Article Text

Abstract
Background Low C3 and lupus anticoagulant (LAC) are known risk factors for thrombosis in SLE. We evaluated the association between C4d products deposited on platelets (PC4d) and thrombosis in SLE. Antiphosphatidyl serine/prothrombin (PS/PT) complex antibody was also evaluated as an alternative to LAC.
Methods This was a cross-sectional analysis of 149 consented patients with SLE (mean age: 47±1 years, 86% female) classified with (n=16) or without (n=133) thrombotic events in the past 5 years. Abnormal PC4d (≥20 units) was measured using flow cytometry. LAC and C3 were measured using dilute Russell’s viper venom time (>37 s) and immunoturbidimetry, respectively. Anti-PS/PT antibody status (IgG) was measured by immunoassay. Statistical analysis consisted of logistic regression and calculation of OR estimates with 95% CI.
Results Abnormal PC4d (OR=8.4, 95% CI 2.8 to 24.8), low C3 (OR=9.5, 95% CI 3.0 to 30.3), LAC (OR=5.4, 95% CI 1.3 to 22.3) and anti-PS/PT IgG (OR=3.4, 95% CI 1.2 to 9.7) status associated with thrombosis (p<0.05). Cumulatively, the presence of PC4d, low C3 and LAC abnormalities as a composite risk score was higher in the presence of thrombosis (1.93±0.25) than in its absence (0.81±0.06) (p<0.01). Each unit of this composite risk score yielded an OR of 5.2 (95% CI 2.5 to 10.7) to have thrombosis (p<0.01). The composite risk score with anti-PS/PT antibody status instead of LAC also associated with thrombosis (p<0.01).
Conclusion A composite risk score including PC4d, low C3 and LAC was associated with recent thrombosis and acknowledges the multifactorial nature of thrombosis in SLE.
- systemic lupus erythematosus
- thrombosis
- complement
- lupus anti-coagulant
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The excessive risk of thrombosis in SLE is dependent on the presence of abnormalities that are specific for the disease, including low C3, antiphospholipid (aPL) antibodies (in particular lupus anticoagulant [LAC]) and nephrotic syndrome.1 Other factors related to SLE treatment such as prednisone may further elevate the risk of thrombosis.1 2
Cell-bound complement activation products (CB-CAPs) and deposition of C4d split fragments on haematopoietic cells such as B lymphocytes (BC4d) and erythrocyte (EC4d) are commonly present in SLE.3 4 In contrast, deposition of C4d on platelets (PC4d) is generally uncommon (20% SLE) but highly specific.5
Several groups have reported that abnormal PC4d associates with mortality and thrombosis in SLE.6–8In this study, we evaluated the relationships between PC4d and thrombosis in SLE, and built a composite score for thrombosis risk of PC4d, low C3 and LAC. Because of the difficulty in performing and interpreting the LAC assay in anticoagulated patients, we also looked at antiphosphatidyl serine/prothrombin (PS/PT) complex antibody as an alternative to LAC.9
Methods
Patients
This was a cross-sectional study designed to evaluate the association between complement abnormalities and a history of thrombosis in patients with SLE, all enrolled at a single lupus centre in the Baltimore area (Hopkins Lupus Center). All patients with SLE fulfilled the 2012 Systemic Lupus International Collaborating Clinics classification criteria for SLE.10 Thrombosis that occurred in the past 5 years was classified as any thrombosis, venous thrombosis or arterial thrombosis, as described.11 Disease activity was assessed using the Physician Global Assessment (PGA) on a 0-point to 3-point Visual Analogue Scale and the Safety of Estrogens in Lupus Erythematosus National Assessment (SELENA) Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) without anti double-stranded DNA (anti-dsDNA) and complement components as described (clinical SELENA-SLEDAI).4 Active disease status was defined as a clinical SELENA-SLEDAI greater or equal to 4 points.
Laboratory markers
Whole blood and serum were collected in EDTA-containing and serum separator tubes, respectively, and routed overnight to the reference clinical laboratory at Exagen (using transportation kit equipped with coolant cartridge). EC4d and BC4d levels were measured using fluorescence-activated cell sorting (FACS) as described,12 and expressed as net mean fluorescence intensity (MFI). PC4d levels were also measured by FACS as follows: red blood cells from EDTA whole blood were lysed and platelets were stained using mouse monoclonal antibody against human C4d (Quidel, San Diego, California), or alternatively using mouse IgG1 kappa monoclonal (MOPC-21), isotype control. After incubation for 30 min at 2°C–8°C, samples were stained using goat antimouse conjugated to Fluorescein Isothiocyanate (FITC) (30 min at 2°C–8°C in the dark). A monoclonal antibody against human CD42b conjugated to phycoerythrin (PE) (platelet-specific marker) was used to identify C4d complement activation fragment covalently bound to the platelets. FACS analysis was performed using a Gallios (10-colours) flow cytometer (Beckman Coulter, Brea, California) equipped with a CXP software to measure fluorescent staining intensity. Light scatter (forward and side) gating parameters were used during acquisition to isolate the platelet population, followed by secondary gating based on positive CD42b PE staining. Quantification of the non-specific (isotype control) and specific (C4d) fluorescence in the FL1 (fluorescein isothiocyanate) channel was determined for the CD42b PE gated platelet cells (5000 events). Net MFI was determined by subtraction of isotype control background MFI results from the specific C4d MFI results on gated platelet cells. Abnormal EC4d, BC4d and PC4d status corresponded to levels greater than the 99th percentile of normal healthy group (>14, >60 and >20 net MFI, respectively).3 Abnormal PC4d yielded specificity greater than 95% in distinguishing SLE from rheumatoid arthritis (98%), primary Sjogren’s (98%) and fibromyalgia (100%) (data not shown).
ANA status was determined using digital imaging on NOVA View (≥1:80 as positive) (INOVA Diagnostics, San Diego, California). Antibody titres to dsDNA were measured using chemiluminescence immunoassays (QUANTA Flash, INOVA Diagnostics). Low C3 or C4 status was established using serum C3 (<81.1 mg/dL) and C4 (<12.9 mg/dL) levels all measured using immunoturbidimetry (Optilite, Binding Site, San Diego, California). LAC was measured at the Hopkins Lupus Center using the dilute Russell’s viper venom time (dRVVT >37 s) as per the recommendation of the Scientific and Standardisation Committee of the International Society on Thrombosis and Haemostasis.13 Anticardiolipin, antibeta2 glycoprotein 1 antibody (IgM, IgG and IgA isotypes) and anti-PS/PT complex antibodies (IgM and IgG) were measured using immunoassays (INOVA Diagnostics). Manufacturer cut-offs were used for all assays. Triple positivity for aPL antibodies (abnormal dRVVT and presence of cardiolipin and beta2 glycoprotein 1 antibodies [IgM, IgG or IgA]) was measured for all subjects. The site investigator (MAP) was blinded to all CB-CAPs throughout the study, and testing personnel was blinded to clinical status.
Statistical analyses
The association of a history of thrombosis (venous, arterial or any thrombosis) in the past 5 years with the laboratory measures was assessed using positive and negative likelihood ratio and OR, all reported with 95% CI. Univariate and multivariate logistic regression tests with thrombosis as the dependent variable and the biomarkers as independent predictors were used. The cumulative presence of abnormalities in composite scores was calculated and the Odds Ratio (OR) for thrombosis (per unit change) was calculated. Differences between models were estimated using minimum Akaike information criterion (AIC). Mann-Whitney and χ2 tests were employed as appropriate.
Results
The study enrolled 149 consecutive patients with SLE (mean 48.3 years, 83% ANA-positive [>1:80]). Sixteen of them (10.7%) had a history of thrombosis (venous or arterial) in the past 5 years. Venous thrombosis occurred in 10 patients (inclusive of 8 deep vein thrombosis/pulmonary embolism and 2 superficial thrombosis); arterial thrombosis occurred in 8 patients (inclusive of 3 myocardial infarctions, 2 cerebrovascular accidents, 1 digital gangrene and 2 other arterial events). Two patients experienced both venous and arterial events. Patient characteristics are presented in table 1.
Patient characteristics in the presence or absence of any thrombosis (venous or arterial)
In this cohort of 149 patients, BC4d status was unavailable in nine patients due to low B cell events (<200) collected on the flow cytometer. C3/C4 was not available in one patient. Among 140 patients with C3, C4, EC4d and BC4d status available, a 21.4% higher proportion of SLE were positive for abnormal EC4d or BC4d (42.9%, n=60/140) than for low C3 or C4 (21.4%, n=30/140) (p<0.01).
A significantly lower frequency of thrombosis was observed in Caucasians (25% vs 59%; p=0.009) compared with other ethnic groups. African–Americans (32% vs 50%; p=0.19) tended to have a higher frequency of thrombosis. Current prednisone treatment was also associated with a higher frequency of thrombosis (56% vs 32%). Patients taking prednisone were 3.1-fold more likely (OR=3.0, 95% CI 1.1 to 9.0) (p=0.029) to have had thrombosis than those not taking prednisone. Other demographic variables, including active disease status (OR=2.2, 95% CI 0.7 to 7.3) (p=0.18), did not associate with thrombosis.
The frequency of laboratory abnormalities, overall and by the presence of thrombosis (any thrombosis, venous thrombosis or arterial thrombosis), is highlighted in table 2. Low C3, low C4, abnormal EC4d, PC4d, anti-PS/PT IgG and LAC status all significantly associated with any thrombosis (p<0.05). The incidence of triple positivity for aPL antibodies was higher in patients with thrombosis (25%) than without (16.4%) but did not reach statistical significance (p=0.39).
Laboratory measures in the presence or absence of any thrombosis (venous or arterial)
The median (IQR) EC4d and PC4d levels were 2.2-fold and 5.5-fold higher, respectively, in the presence of thrombosis (20 net MFI [IQR: 9–59] and 27 net MFI [IQR:9–79], respectively) than in its absence (9 net MFI [IQR: 6–19] and 5 net MFI [IQR:2–14], respectively) (p<0.01). BC4d levels were slightly elevated in the presence of thrombosis (median 46 net MFI [IQR: 26–74] compared with 29 net MFI [IQR: 17–62]), but the difference was not significant (p=0.27).
Online supplementary tables 1 and 2 highlight the associations between the laboratory measures and venous or arterial thrombosis. Low C3 and abnormal PC4d status associated with venous thrombosis (OR=10.5 [95% CI 2.8 to 39.5] and 19.2 [95% CI 4.2 to 84.7], respectively) (p<0.05) and arterial thrombosis (OR=5.4 [95% CI 1.28 to 23.17] and OR=4.0 [95% CI 1.0 to 15.8], respectively) (p<0.05). All patients with venous thrombosis tested positive for LAC (OR=+∞ [95% CI 1.3 to +∞], 100% sensitive), but LAC did not associate specifically with arterial thrombosis (OR=2.10 [95% CI 0.5 to 9.4], p=0.37). This contrasted with anti-PS/PT IgG status, which associated with arterial thrombosis (OR=5.4 [95% CI 1.3 to 21.9], p=0.02), but not venous thrombosis (OR=2.10 [95% CI 0.6 to 7.3], p=0.30). Anticardiolipin antibodies were not associated with thrombosis, while antibeta2 glycoprotein 1 antibodies (IgG and IgA isotype) associated with arterial thrombosis. Triple positivity for aPL antibodies was higher in patients with arterial thrombosis (37.5%) than without arterial thrombosis (16.2%) (p=0.12) but was not associated with venous thrombosis (20.0% vs 17.2%; p=0.81).
Supplemental material
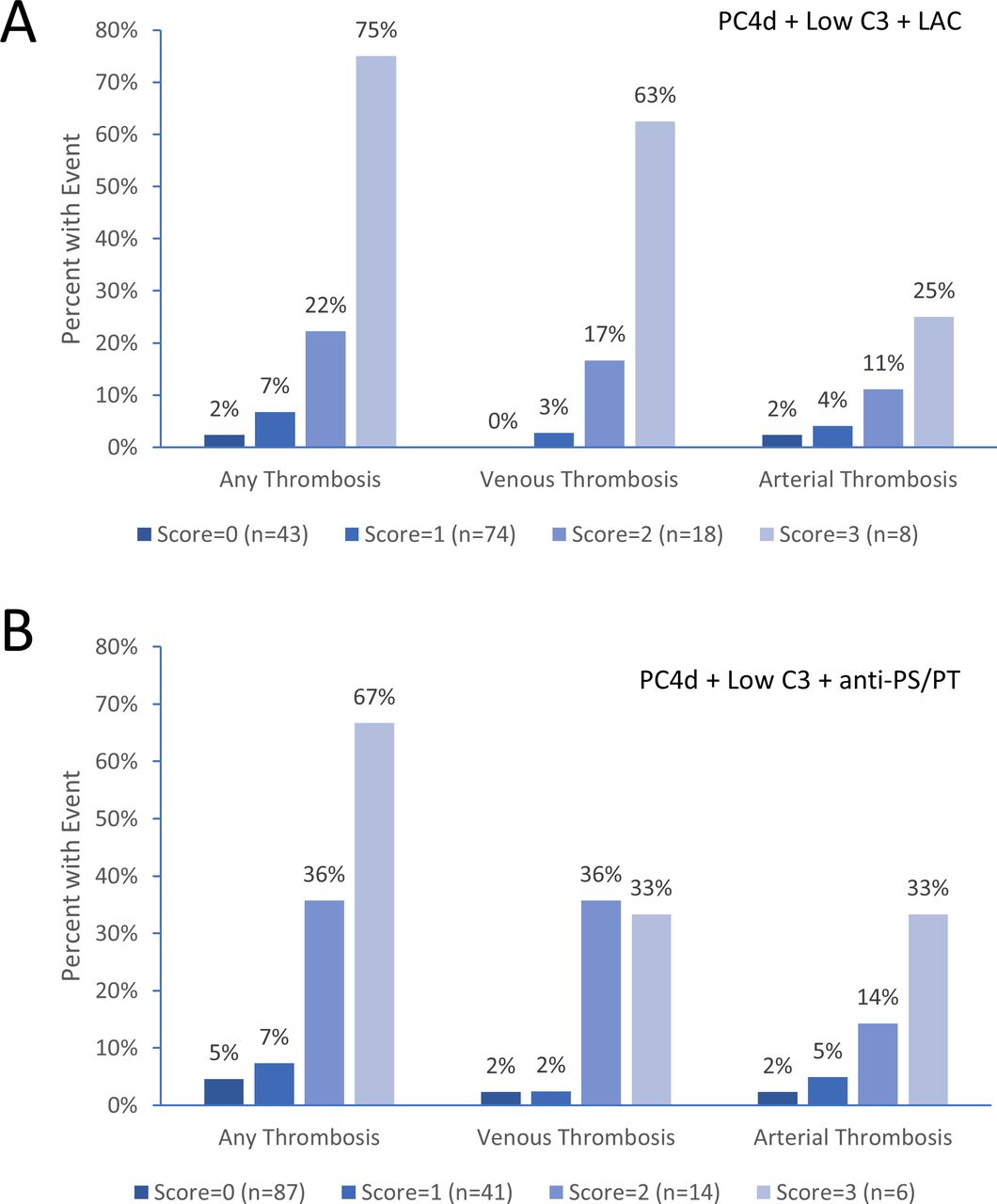
In 143 patients with PC4d, low C3 and LAC status available, multivariate logistic regression analysis revealed that abnormal PC4d (adjusted OR=4.2 [95% CI 1.1 to 16.0], p=0.04), low C3 (adjusted OR=6.20 [95% CI 1.3 to 29.6], p=0.02) and LAC (adjusted OR=7.0 [95% CI 1.3 to 38.5], p=0.02) were all significantly and independently associated with any thrombosis, thus indicating additive utility of the three markers in combination. Cumulatively, the presence of PC4d, low C3 and LAC abnormalities as a composite risk score was higher in the presence of thrombosis (1.93±0.25) than in its absence (0.81±0.06) (p<0.01). Each unit of this composite risk score yielded an OR of 5.2 (95% CI 2.5 to 10.7) to have thrombosis (p<0.01, AIC=78.94) (figure 1A). The average composite risk score was also higher in the presence of venous thrombosis (2.30±0.26, n=10) than in its absence (0.83±0.06, n=133) (p<0.001), and each unit of the score yielded an OR of 8.30 (95% CI 3.16 to 21.83) for venous thrombosis (p<0.01, AIC=49.48). The composite risk score was also higher in the presence (1.62±0.37, n=8) of arterial thrombosis than in its absence (0.90±0.07, n=135) (p=0.05), and each unit of the score yielded an OR of 2.57 (95% CI 1.17 to 5.64) for arterial thrombosis (AIC=60.27, p=0.02). Table 3 and online supplementary figure 1 highlight the performance of other risk score combinations. PC4d, low C3 and LAC in combination yielded lower AIC for any thrombosis (78.94) and venous thrombosis (49.48) compared with other models.

{kind=link}
Composite score of risk factors and thrombosis. Per cent of patients with any thrombosis, venous thrombosis and arterial thrombosis is given. The composite score (range 0–3) corresponds to the number of abnormalities present at the time of specimen collection. (A) Abnormal PC4d (>20 net MFI), low C3 (<81 mg/dL) and LAC (dRVVT >37 s) (n=143). (B) Abnormal PC4d (>20 net MFI), low C3 (<81 mg/dL) and anti-PS/PT IgG (>30 units) (n=148). dRVVT, dilute Russell’s viper venom time; LAC, lupus anticoagulant; MFI, mean fluorescence intensity; PC4d, platelets C4d; PS/PT, phosphatidyl serine/prothrombin.
Markers and composite score in association with thrombosis
Anti-PS/PT IgG as an alternative to LAC (n=148 patients) in composite risk score also yielded higher score in the presence versus the absence of any thrombosis (1.56±0.29 [n=16] vs 0.47±0.06 [n=132]) (p<0.001), venous thrombosis (1.70±0.25 [n=10] vs 0.51±0.06 [n=138]) (p<0.001) and arterial thrombosis (1.50±0.25 [n=8] vs 0.53±0.06 [n=140]) (p=0.02). The OR for any thrombosis was 3.60 (95% CI 1.98 to 6.53) (p<0.01, AIC=84.95), the OR for venous thrombosis was 3.65 (95% CI 1.83 to 7.27) (AIC=62.15), and the OR for arterial thrombosis was 2.79 (95% CI 1.38 to 5.65) (AIC=58.18) (figure 1B). PC4d, low C3 and anti-PS/PT in combination as composite risk score yielded a lower AIC (58.18) for arterial thrombosis than any of the other marker combinations (table 3).
There was also a higher incidence of low C3 (26% vs 8%; p=0.001), low C4 (37% vs 12%; p=0.001), abnormal EC4d (59% vs 27%; p=0.001), PC4d (37% vs 18%), BC4d (59% vs 27%; p=0.08) and anti-dsDNA (48% vs 25%; p=0.01) among patients with SLE presenting with active compared with inactive disease status (clinical SELENA-SLEDAI ≥4 points). However, multivariate analysis with three CB-CAP abnormalities revealed that only EC4d status (OR=3.5, 95% CI 1.2 to 10.2) (p=0.023) associated with active disease (BC4d: OR=1.2 [95% CI 0.4 to 3.3] and PC4d: OR=1.3 [95% CI 0.4 to 4.0]) (p>0.66). aPL antibodies were generally not associated with active disease status (p≥0.05; data not shown).
Discussion
SLE is an immune complex disease linked to classical complement pathway activation, hyperconsumption of C3 and C4 proteins, and production of C4d split fragments covalently bound to a variety of haematopoietic cells, including the erythrocytes, the B lymphocytes and the platelets. The complement system, platelets and coagulation pathways interact. This is the first report of a composite risk index which includes measures of these pathways and which highlights the additive association with thrombosis in SLE.
PC4d yielded an OR of 8.4 for any thrombosis, and the association of the marker for venous thrombosis was stronger (OR=19.2) than for arterial events (OR=4.0), a finding in agreement with those reported by Lood et al,6 who also found stronger association of PC4d with venous than with arterial thrombosis. In this study, 20% of patients with SLE presented with abnormal C4d deposition on platelets (PC4d), a finding consistent with a previous report and the low sensitivity of the marker for SLE overall.5 Among CB-CAPs, PC4d is known to have the highest level of specificity for SLE. The data presented here (1) suggest that PC4d is a prognostic marker associating with thrombosis, and (2) add to our understanding that the complement system and platelets are intimately linked and cooperate in the development of venous and arterial thrombosis. In contrast, abnormal BC4d status was not associated with vascular events, and the weak contribution of EC4d status to thrombosis was negligible, after adjusting for the presence of PC4d.
LAC was a sensitive marker for thrombosis (75% for venous and 100% for arterial), yielding an OR of 5.4 for any thrombosis. However, the statistically significant impact of LAC on thrombosis was restricted to venous events. This contrasted with anti-PS/PT antibody status (IgG isotype) that associated with arterial but not venous thrombosis. While it is tempting to suggest that LAC and anti-PS/PT may have different selectivity for venous and arterial thrombosis, larger studies will be required. Triple positivity for LAC, beta2 glycoprotein 1 and anticardiolipin antibodies also tended to associate with thrombosis, and the lack of significance in our study may reflect the low number of subjects enrolled as well as the cross-sectional design of the study. It will be important to evaluate the association between aPL antibodies and thrombosis at follow-up visits.
In this cohort, low C3 was the strongest risk factor for any thrombosis (OR=9.5) and associated with both venous (OR=10.5) and arterial thrombosis (OR=5.4). Clinical activity (PGA or SLEDAI), in contrast, was not associated with thrombosis.
We conducted a multivariate analysis and combined the presence of low C3, PC4d and LAC to produce a composite score of risk factors for thrombosis. Independently, each of the three markers was significantly associated with thrombosis (adjusted OR ranging from 4.2 to 7.0), thus indicating additive value. We also estimated the value of anti-PS/PT as an alternative to LAC. While a lower OR (3.6 vs 5.2 per unit change) was observed with anti-PS/PT, both composite scores with LAC or anti-PS/PT (as an aPL alternative) associated with venous and arterial thrombosis.
Prednisone was also associated with thrombosis, and these data are consistent with the elevated risk of thrombosis and increased damage in SLE. Hydroxychloroquine was prescribed to the vast majority of subjects and was not associated with a lower incidence of thrombosis. We have previously reported a dose-dependent association of prednisone with cardiovascular events in SLE.1 While this is not completely understood, prednisone does increase factor VIII levels, decreases fibrinolysis and produces abnormal von Willebrand factor multimer composition.2
We acknowledge that there are limitations to our study. First, the number of thrombotic events was small and larger cohorts will be required to confirm the thrombosis risk equation. Second, the thrombosis risk equation was established retrospectively, the study was cross-sectional, and it is not known whether higher scores translate to higher incidence of thrombosis in future follow-ups. Our results will need to be confirmed prospectively. However, collectively, these data as well as data from others strongly support the value of PC4d in associating with thrombosis. Both the composite risk score and the individual markers may be of value in clinical practice to identify patients likely to benefit from interventions, including hydroxychloroquine therapy, that can significantly reduce the risk of thrombosis in SLE.14 15
In conclusion, a composite thrombosis risk equation including PC4d, low C3 and LAC strongly associates with thrombosis in SLE. This composite score of risk factors performed better than single risk factors alone.
Acknowledgments
We thank Robert Apilado, Jo-Anne Ligayon, Leilani Wolover and Kelley Brady for technical assistance. We also thank Claudia Ibarra for the management of our clinical laboratory and Dr Roberta Alexander for clinical research support.
References
Footnotes
Contributors MAP and TD designed the study. TD performed the analysis and wrote the first draft of the manuscript. JC performed flow cytometry and clinical data management. TO'M participated in flow cytometry data acquisition. All authors approved the final manuscript.
Funding The study is funded by Exagen. The Hopkins Lupus cohort is supported by NIH grants R01 AR43727 and AR69572.
Competing interests MAP has received research grants from Exagen. TD JC and TO’M are employed by Exagen Diagnostics.
Patient consent for publication Obtained.
Ethics approval The Johns Hopkins University School of Medicine internal review board approved the study and informed consent was collected from all subjects.
Provenance and peer review Not commissioned; externally peer reviewed.