inefficiency of IC clearance but stronger reactivity by activated C4B may expose individuals with a higher C4B GCN to increased end-organ IC deposition and subsequent disease complications such as accelerated atherosclerosis. Furthermore, inherited variations in complement C3 ‘fast’ and ‘slow’ allotypes (C3F and C3S, respectively) may play a role in disease. Human subjects with a C3F allotype, for example, were shown to be at higher risk for myocardial infarction and systemic inflammatory diseases such as vasculitis.20–22
Robust consumption of complement, leading to low serum levels of complement C4 and C3, is initiated by the presence of high concentrations of ICs. Excess complement activation has been implicated in the pathogenesis of lupus nephritis (LN), a major cause of hypertension in SLE.23–25 The inverse relationship between SLE disease activity and serum complement levels makes C4 and C3 protein levels convenient clinical biomarkers of disease activity. This relationship becomes complicated when considering that CVD, a result of chronic inflammation in SLE, would be associated with higher serum levels of C4 and C3.
Our study aims were to elucidate and clarify the dynamic relationship between CVD-related phenotypes, complement genetic profiles and response to anti-lipid therapies.
Patients and methods
Atherosclerosis Prevention in Pediatric Lupus Erythematosus trial design
The Atherosclerosis Prevention in Pediatric Lupus Erythematosus (APPLE) was a multicentre, prospective, randomised, placebo controlled clinical trial. In total, 221 children, adolescents and young adults (aged 10–21 years) with SLE, as determined by the 1997 American College of Rheumatology Revised Classification Criteria,26 were enrolled from 21 North American centres from the Childhood Arthritis and Rheumatology Research Alliance.27–29 Participants underwent 1:1 randomisation to receive placebo or atorvastatin (>50 kg: 10 mg/day, increasing to 20 mg/day at day 30; ≤50 kg: 10 mg/day). Participants were counselled to follow the American Heart Association Therapeutic Lifestyle Changes diet.30 The primary endpoint of the trial was rate of progression of mean–mean common carotid intima media thickness (CIMT). A clinically significant change was defined as a 0.0045 mm/year difference in the endpoint between the atorvastatin and placebo groups at the end of the trial. This endpoint was based on previous adult studies that demonstrated a significant increase in risk for cardiovascular events for every 0.16 mm increase CIMT.31 The authors reasoned that a child diagnosed with cSLE at 15 years of age would reach this clinically significant cut-off by the age of 50 years if they demonstrated a 0.0045 mm/year increase in CIMT. Secondary outcomes included other ultrasound CIMT measurements defined in the APPLE trial (mean–mean CIMT, mean–mean common CIMT, mean-max CIMT and mean-max common CIMT) as well as SLE disease activity, organ system damage, health-related quality of life and laboratory measures such as serum C3 and C4 concentrations, high-sensitivity C-reactive protein (CRP) and serum lipid levels. Each of these data points was collected at serial study visits over 3 years. On enrolment into the APPLE trial, physicians indicated whether participants had a past history of hypertension, which was further ascertained on multiple occasions. Automated systolic blood pressure (SBP) and diastolic blood pressure (DBP) measurements were taken under resting conditions at each visit.
Ultrasonography of carotid arteries in the APPLE trial
Two CIMT ultrasound examinations were performed at enrolment and at the end of the trial. One CIMT examination was performed at 6, 12 and 24 months for a total of seven examinations. Standardised measurements of the bilateral common carotid arteries (CCA), carotid bifurcations and proximal internal carotid artery CIMT were obtained at each examination. Mean-max and mean–mean CIMT were calculated and recorded using measurements from each measurement site. Mean-max and mean–mean common CIMT were calculated and recorded using measurements only from the CCA.27 A single reader with more than 20 years of experience reading CIMT research studies read all ultrasound scans for CIMT using Image Pro software (Media Cybernetics). To evaluate intra-reader reliability, a set of 68 studies were re-read. The intra-class correlation coefficient was 0.74 (95% CI: 0.61–0.83) for mean–mean common and 0.71 (0.56–0.81) for mean‐max CIMT measurements.27
Genotypes and phenotypes of complement C4
Biological samples were available for 200 of 221 participants. Paired genomic DNA and EDTA-plasma samples for 21 patients were not available. GCNs for total C4 (C4T), C4A and C4B were measured by TaqMan-based quantitative real-time PCR through five independent amplicons. Data were validated when total C4 GCN (C4T) was equal to the sum of C4A and C4B.14 GCN calls for 100 patients were further confirmed by Southern blot analyses using genomic DNA digested by TaqI restriction enzymes, and hybridised to genomic DNA probes corresponding to genomic fragments for (a) intergenic genomic fragments between 3′ region of RP and 5′ region of C4, (b) steroid 21-hydroxylase CYP21A1P and CYP21A2 and (c) 3′ regions of extracellular matrix protein tenascin TNXB and TNXA.32–34 Native C4 proteins from EDTA-plasma were resolved by high voltage agarose gel electrophoresis based on gross differences in electric charges, and used to elucidate C4A and C4B protein polymorphisms by immunofixation using goat antiserum against human C4 (Diasorin, Stillwater, MN, USA).34
Genotyping of complement C3: C3 fast and C3 slow
The C→G nucleotide change leading to Arg 102 Gly polymorphism for the slow and fast variants of C3 protein can be distinguished by HhaI restriction fragment length polymorphism.35 Genomic DNA fragments corresponding to nucleotides 4169 and 4502 of the human C3 gene were amplified by PCR, subjected to HhaI restriction digest, and resolved by agarose gel electrophoresis. The fast and slow alleles were shown as 333 bp, and 232+101 bp, restriction fragments, respectively.
Statistical analyses
We analysed baseline characteristics of APPLE participants based on dichotomised C4 GCN groups. Specifically, participants were grouped by whether total C4, C4A and C4B GCNs were low (<4 for total C4; <2 for C4A or C4B) or medium to high (≥4 for total C4; ≥2 for C4A or C4B). Baseline variables and their associations were examined through analysis of variance (ANOVA), Student’s t-test and χ2 tests. Stepwise logistic regression was used for risk factor analysis. Based on hypertensive status and treatment group, longitudinal changes in C4 and C3 protein levels and in CIMT variables were examined using repeated measures ANOVA models that included interaction effects. Significance of relationships was tested using post-hoc t-tests (Tukey). P values of ≤0.05 were considered significant. JMP V.13 (SAS Institute, Cary, NC, USA) was used for analysis.
Results
Baseline demographics and complement profiles of the APPLE trial cohort
Baseline demographic and clinical data for 221 patients with cSLE enrolled in the APPLE trial are shown in table 1. In all, 56 (25.5%) participants were African American, 106 (48.2%) were white and 58 (26.4%) were either of mixed race or other racial background. Mean age (±SD) of participants was 15.8±2.6 years. Mean body mass index (BMI) was 24.4±5.3 kg/m2. Mean SBP and DBP were 112.8±12.2 mm Hg and 66±9.6 mm Hg, respectively. In all, 73 patients (33.2%) had a history of hypertension; 104 (47.1%) had a history of kidney disorder, defined as previous or current nephrotic syndrome, nephritic syndrome or any class of LN on renal biopsy based on either the International Society of Nephrology/Renal Pathology Society36 classification or the WHO37 classification. At baseline, 67 participants (30.3%) were using or had previously used an anti-hypertensive medication (angiotensin receptor blocker, calcium channel blocker, beta blocker and/or ACE inhibitor). Specific indication for use of these medications was not documented.
Baseline demographics and complement profiles in cSLE41of the APPLE cohort
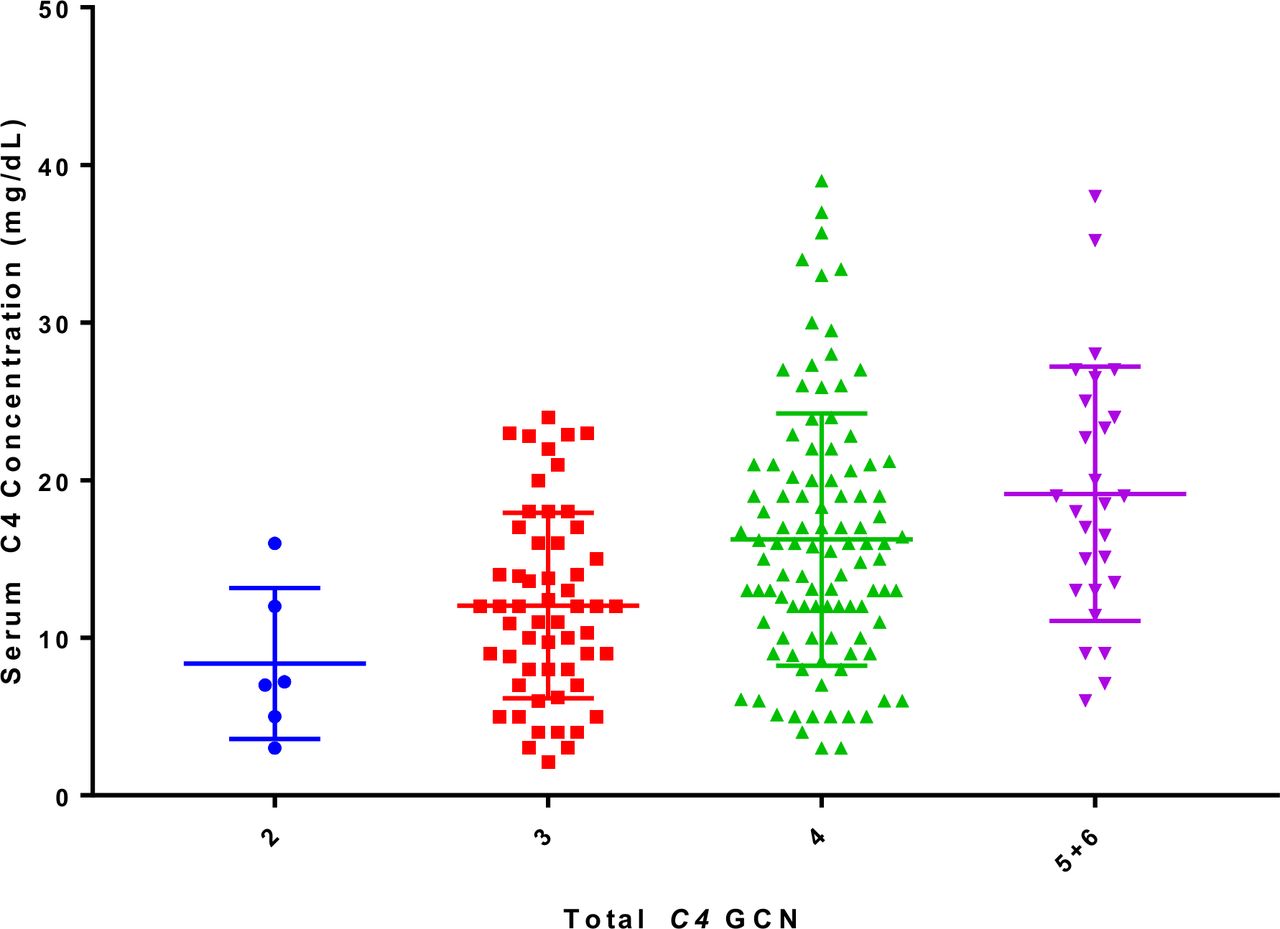
Complement C4 and C3 genotypes were successfully determined and validated on 183 participants (82.8%). GCNs for total C4, C4A and C4B varied between 2 and 6, 0 and 5, and 0 and 5, respectively. Mean total C4 GCN was 3.82±0.80. Mean C4A and C4B GCNs were 1.99±0.74 and 1.84±0.64, respectively. Baseline mean serum C4 concentration was 15.2±7.8 mg/dL. Serum C4 protein concentrations strongly correlated with total C4 GCN (ANOVA P=1.8×10-6). Based on linear regression analyses, each one-copy increase in C4 GCN resulted in an increase in mean serum C4 concentration of 3.28 mg/dL (figure 1).
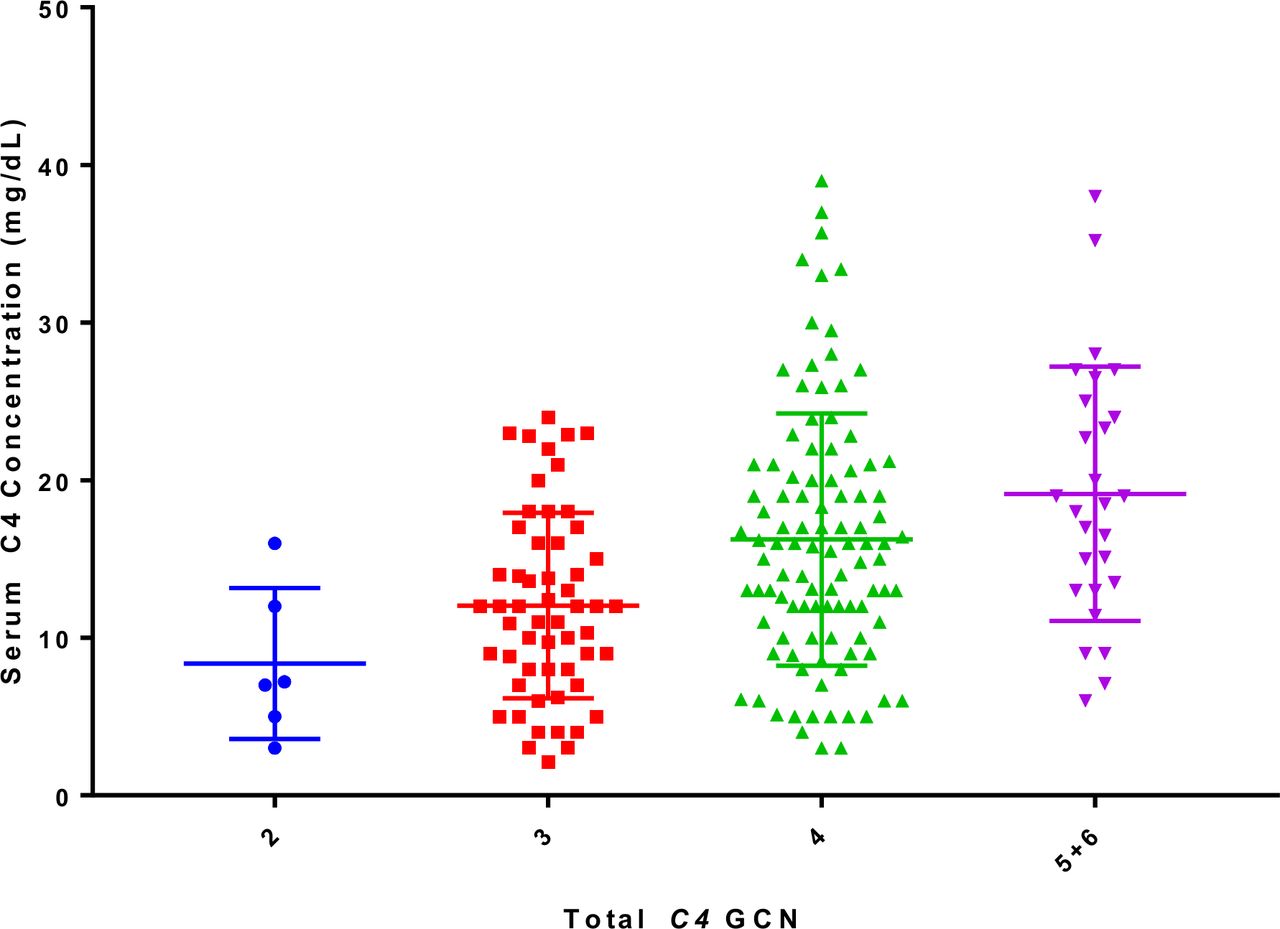
Baseline serum C4 concentrations in APPLE participants based on total C4 GCN. Mean and SD are shown. Participants with five and six copies of total C4 were grouped together because of small sample size (analysis of variance p value: 3.0×10−5). The linear regression formula for C4 protein concentration (mg/dL) was 2.62+3.28 x GCN of total C4. APPLE, Atherosclerosis Prevention in Pediatric Lupus Erythematosus; GCN, gene copy number.
Baseline mean serum C3 concentration was 100.7±29.0 mg/dL (table 1). For the C3 fast (F) and slow (S) variants, the most common genotype was SS (frequency 78.2%). Heterozygous fast and slow genotype FS, and homozygous genotype FF had a combined frequency of 21.8%. C3 F and S genotypes had no significant effect on serum C3 levels.
Baseline laboratory values and CIMT measurements
Patients with low copy number of total C4 genes has an earlier age of disease diagnosis than patients with medium or high copy number of total C4 (GCN=2 or 3: 12.53±3.08 years old; GCN=4 or 5: 13.47±2.75 years old; p=0.033). Participants with medium-to-high GCN of total C4 had a higher mean BMI than those with low total C4 GCN (p=0.03, table 2). Compared with participants with a low C4B GCN, those with a medium-to-high C4B GCN were more likely to have history of hypertension (p=0.02), a higher DBP (p=0.02) and a past history of pericarditis (p=0.031). Lipid profiles were similar between each GCN pair (low vs medium to high) as was baseline CRP. Individuals with cSLE and a GCN of C4A less than 2 were more likely to have a history of myositis than those with a C4A GCN of 2 or more (20.5% vs 7.59%; p=0.03).
A comparison of baseline laboratory and clinical data for patients with cSLE /APPLE between dichotomised GCN groups of total C4, C4A and C4B
Participants with medium-to-high GCNs of total C4 and C4B had significantly higher serum concentrations of serum C4 protein (P=1.2×10−5 for C4T and 0.01 for C4B). These patients were also slightly older than participants with low GCN of total C4 (P=0.02) and C4B (P=0.06), respectively. Serum C4 concentrations and age did not differ between C4A GCN groups. No significant differences in distribution of race or gender were observed when comparing participants based on GCNs of complement C4 and its isotypes.
CIMT measurements were similar in participants with low total C4 GCN and low C4B GCN compared with those with medium-to-high total C4 GCN and medium-to-high C4B GCN, respectively. Compared with participants with ≤2 C4A, those with >2 C4A had significantly higher mean–mean CIMT (0.463 vs 0.451 mm; P=0.04), mean–mean common CIMT (0.471 vs 0.455 mm; P=0.05), and mean-max common CIMT (0.603 vs 0.580 mm; P=0.03). Conversely, mean-max CIMT was similar between the two C4A groups (0.570 vs 0.590 mm; P=0.09).
No significant relationship was appreciated when comparing baseline CIMT measurements to baseline serum C3, C4 and CRP protein levels.
Complement profiles in hypertensive and normotensive participants
Hypertensive and normotensive participants had similar mean age and racial distribution (table 3). Those with hypertension had significantly higher mean values of BMI and body weight but not height (p=0.0046). Compared with normotensive participants, the frequencies of nephrotic syndrome or nephritis syndrome, and other renal involvement were dramatically higher in hypertensive participants (table 3). We also observed significant differences in baseline serum levels of complement C4 between hypertensive and normotensive participants (18.5±8.6 vs 13.5±6.7 mg/dL; P=4.7×10−6). Baseline serum C3 levels were significantly higher among hypertensive participants (110.7±26.4 vs 95.7±29.0 mg/dL, P=0.0003).
Baseline demographics and complement profiles of normotensive and hypertensive APPLE participants
Mean serum C4 and C3 levels over time in hypertensive and normotensive participants are shown in figure 2A, B. A history of hypertension was with higher serum mean C4 (P=5.0×10−25) and C3 levels (P=5.8×10−20) over time.

Serial serum C4 (panel a) and C3 (panel B) concentrations in APPLE participants with (red curve) and without (blue curve) a history of hypertension. Mean concentrations of serum C4 or C3 with standard errors were plotted against time (visit month). APPLE, Atherosclerosis Prevention in Pediatric Lupus Erythematosus.
To investigate the genetic basis for higher baseline and serial complement levels among hypertensive participants, we compared GCNs of total C4, C4A and C4B in the hypertensive and normotensive groups (table 3). Hypertensive participants demonstrated significantly higher mean C4B GCN (2.0±0.6 vs 1.8±0.7, P=0.023), and significantly lower mean C4A GCN (1.8±0.7 vs 2.1±0.8, P=0.032) than normotensive participants. Hypertensive participants had a higher C4S GCN (P=0.0054) and a lower mean C4L GCN (P=0.0098). Total C4 GCN was not significantly different between groups, nor were frequencies of fast and slow genotypes of C3.
We performed stepwise logistic regression analyses to identify independent risk factors for hypertension at baseline. As shown in part b of table 3, in the order of decreasing effects, nephrotic syndrome, nephritic syndrome, serum levels of complement C4, BMI and the GCN of long C4 genes were independent risk factors for hypertension (model P: 2.6×10–24; R2: 0.51; area under curve: 0.932).
Effects of complement C4 GCNs on serum complement level and response to atorvastatin treatment
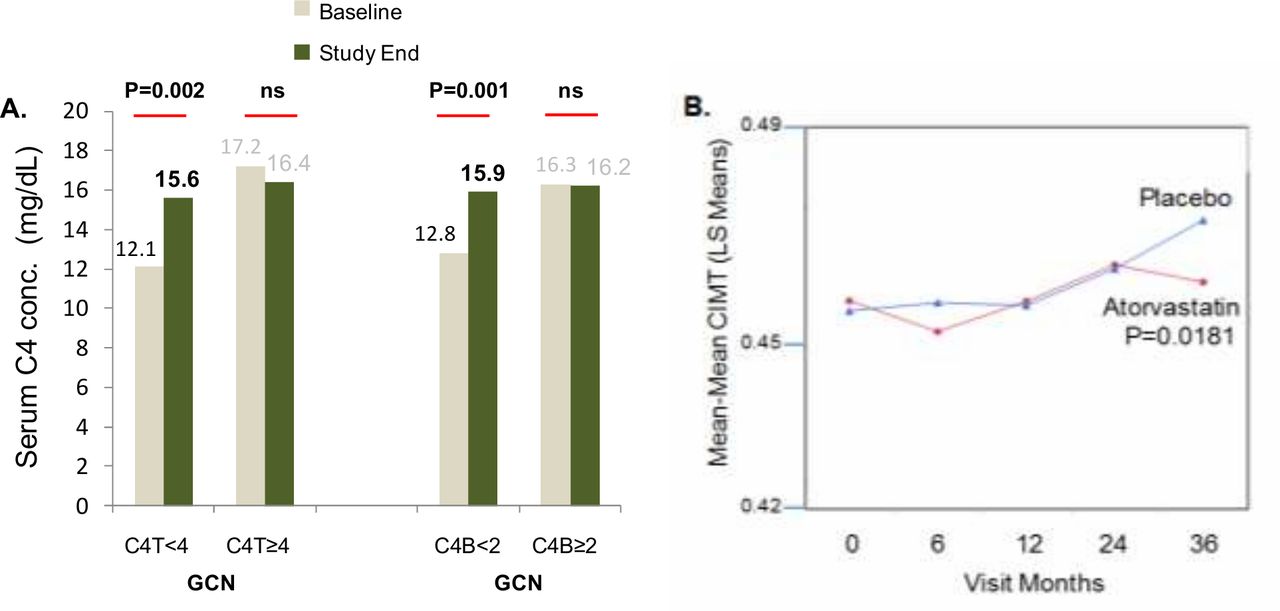
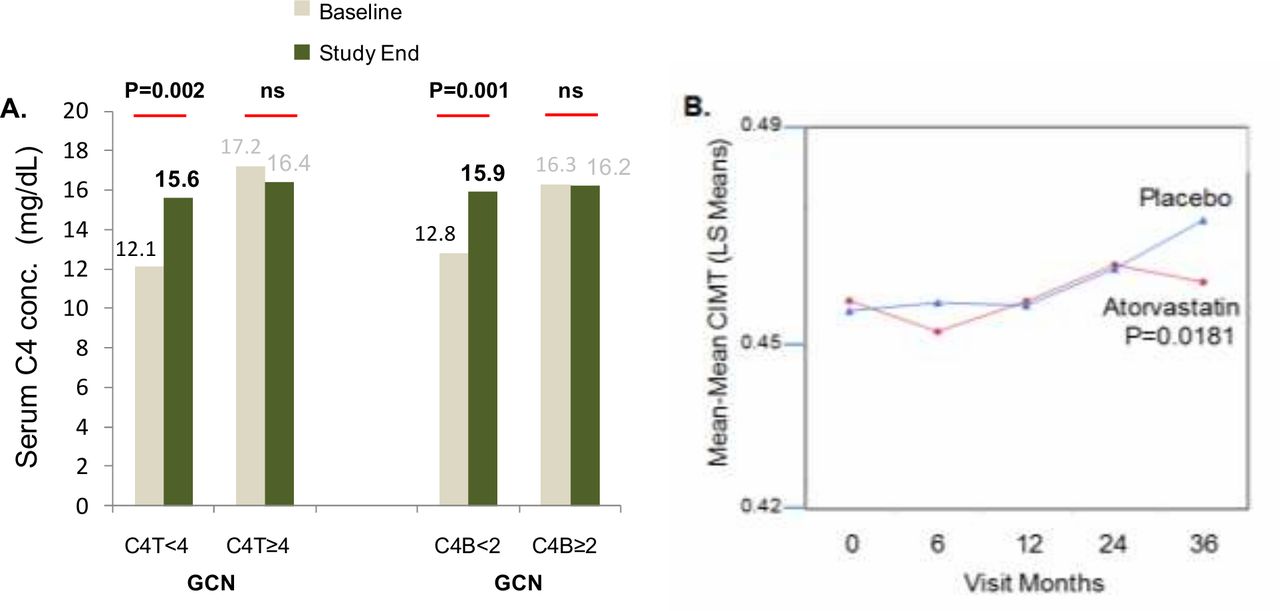
APPLE participants were randomised to receive either daily atorvastatin or placebo and monitored meticulously over the 3-year trial period. Overall, there were no significant differences in serum complement levels between placebo and atorvastatin groups at baseline and at study end. Participants were then dichotomised into low versus medium-to-high groups based on total C4 GCN and C4B GCN. Compared with participants in the medium-to-high groups, those with low GCNs of total C4 or C4B had lower mean serum levels of complement C4 at baseline (table 2). By the end of the trial, mean serum C4 protein levels had increased significantly in this low GCN group regardless of treatment (figure 3, panel A). In the medium-to-high GCN group, mean serum C4 levels remained stable over time. This would suggest that patients with low GCNs of total C4 or C4B benefited from the clinical trial process to normalise serum complement levels.
{kind=link}
{kind=link}
{kind=link}
Treatment effects of APPLE clinical trial. (A) improvement of mean serum C4 concentrations at the endpoint of APPLE trial among patients with low GCNs for total C4 (<4) or C4B (<2), irrespective of treatment with placebo or atorvastatin, when compared with C4 concentrations at baseline. (B) Slower progression of mean–mean CIMT in cSLE treated with atorvastatin (red) than placebo (blue) among patients with GCN of C4B≥2. APPLE, Atherosclerosis Prevention in Pediatric Lupus Erythematosus; CIMT, carotid intima media thickness; cSLE, childhood-onset systemic lupus erythematosus; GCN, gene copy number; NS, not significant.
As shown in figure 3, panel B, the medium-to-high C4B GCN group treated with atorvastatin demonstrated significantly slower mean–mean CIMT progression compared with participants who received placebo (P=0.018). While the mean serum C4 protein levels in the atorvastatin treatment group with C4B≥2 was slightly lower than that of the placebo group, the progression of changes was not significantly different between these two groups. There was also no significant difference in the rate of mean–mean CIMT progression between atorvastatin treatment and placebo groups over the 3-year trial in the low C4B GCN subset.
Discussion
Understanding that CVD is often subclinical in children with cSLE, we investigated the relationship between complement genetics and risk for CVD. Conceivably, patients with low serum complement levels at baseline would be more readily depleted during active disease. Given the linear relationship between total C4 GCN and serum C4 concentration demonstrated in our study, we propose that low total C4 GCN is an inherited unmodifiable risk factor that, on early identification, may trigger more intensive clinical monitoring.
Our results suggest that patients with cSLE with a medium-to-high C4B GCN more commonly have a history of hypertension and pericarditis. Additionally, these potentially ‘high-risk’ individuals who were in the treatment group of the APPLE trial demonstrated slower CIMT progression over the course of the trial. We also noted an association between low C4A GCN and myositis, an observation which was consistent with our earlier report on C4A deficiency in juvenile dermatomyositis.38
Importantly, we showed that APPLE participants with a history of hypertension had significantly higher serum concentrations of C4 and C3 at baseline and throughout the 36-month trial period than participants without a history of hypertension (figure 2). Elevated serum levels of complement have been described in people with CVD but, to our knowledge, this association has not previously been demonstrated in SLE or in children. This is the first study to analyse complement genetics and serial serum complement protein levels as a predictor of CVD in patients with cSLE. We leveraged data from the APPLE trial which was strengthened by its serial collection of CIMT and laboratory data in a cohort of racially and ethnically diverse children with SLE. The exclusion of patients with severe nephritis from this cohort reduced the confounding effects of kidney disease on hypertension in our analysis but also limited the generalisability of our findings to a cohort of patients with cSLE known to be highly affected by hypertension. In addition to inflammatory mechanisms, there are other factors thought to be associated with CVD in SLE such as the presence of antiphospholipid antibodies and vitamin D deficiency.9 We were able to consider CRP which has been proposed as an independent risk factor for CVD.39 While our study found no significant association between the levels of CRP and CIMT, further studies would be desirable to more thoroughly investigate various proposed risk factors for CVD. Among adult subjects with recurrent positivity of antiphospholipid antibodies, we observed that patients who experienced thromboses and/or recurrent pregnancy loss had significantly higher serum protein levels of complement C4 and C3 and higher GCN of C4B than patients who did not manifest antiphospholipid syndrome-related disorders.40
In view of the high CVD risk, it would be appropriate for patients with cSLE including those with hypertension, high C4B GCN, high serum levels of complement and a recurrent presence of antiphospholipid antibodies to receive routine cardiovascular risk assessment, and probably prophylactic therapy to ameliorate the progress of underlying disease. It remains to be established if and to what extent anti-inflammatory therapy would give additional benefit.
Our study was limited by the lack of data on steroid exposure and SLE disease activity. Furthermore, blood pressures measured in the APPLE trial were not performed in a highly standardised fashion. Next, our study relied on CIMT as a surrogate marker for atherosclerosis. This is a widely accepted measurement but there are novel measurements of arterial stiffness such as pulse wave velocity that could be explored in future studies. The post-hoc nature of our analysis is another limitation. Prospective analysis of patients with cSLE who fall into our ‘high-risk’ groups using standardised and repeat blood pressure measurements would help support our findings. Our findings regarding effective response to atorvastatin in individuals with medium-to-high C4B GCN were also limited by the relatively short follow-up time of the trial. Longer follow-up would be necessary to verify the effect of C4B GCN as it pertains to attenuation of CIMT progression.
In conclusion, serial serum C4 and C3 levels are remarkably higher in patients with cSLE with a history of hypertension than in those without. Individuals with ≥2 copies of C4B are more likely to have a history of hypertension, and progression of atherosclerosis among these subjects was attenuated when treated with atorvastatin compared with placebo. Knowledge of a patient’s complement genetic profile can be useful in risk stratification and therapy of CVD in SLE.
Acknowledgments
We are indebted to colleagues and patients engaged in the APPLE clinical trial. Results of article were partially presented at the 27th International Complement Workshop at Santa Fe, New Mexico (9/2018) and its abstract published at Molecular Immunology 2018; 102: 230-231.
References
Footnotes
Contributors SA, LES, EM and CYY conceived project. ST, SA, NS, DL, HB and LES examined and approved study protocol, provided APPLE repository genomic DNA and plasma samples, repository data and inputs on rheumatic disease studies. CYY, BZ, GRY, EHK and YLW designed and performed molecular genetics and immunology experiments. EM, SA, HNN and CYY conducted clinical, genetic and immunologic data analyses. EM, SA, HNN and CYY drafted the first version of the manuscript. All authors read and approved the final draft of the manuscript.
Funding This work was supported in parts by NIH/NIAMS grants 1R01 AR073311 and 1R21 AR070509 (CYY), and a Childhood Arthritis and Rheumatology Research Alliance (CARRA)-Arthritis Foundation Fellows Small Grant (EM). The APPLE clinical trial was supported by the NIH (National Institute of Arthritis and Musculoskeletal and Skin Diseases contract N01-AR-2-2265), the Edna and Fred L Mandel Jr Center for Hypertension and Atherosclerosis, and Pfizer, which provided atorvastatin and matching placebo. Dr Singer’s work was supported by the NIH (Clinical and Translational Science Award program grant UL1-RR-024989).
Competing interests The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Patient consent for publication Not required.
Ethics approval information This study was approved by Institutional Review Board at the Nationwide Children’s Hospital, the Data and Specimen Repository Review Committees of the APPLE clinical trial, and the CARRA Publication Committee in the USA.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Aggregate research data is presented in this manuscript. APPLE clinical trial data can be requested from the APPLE Data Committee.