Article Text

Abstract
Objective To define the SLE phenotype associated with pulmonary hypertension using multiple autoantibodies.
Methods 207 (8%) patients with SLE with pulmonary hypertension, defined as a right ventricular systolic pressure greater than 40 mm Hg on transthoracic echocardiogram or as pulmonary artery dilatation on CT of the chest, were identified from the Hopkins Lupus Cohort (94.2% female; 56.5% African–American, 39% Caucasian; mean age 45.6 years). 53 patients were excluded from the clustering analysis due to incomplete autoantibody profiles. Agglomerative hierarchical clustering algorithm with Ward’s method was used to cluster the patients with pulmonary hypertension, based on their autoantibodies. Autoantibodies used in the clustering analysis included lupus anticoagulant, anticardiolipin, anti-beta 2 glycoprotein I, antidouble-stranded DNA, anti-Sm (anti-Smith), antiribonucleoprotein, false positive-rapid plasma reagin, anti-Ro, anti-La and hypocomplementaemia (C3 ever low or C4 ever low). The Dunn index was used to internally validate the clusters. Bootstrap resampling derived the mean Jaccard coefficient for each cluster. All analyses were performed in R V.3.6.1 using the packages cluster, fpc and gplots.
Results A significantly higher prevalence of pulmonary hypertension in African–American patients with SLE, compared with Caucasian patients with SLE (11.5% vs 5.9%, p<0.0001), was found. Based on equivalent Dunn indices, the 154 patients with SLE-associated pulmonary hypertension with complete autoantibody data were divided into five clusters, three of which had mean Jaccard coefficients greater than 0.6. Hypocomplementaemia, renal disorder and age at diagnosis significantly differed across clusters. One cluster was defined by antiphospholipid antibodies. One cluster was defined by anti-Ro and anti-La. One cluster had low frequencies of all antibodies.
Conclusion SLE-associated pulmonary hypertension disproportionately affects African–American patients. Pulmonary hypertension in SLE is defined by five autoantibody clusters. Antiphospholipid antibodies, anti-Ro and anti-La positivity, serological activity, and age at pulmonary hypertension diagnosis significantly differed across clusters, possibly indicating different pathophysiological mechanisms.
- Autoantibodies
- Systemic Lupus Erythematosus
- Cardiovascular Disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Pulmonary hypertension is an important potential complication of connective tissue diseases1 and a leading cause of death in SLE.2–6 A dilated pulmonary artery on chest CT7 or an elevated right ventricular systolic pressure on transthoracic echocardiogram is suggestive of pulmonary hypertension, especially in patients with connective tissue diseases such as scleroderma, in whom the use of echocardiography for diagnosing and monitoring pulmonary hypertension has been validated.8 9 Right heart catheterisation is required to confirm a diagnosis of pulmonary hypertension and aids in WHO pulmonary hypertension group classification. Unlike in scleroderma, there are no guidelines for screening or monitoring pulmonary hypertension in SLE. This is in part because pulmonary hypertension pathogenesis, prevalence, risk factors and natural history in SLE remain poorly understood.
SLE-associated pulmonary hypertension prevalence and serological and clinical associations vary by geographical location.10 11 For example, there is a pulmonary hypertension prevalence of 2% in a Taiwanese SLE cohort12 but 23% in a Pakistani SLE cohort.13 Prabu et al14 found an association of pulmonary hypertension with lupus anticoagulant in an SLE cohort in the UK while associations with antiribonucleoprotein (anti-RNP)15 and anticardiolipin antibodies16 have been reported in Chinese SLE cohorts. Anti-Ro and anti-La have been associated with pulmonary hypertension in a French SLE cohort.5 The REVEAL (Registry to Evaluate Early And Long-term Pulmonary Arterial Hypertension disease management) cohort, which included 1892 US patients with 1-year survival data, 339 of whom had systemic sclerosis, and 110 of whom had SLE, demonstrated a significant ethnicity difference comparing scleroderma-associated pulmonary hypertension versus SLE-associated pulmonary hypertension: Caucasian (84% vs 37%), African–American (11% vs 32%) or Hispanic (4% vs 18%) (p<0.0001).17 Generally, African–American patients with pulmonary hypertension have a higher mortality than Caucasian patients with pulmonary hypertension,18 such that these differences in prevalence across connective tissue diseases imply a potentially important health disparity.
Several autoantibodies are associated with pulmonary hypertension in SLE, including anticardiolipin,19 20 anti-beta 2 glycoprotein,19 anti-RNP,4 10 15 21 anti-Sm (anti-Smith),21 22 anti-Ro10 15 22 and anti-La.5 22 Hypocomplementaemia has also been associated with pulmonary hypertension in SLE.15 Antiendothelial cell antibodies are elevated in patients with SLE with pulmonary hypertension.23
Simonson et al24 found an association of pulmonary hypertension with low SLE disease activity in a US SLE cohort which has been confirmed in several cohorts, including a Chinese SLE cohort.10 Even in those with low SLE disease activity, however, the development of pulmonary hypertension imparts a significant mortality risk.25
SLE-associated pulmonary hypertension has at least three treatment subgroups, namely (1) response to immunosuppression26; (2) response to vasodilator therapy27; and (3) response to combination therapy.28 Sanchez and colleagues26 found that about 40% of patients with SLE-associated pulmonary hypertension responded to immunosuppression which suggests that some SLE-associated pulmonary hypertension has an inflammatory component that may be cytokine-mediated and autoantibody-mediated.29 Sun et al30 reported findings of a clustering analysis, showing that SLE-associated pulmonary hypertension could be divided into ‘vasculitic’ and ‘vasculopathic’ subtypes, which cluster with clinical findings of high SLE disease activity and poorer 3-year survival, versus low SLE disease activity and better prognosis, respectively.
SLE-associated pulmonary hypertension onset is often insidious and has no established clinical biomarker or screening protocol, making it difficult to predict and diagnose.31 In this study, we used the statistical technique of cluster analysis to identify groups of patients with SLE-associated pulmonary hypertension with similar autoantibody and complement patterns. We hypothesised that the cluster analysis would define unique pulmonary hypertension phenotypes in our SLE cohort. Cluster analyses can help to drive future investigations into risk factors and mediators of disease to better target therapeutic approaches.
Patients and methods
All patients who previously consented to participate in the Hopkins Lupus Cohort study were included. The cohort comprises patients with SLE, based on either the revised American College of Rheumatology (ACR) classification criteria or the Systemic Lupus International Collaborating Clinics (SLICC) classification criteria.32–34 All patients were followed up prospectively at quarterly intervals, beginning at the time of entry into the cohort. Clinical features, serological data and damage accrual data were recorded at the time of entry into the cohort and were updated at subsequent visits.
Pulmonary hypertension was defined as either a right ventricular systolic pressure of greater than or equal to 40 mm Hg on transthoracic echocardiogram or as pulmonary artery dilatation on chest CT. There were not sufficient data to further classify patients by WHO group.
Laboratory tests
Baseline immunological tests for 11 autoantibodies were performed at the first cohort visit. They included detection of antidouble-stranded (anti-dsDNA) by Crithidia assay; detection of anti-Ro, anti-La, anti-Sm and anti-RNP; lupus anticoagulant by dilute Russell’s viper venom time and confirmatory tests; and determination of IgG/IgM anticardiolipin by ELISA. Before May 1999, the Ouchterlony double diffusion assay was performed for the detection of Ro, La, Sm and RNP antibodies. Subsequently, ELISA was used for detection of Ro, La, Sm and RNP antibodies in patients enrolled after May 1999. The ELISA kits used were QUANTA Lite SS-A, QUANTA Lite SS-B, QUANTA Lite Sm and QUANTA Lite RNP (all from Inova Diagnostics, San Diego, California). The QUANTA Lite SS-A ELISA detects both 60 kd and 52 kd Ro antigens, but does not allow differentiation of the two Ro antigens. The kits used for detection of anticardiolipin were anticardiolipin IgG, anticardiolipin IgM and anticardiolipin IgA (all from Inova Diagnostics). IgG anticardiolipin levels >10 IgG phospholipid units and IgM anticardiolipin levels of >10 IgM phospholipid units were considered positive.
Statistical analysis
The 11 autoantibodies used in the clustering analysis included lupus anticoagulant, anticardiolipin, anti-beta 2 glycoprotein I, anti-dsDNA, anti-Sm, anti-RNP, false positive-rapid plasma reagin (RPR), anti-Ro, anti-La and hypocomplementaemia (C3 ever low or C4 ever low). An agglomerative hierarchical clustering algorithm with Ward’s method was applied to the autoantibody profiles of patients with lupus-associated pulmonary hypertension to determine the number of groups (clusters) with phenotypically similar profiles. Categorical variables were then assigned to each cluster.35
The Dunn index was used to internally validate the clusters. Bootstrap resampling with 1000 iterations was performed to derive the mean Jaccard coefficient over all iterations for each cluster with the cohort divided into three, four or five clusters. After clustering, associations between final clusters and patient characteristics were assessed by one-way analysis of variance for continuous variables and by Fisher’s exact test for categorical variables. Statistical analyses were performed in R version 3.6.1 using packages cluster, fpc and gplots.
In order for a patient with SLE to be eligible for the cluster analysis, information for all 11 selected autoantibodies (anti-dsDNA, anti-Ro, anti-La, anti-Sm, anti-RNP, lupus anticoagulant, IgG/IgM anticardiolipin, anti-beta 2 glycoprotein I, C3, C4, false positive-RPR) had to be available. Fifty-three patients with SLE were excluded from the clustering analysis for this reason. Excluded patients were often missing anti-beta 2 glycoprotein I, as it was not available in the early cohort years.
Results
A total of 207 patients with pulmonary hypertension were identified from the Hopkins Lupus Cohort (8% of the cohort) and were included in the analysis (53 patients were excluded because their autoantibody profiles were incomplete). The presence of revised ACR classification criteria were documented for all 207 patients with pulmonary hypertension, with 51% malar rash, 28% discoid rash, 50% photosensitive rash, 53% oral ulcer, 80% arthritis, 69% serositis, 60% renal disorder, 13% neurological disorder, 81% haematological disorder, 91% immunological disorder and 99% ANA positivity.32 33 Additional SLICC classification criteria included 27% direct Coombs test, 68% low C3, 59% low C4 and 17% low CH50.34
Table 1 shows the patient demographics in the Hopkins SLE cohort by presence of pulmonary hypertension. The mean±SD age of the patients at pulmonary hypertension diagnosis was 45.6±15.0; 94.2% were female; 56.5% were African–American, 2.9% were Asian and 39.1% were Caucasian; and 45% had a history of smoking. A significantly higher prevalence of pulmonary hypertension in African–American patients, compared with Caucasian patients (11.5% vs 5.9%, p<0.0001), was found. There was no significant difference in the prevalence of pulmonary hypertension by sex (5.9% male vs 8.2% female, p=0.2831). Of the 207 patients with SLE with pulmonary hypertension, 12 subjects had end-stage renal disease, 26 subjects had cardiomyopathy, 38 subjects had a diagnosis of cutaneous vasculitis, 108 subjects had a diagnosis of Raynaud’s phenomenon, and 29 subjects had pulmonary fibrosis prior to the diagnosis of pulmonary hypertension.
Pulmonary hypertension prevalence by demographics of patients with SLE
Autoantibody clusters
The Dunn index was 0.32 for three, four and five clusters. Dividing the cohort into five clusters produced a highly stable cluster 3 (mean Jaccard coefficient of 0.92). Clusters 1 and 5 were also stable with mean Jaccard coefficients greater than 0.6 (stable 0.71 and 0.63, respectively). Clusters 2 and 4 had lower mean Jaccard coefficients, indicating that these clusters were less stable. Using five clusters generated the highest number of stable clusters (compared with using three or four clusters), with a mean Jaccard coefficient greater than 0.6.
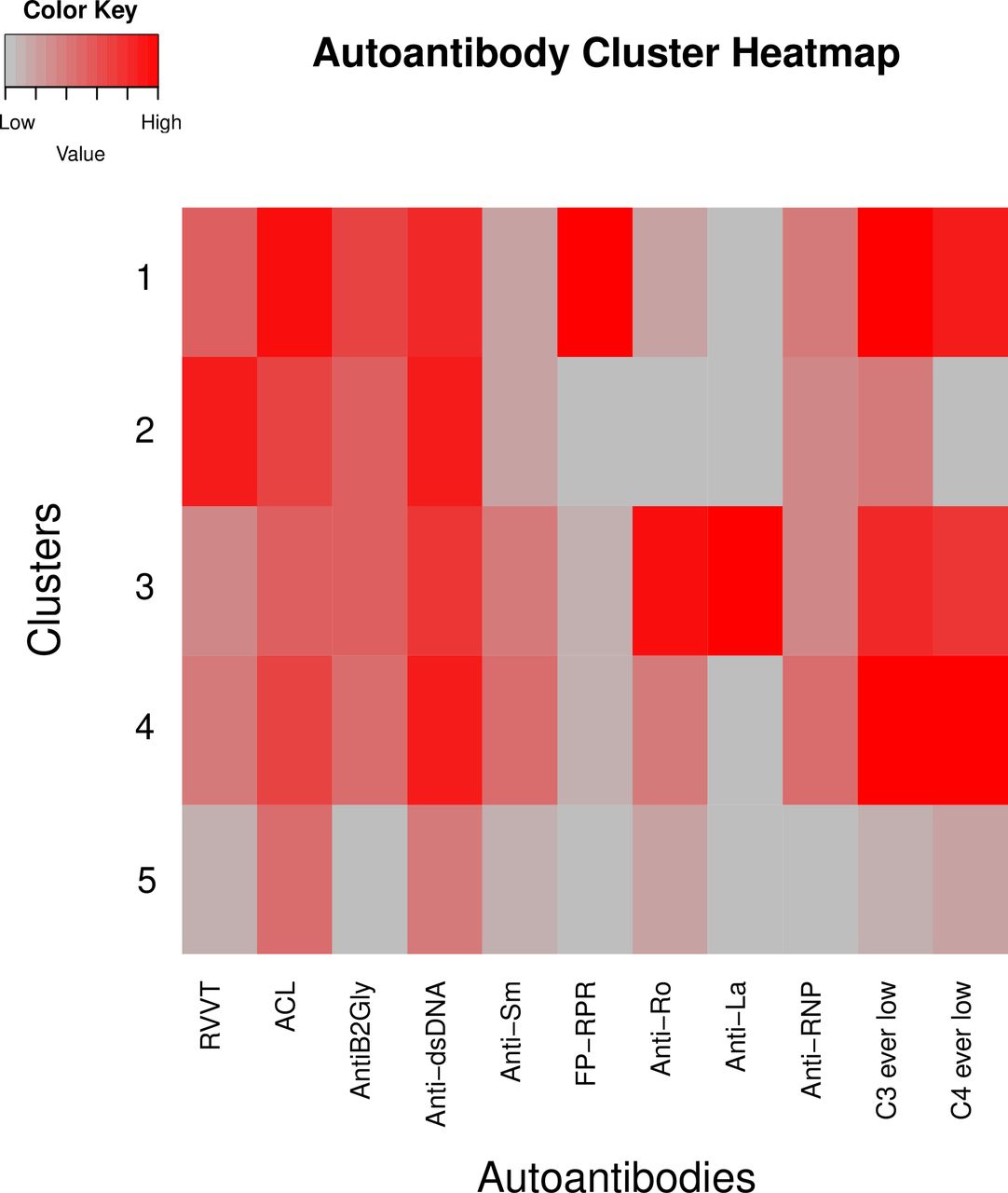
The heatmap shown in figure 1 depicts the five unique autoantibody clusters, with bright red representing high frequencies of a particular antibody and grey representing very low incidences of a particular autoantibody. Cluster 1, with 20 subjects, had high frequencies of anticardiolipin, anti-beta 2 glycoprotein, anti-dsDNA, false positive-RPR, low C4 and low C3, but a very low incidence of anti-La. Cluster 2, with 32 subjects, had high frequencies of lupus anticoagulant, anticardiolipin and anti-dsDNA, but low anti-Ro, anti-La, false positive-RPR and low C4. Cluster 3, with 15 subjects, had high frequencies of low C3, low C4, anti-Ro, anti-La and anti-dsDNA, and had some frequencies of all autoantibodies included in the analysis. Cluster 4, with 53 subjects, had high frequencies of low C3, low C4, anticardiolipin and anti-dsDNA, but low anti-La. Cluster 5, with 34 subjects, had no high frequencies of any autoantibody included in the analysis. Cluster 5 had only moderate frequencies of anti-dsDNA and anticardiolipin, and had low anti-beta 2 glycoprotein I, false positive-RPR and anti-La.
{kind=link}
SLE-associated pulmonary hypertension autoantibody clusters. Heatmap shows the frequency of each autoantibody by cluster. The scale on the left denotes antibody frequency from grey (0.0, low) to red (1.0, high). Heatmap rows corresponding to clusters 1, 2, 3, 4 and 5 are indicated. ACL, anticardiolipin; AntiB2Gly, anti-beta 2 glycoprotein I; anti‐dsDNA, antidouble-stranded DNA; anti‐RNP, antiribonucleoprotein; anti‐Sm, anti-Smith; FP‐RPR, false positive-rapid plasma reagin; RVVT, Russell’s viper venom time.
The clusters were immunologically distinct (p=0.0003; table 2). Cluster 1 had the highest frequency of false positive-RPR. Cluster 2 had the highest frequency of lupus anticoagulant. Cluster 3 was defined by anti-Ro and anti-La. Clusters 1, 3 and 4 had very high levels of hypocomplementaemia with over 96% of cluster 4 subjects having low C3 or low C4 (p<0.0001; table 2). Cluster 5 represented a nearly neutral phenotype, with less than 50% frequency of any autoantibody.
Patient demographics and ACR classification criteria by cluster
Demographic and clinical characteristics, ACR SLE classification criteria and comorbidities by cluster
The demographic characteristics and ACR SLE classification criteria of the 154 patients with SLE with pulmonary hypertension included in the clustering analysis are shown in table 2 by cluster. Age at pulmonary hypertension diagnosis significantly differed across clusters (p=0.0083), with cluster 4 representing the largest (n=53) and youngest (average age 40.2±16.3 years) cluster. Cluster 3 had the largest percentage of African–American patients and cluster 1 had the largest percentage of Caucasian patients. Cluster 3 was 100% female. A history of malar rash (p=0.0165), renal disorder (p=0.0214) and low complements, including low CH50 (p=0.0234), significantly differed across the clusters. Interestingly, ethnicity, serositis and haematological disorder were not significantly different across clusters.
There were no significant differences in the prevalence of cardiomyopathy, end-stage renal disease, cutaneous vasculitis, Raynaud’s phenomenon or pulmonary fibrosis across the five clusters (table 3). Clusters 1, 3 and 5 had no end-stage renal disease.
Comorbidities by cluster
Discussion
This is the first study using a clustering technique to evaluate the autoantibody profiles associated with SLE-associated pulmonary hypertension in a US, ethnically diverse cohort. We found that SLE-associated pulmonary hypertension disproportionately affects African–Americans and stratified into clinically relevant clusters, which differed by age and immunological activity, and were defined by specific autoantibody profiles. All autoantibodies selected for this study were readily available and could be measured routinely in most medical centres.
As demonstrated in other diverse pulmonary hypertension cohorts,17 18 African–Americans had a higher prevalence of pulmonary hypertension compared with Caucasian and Asian patients, with African–Americans making up more than half of the SLE cohort with pulmonary hypertension compared with 37.8% of those without pulmonary hypertension. Although there were no significant differences in ethnicity across clusters, there were trends of autoantibody profiles associating with African–American patients with SLE pulmonary hypertension. Cluster 3, the only cluster with anti-La positivity, was majority African–American, while cluster 1, the only cluster with false positive-RPR, was equally divided between African–American and Caucasian patients.
In the setting of SLE-associated pulmonary hypertension, our study identified five autoantibody profiles with three stable clusters representing unique phenotypes: antiphospholipid antibody predominant (cluster 1), anti-Ro and anti-La predominant (cluster 3), and neutral (cluster 5). Clusters 1 and 2 exhibited an antiphospholipid antibody predominant profile with the highest levels of anticardiolipin and lupus anticoagulant, respectively. Anticardiolipin was previously identified as a risk factor in a Chinese cohort,19 while lupus anticoagulant was found in a UK cohort.14
Cluster 3 was defined by anti-Ro and anti-La, possibly representing an SLE phenotype with features of Sjogren’s, which can be associated with pulmonary hypertension.36–38 This is consistent with work by Hachulla et al5 showing significantly higher incidences of anti-Ro and anti-La in patients with SLE with pulmonary hypertension compared with those without, suggesting these autoantibodies may be risk factors for pulmonary hypertension in SLE. In our previous work on clusters of SLE, we found a cluster described by anti-Ro and La as well.39
Anti-dsDNA was elevated across all clusters, in contrast to hypocomplementaemia, which was found only in clusters 1, 3 and 4. These differences in complement levels may reflect more serologically active (clusters 1–4) versus serologically inactive (cluster 5) states. Whether these clusters might reflect different pathophysiology and potentially different susceptibilities to immunosuppressive versus vasodilatory therapies must be studied prospectively.
There are limitations to our study. First, the definition of pulmonary hypertension is based on elevated right ventricular systolic pressure or dilated pulmonary artery on chest CT and is not sufficient for subclassifying pulmonary hypertension into a WHO class. Second, as the Hopkins Lupus Cohort started 30 years ago, specific treatments for pulmonary hypertension were not available for most of the duration of the cohort. Finally, although three of the five clusters were stable with mean Jaccard coefficients above 0.6, clusters 2 and 4 were not as stable based on low mean Jaccard coefficients. Despite these limitations, our study confirms that pulmonary hypertension is an important complication of SLE in African–American patients and demonstrates that SLE-associated pulmonary hypertension is associated with specific autoantibody profiles.
References
Footnotes
Funding This work was supported by grant number T32-AR048522 and grant number R01- AR69572 from the National Institutes of Health (NIH) and the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS). This publication was also supported by the Cupid Foundation Discovery Fund from the Johns Hopkins Division of Rheumatology.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Hopkins Lupus Cohort was approved yearly by the Johns Hopkins University School of Medicine Institutional Review Board (NA_00039294) and complied with the Health Insurance Portability and Accountability Act and the Helsinki Declaration. All patients gave written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.