Article Text

Abstract
Objective A link between bone metabolism and cardiovascular (CV) disease has been suggested mainly in the general population. In the current study we explored whether altered bone metabolism influence CV risk in patients with SLE.
Methods In 138 consecutive patients with SLE, atherosclerosis was assessed by the presence of plaque and/or arterial wall thickening in carotid/femoral arteries by ultrasound. Bone mineral density (BMD) levels and hip/spinal cord fractures together with classical CV disease and osteoporosis risk factors including serum 25(OH) vitamin D3 and parathormone (PTH) levels were recorded in all patients. Serum osteoprotegerin (OPG) and receptor activator of nuclear factor kappa-Β ligand were quantitated by commercial ELISA. Statistical analysis included both univariate and multivariate models.
Results Abnormal PTH serum concentrations (>65 pg/mL)—but not 25(OH) vitamin D3 serum levels—were identified as a risk factor for both plaque formation and arterial wall thickening in patients with SLE (ORs (95% CIs): 8.2 (1.8 to 37.4) and 3.9 (1.3 to 11.8), respectively). This association remained significant following adjustment for vitamin D3 levels and classical CV risk factors. Moreover, an independent association between osteoporosis with plaque formation and arterial wall thickening was detected following adjustment for total steroid dose, premature menopause and disease duration (ORs (95% CIs): 5.3 (1.1 to 26.2) and 3.5 (1.1 to 11.4), respectively). An inverse correlation between femoral neck BMD values and intima–medial thickness scores was also observed (r: −0.42, p=0.008).
Conclusions These findings further strengthen the concept of shared pathophysiological mechanisms between atherogenesis and altered bone metabolism in autoimmune populations, revealing heightened PTH levels as a potential marker for atherosclerosis among patients with SLE.
- systemic lupus erythematosus
- atherosclerosis
- osteoporosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In the general population, osteoporosis and cardiovascular disease (CVD) have been perceived not only as coexisting conditions of the elderly but also as inter-related disorders affecting both sexes1 2; therefore, the idea of a common, yet unknown link in the pathogenesis of both entities seems appealing.3 Alterations in the osteoprotegerin (OPG)/receptor activator of nuclear factor kappa-Β ligand (RANKL) axis have been previously postulated as common denominators. Indeed, the contribution of bone metabolism markers such as OPG or osteopontin has been previously shown to serve as surrogate markers for CVD.4 Moreover, OPG-deficient mice displayed increased atherosclerosis, vascular calcification and osteoporosis together with heightened circulating RANKL levels.5
A candidate molecule which attracted particular attention in recent years is 25(OH) vitamin D3 (25-OHD), due to pleiotropic functions extending beyond bone mineralisation and calcium homeostasis. Therefore, the presence of 25-OHD receptors in cardiovascular (CV) tissue cells6 7 and the associations of low 25-OHD concentrations with myocardial infarction, extent of coronary artery disease and worse CV-related clinical outcome8 9 support this concept. A number of studies, though not all, have also reported associations of low 25-OHD levels with subclinical atherosclerosis.10–13 In addition, parathormone (PTH)—traditionally considered an endogenous biological marker of 25-OHD deficiency—has also been linked to coronary heart disease14 and CV mortality.15
A growing body of evidence over the last years revealed an excessive burden of both CVD and impaired bone health in patients with systemic autoimmune disorders.16–18 For instance, in SLE, heightened rates of both subclinical atherosclerosis,16 osteoporosis as well as peripheral and vertebral fractures have been repeatedly reported.19 20 Moreover, low 25-OHD levels (<20 ng/mL) were found to be prevalent in patients with SLE .21 This is a rather unsurprising finding given that patients with SLE are advised to avoid sun exposure, often suffer from renal dysfunction and are subjected to medication affecting 25-OHD metabolism, such as antimalarials and corticosteroids; in addition, disease activity has been found to decrease 25-OHD concentrations.21
In the present study, we sought to investigate whether 25-OHD deficiency and/or increased PTH levels, as well as bone density alterations, influence atherosclerosis in patients with SLE.
Methods
Study subjects
In the present study, 138 consecutive patients with SLE (mean age ±SD: 44.7±13.6, female prevalence: 94%) according to the American College of Rheumatology 2012 criteria for the classification of SLE22 were included. All patients were followed by HMM, CPM and MG. Criteria exclusion included age <18 years old, pregnancy and renal dysfunction (serum creatinine levels >3 mg/dL, creatinine clearance <30 mL/min). All participants provided informed consent prior to study entry. Patients with prior CV events were not excluded.
Assessment of atherosclerosis and impaired bone health
All study participants were evaluated by ultrasound for carotid and/or femoral plaque detection. Additionally, measurement of intima–medial thickness (IMT) scores at the same sites was performed in 125 SLE and mean scores were calculated as previously described. IMT score higher than 0.90 mm was defined as arterial wall thickening.23 In detail, both the carotid (common carotid, bifurcation and internal carotid) and the femoral (common femoral and superficial femoral) arteries were evaluated in each individual by ultrasound (iU22; Philips, Royal Philips Electronics of the Netherlands). The mean carotid artery IMT was defined as the average of 36 IMT readings (common, bifurcation, and internal carotid arteries, right and left side, far and near wall, with three sampling points per segment) and the mean femoral artery IMT was the average of 24 IMT readings (common and superficial femoral arteries, right and left sides, far and near wall, with three sampling points per segment), as previously described.23 Plaque formation was defined as a focal protrusion of more than 50% of the surrounding wall.24 The radiologist (EA) in charge of the ultrasound scanning was unaware of the clinical diagnosis of the subjects under evaluation.
Bone mineral density (BMD) measurements were performed in all study participants using dual X-ray absorptiometry QDR4500 (Hologic). BMD measurements were performed either on the spine or hip, according to age.25 Thus, in patients <65 years old, BMD was measured on the spine, while in those >65 years old, BMD was measured on the hip. For postmenopausal women and men ≥50 years old, the presence of osteoporosis or osteopaenia was defined according to the WHO classification system, as a T-score less than −2.5 SDs and −1 SDs, respectively, at either site of measurement. For premenopausal patients or men aged <50 years, the Z-score for low BMD was implemented, with z-score less than −2SD considered low BMD for chronological age. 26 Lateral radiographs of the thoracic and lumbar spine were implemented to identify asymptomatic vertebral fractures by semiquantitative evaluation.27 Vitamin D deficiency was defined as serum 25-OHD levels lower than 20 ng/mL, while cut-off value for high PTH levels was set as 65 pg/mL, as previously suggested.28
Disease and traditional risk factors for atherosclerosis and impaired bone health
Demographic data (age, sex and body mass index (BMI)), clinical and laboratory features, disease activity/damage scores (SLEDAI: Systemic Lupus Erythematosus Disease Activity Index, SLICC: Systemic Lupus International Collaborating Clinics), current and prior medications, traditional risk factors for atherosclerosis and osteoporosis and bone metabolism parameters were thoroughly recorded as previously described.29 30 Additionally, all patients underwent evaluation for traditional CVD risk factors such as serum cholesterol, triglyceride and homocysteine levels as well as bone metabolism markers including PTH and 25-OHD serum levels. Blood was drawn in the morning in fasting conditions.
OPG and RANKL quantitation
To explore whether the RANK/RANKL/OPG signalling pathway is implicated in the pathogenesis of SLE-related atherosclerosis, OPG/RANKL levels were determined in available sera from 28 patients with SLE by commercial ELISA, as per manufacturer instructions.
Statistical analysis
Two-sided Fisher’s exact and Mann-Whitney or Kruskal-Wallis tests were used to compare qualitative and quantitative characteristics, respectively, and ORs with 95% CIs were calculated. To test whether osteoporosis (independent variable) was associated with plaque formation (dependent variable) in SLE, a multivariate backwards stepwise model including SLE-related shared risk factors for both entities such as disease duration, total steroid dose, premature menopause was constructed. Similarly, to assess whether PTH levels (independent variable) are associated with plaque formation or arterial wall thickening (dependent variables) independently of 25-OHD serum levels and other potential confounders for CV risk, a second multivariate model was implemented. Pearson’s correlation coefficient analyses were used for the detection of a relationship between IMT and BMD values in patients with SLE. A p-value of less than 0.05 for univariate analyses and 0.1 for multivariate analyses, respectively, were considered statistically significant. Data were analysed by the SPSS V.25.0 statistical package.
Results
Contributors of atherosclerosis in SLE
Traditional and disease-related risk factors
As shown in table 1, and in line with previous reports, traditional CV risk factors and disease-related features have been both found to account for plaque formation and/or arterial wall thickening among patients with SLE.31 Age, BMI, hypertension, triglycerides, menopausal status and disease duration were found to be associated with both plaque formation and high IMT scores, while total steroid dose with plaque. A protective role for higher current steroid dose for arterial wall thickening was also observed. In the entire cohort, two patients had a history of stroke and one patient a history of stroke and coronary artery disease (data not shown).
Contribution of traditional and disease-related risk factors in carotid/femoral plaque formation and arterial wall thickening (IMT >0.90 mm) among patients with SLE
Bone metabolism regulators/markers
We next wished to explore whether bone metabolism-related features can contribute to atherosclerosis among patients with SLE.
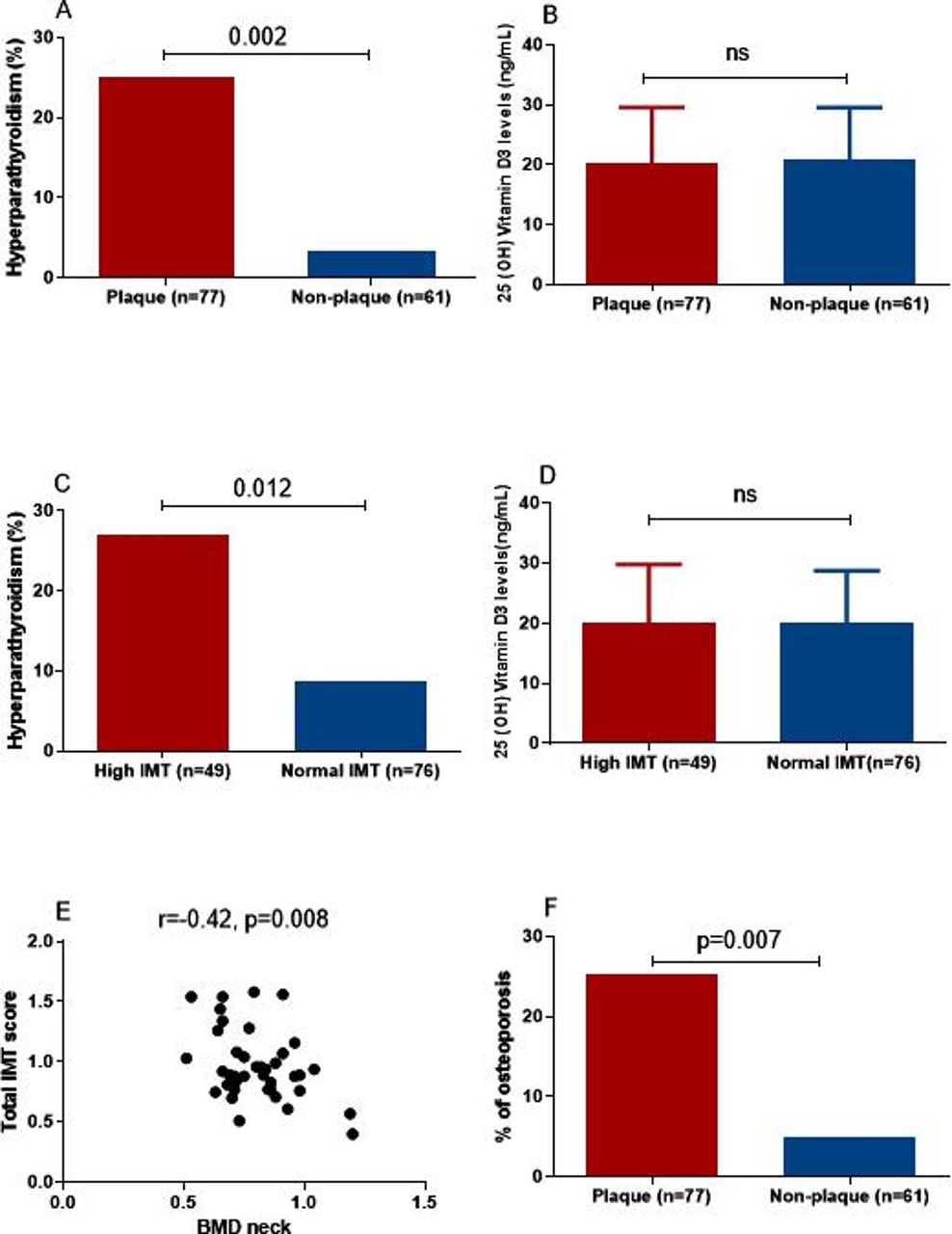
As shown in table 2, PTH levels were found to be significantly increased in patients with SLE with plaque formation and/or arterial wall thickening compared with those without (51.1±27.7 vs 37.4±18.4 pg/mL, p=0.003 and 54.0±32.7 vs 40.0±18.3 pg/mL, p=0.02, respectively). Moreover, as shown in both figure 1A,C and table 2, the presence of hyperparathyroidism (defined as PTH serum levels >65 pg/mL) was also found to be significantly associated with plaque formation and arterial wall thickening (25% vs 3.9%, p=0.002 and 27% vs 8.7%, p=0.012, respectively) and was therefore identified as a risk factor for both plaque formation and arterial wall thickening (ORs (95% CIs): 8.2 (1.8 to 37.4) and 3.9 (1.3 to 11.8), respectively). No association was observed between plaque or arterial wall thickening with 25-OHD levels or 25-OHD deficiency (figure 1B,D; table 2) serum or urine calcium and phosphate levels and collagen cross-links CTX (C-terminal telopeptide of type I collagen) and NTX (N-terminal telopeptide of type I collagen) (table 2). No patient was on PTH or denosumab. Following adjustment for 25-OHD levels, diabetes, hypertension, high cholesterol (>200 mg/dL) and triglyceride (>150 mg/dL) levels, increased BMI (more than 25 kg/m2), advanced age (>70 years old) and menopausal status, the association between PTH levels with plaque and arterial wall thickening remained significant (ORs (95% CIs): 1.024 (1.001 to 1.048) and 1.031 (1.007 to 1.055), respectively (table 3).
Contribution of bone metabolism features in carotid/femoral plaque formation and arterial wall thickening (IMT>0.90 mm) among patients with SLE
{kind=link}
(A) Increased rates of elevated serum parathormone (PTH) levels (>65 pg/mL, hyperparathyroidism) in patients with SLE with plaque compared with those without (25% vs 3.9%, p=0.002). (B) No statistically significant differences in 25(OH) vitamin D3 (25-OHD) levels in patients with SLE with or without plaque formation (20.2±9.4 vs 20.2±8.4 ng/mL, non-significant (ns)). (C) Increased rates of elevated serum PTH levels (>65 pg/mL, hyperparathyroidism) in patients with SLE with arterial wall thickening (intima–media thickness (IMT) scores >0.90 mm) in comparison to those with normal IMT scores (27% vs 8.7%, p=0.012). (D) Lack of association of 25-OHD levels with arterial wall thickening in patients with SLE (20.0±9.7 vs 19.9±8.7 ng/mL, ns). (E) Inverse correlation of femoral neck bone mineral density (BMD) with intima-medial thickness (IMT) score in patients with SLE by Pearson’s correlation test. (F) Higher prevalence of osteoporosis in patients with SLE with plaque formation compared with those without (25.4% vs 4.9%, p=0.007).
Independent associations between PTH levels with plaque formation and arterial wall thickening, after adjustment for 25-OHD serum levels, diabetes, hypertension, high cholesterol and triglyceride levels, increased BMI, advanced age and menopausal status
In view of the association between serum PTH levels and atherosclerosis, we next wished to explore whether patients with SLE with plaque formation and/or arterial wall thickening also display reduced BMD levels. As depicted in figure 1E, an inverse correlation between femoral neck BMD values and total IMT scores was detected (r: −0.42, p=0.008). No significant correlation was detected between spine BMD levels and IMT scores (r=0.20, p=0.11, data no shown). Furthermore, patients with SLE with plaque formation exhibited increased rates of osteoporosis compared with those without (25.4% vs 4.9%, p=0.007, OR 95% (CI): 6.7 (1.4 to 30.9) (table 2; figure 1F)). Similarly, a higher frequency of osteoporosis was detected among patients with high IMT scores compared with those without (26.3 vs 8.8, p=0.04, OR 95% (CI): 3.7 (1.2 to 11.9); table 2). Following adjustment for disease duration, total steroid dose and premature menopause, osteoporosis turned to be independent risk factor for both plaque formation and arterial wall thickening in patients with SLE (ORs 95% CI: 5.3 (1.1 to 26.2) and 3.5 (1.1 to 11.4), respectively, (table 4)).
Independent associations between osteoporosis with plaque formation and arterial wall thickening, after a multivariate model was applied considering potential confounders (disease duration, premature menopause and total steroid dose)
Clinical and serological associations of high PTH levels in patients with SLE
To explore the underlying aetiology of elevated PTH serum concentrations (defined as >65 pg/mL) and identify potential links to atherosclerosis in patients with SLE, we compared patients with high versus low PTH levels in terms of demographic characteristics, metabolic and disease-related features, as well as bone metabolism-related parameters. As shown in table 5, significantly lower 25-OHD concentrations were observed in the high PTH group (14.3±5.9 vs 21.1±8.7 ng/mL, p=0.003), with higher rates of 25-OHD deficiency (70.6% vs 47.4%). None of the patients had evidence of hypercalcaemia suggesting primary hyperparathyroidism (data not shown). Other significant associations of elevated serum PTH included age and higher LDL levels. No statistically significant differences in statin use were detected between the high versus the low PTH group (22.2% vs 14%, p-value: 0.48). Osteoporosis, osteopaenia and osteoporotic fractures displayed higher frequency in the high serum PTH group, though the differences did not reach statistical significance, possibly due to the limited patient number (table 5).
Comparison of clinical and serological parameters among patients with SLE with high (defined as >65 pg/mL) and normal PTH levels (≤65 pg/mL)
PTH and OPG/RANKL/RANK signalling pathway
In view of previously published data showing that PTH influences both OPG and RANKL gene expression,32 together with the increasingly recognised involvement of the OPG/RANKL/RANK signalling pathway in vascular calcification,25 we aimed to explore whether OPG/RANKL/RANK pathway is activated in patients with SLE with high PTH levels. RANKL and OPG levels were measured in available sera from 28 female patients with SLE and RANKL/OPG ratio was also determined. Among them, 7 patients exhibited high serum PTH levels, while 21 had PTH concentrations within normal range. The two groups did not differ in terms of age (49.9±4.2 vs 48.3±5.8 years, p=ns), or prevalence of osteoporosis or osteopaenia (57.1% vs 52.6%). No statistically significant associations emerged between high/low PTH status and OPG and RANKL levels or RANKL/OPG ratio (164.94±77.33 vs 156.60±51.51 pg/mL, 2496.75±1597.87 vs 2390.43±1299.32 pg/mL and 14.94±5.54 vs 16.82±11.05, respectively, all comparisons non-significant; online supplementary figure 1). Additionally, no statistically significant associations were detected between OPG/RANKL levels and plaque or arterial wall thickening (data not shown).
Supplemental material
Discussion
In the present study, while we confirm previous reports of an excessive atherosclerotic burden in patients with SLE, we report a novel association between increased PTH—but not 25-OHD—serum levels with both arterial wall thickening (IMT >0.9 mm) and plaque formation. Furthermore, an inverse association between femoral neck BMD values and total IMT scores was observed, together with increased rates of osteoporosis among patients with SLE with plaque formation.
Increased PTH levels have been previously linked to CVD in general population. The underlying mechanisms behind this association might be related to hypertension, metabolic syndrome, glucose intolerance and insulin resistance, previously reported in patients with hyperparathyroidism, potentially as a result of activated renin–angiotensin–aldosterone system.33–35 In addition, PTH has been found to influence the expression of proinflammatory endothelial factors, such as the receptor of advanced glycation end products and interleukin 636 and to promote osteoblastic differentiation of endothelial cells through induction of bone morphogenetic proteins.37 Towards the same direction, arterial wall thickening,33 endothelial dysfunction,38 number of stenotic coronary arteries14 and increase in CVD mortality15 have been reported in association with high PTH levels. In the current study, none of the patients with heightened PTH levels had evidence of primary hyperparathyroidism; advanced age and reduced 25-OHD serum levels seemed to account for these cases. With the exception of a sole paediatric SLE study where no associations between serum PTH levels and IMT scores or alterations in high-density lipoprotein/low-density lipoprotein cholesterol profile were detected,39 no other data have been so far available in SLE populations.
There is ample evidence of 25-OHD involvement in CVD development,6–8 40 and 25-OHD deficiency has been shown to influence endothelial dysfunction in both animal models41 and patients with SLE,42 possibly as a result of increase in interferon activity,41 43 previously shown to be involved in SLE-related atherosclerosis.44 In the present report, no association between atherosclerosis and 25-OHD serum levels was observed. This finding is in accord with a prospective study by Kiani et al45 in 154 patients with SLE, assessing the progression of carotid/coronary atherosclerosis over a 2-year period. Similarly, in patients with SLE of Asian descent, no associations were detected between 25-OHD levels and carotid/coronary plaque or carotid IMT scores.46 Only in a SLE cohort of predominantly African-American origin, low 25-OHD levels were found to be associated with carotid plaque formation, after adjustment for age.47
These apparently discrepant findings could be attributed to methodological limitations in 25-OHD measurement by immunoassay due to hydrophobic properties of the molecule.48 Therefore, concomitant evaluation of PTH concentrations could provide more accurate information on 25-OHD status of populations under examination.
In the present study, 25-OHD deficiency was detected in 49.6% of patients with SLE, in accord with previously reported rates.21 It should, however, be mentioned that approximately three quarters of our patients were already receiving vitamin D supplementation in doses varying from 400 IU to 800 IU daily together with calcium, as a preventive measure against corticosteroid-induced osteoporosis. Although it has been suggested that vitamin D supplementation could have beneficial effects on endothelial function in patients with SLE,49 in another SLE cohort higher 25-OHD levels and vitamin D/calcium supplement intake were identified as risk factors for arterial stiffness.50 In view of a recent report where vitamin D supplementation did not lower the incidence of CV events in general population,51 its use for disorders other than bone metabolism alterations cannot be advocated; in fact, increased doses should be avoided as they could even be immunologically damaging.52 53
Another key observation in the present study is the negative association between BMD levels and markers of atherosclerosis, consistent with previous findings in both SLE and Sjogren’s syndrome.25 30 54 However, other studies on SLE did not confirm an association between the two entities.55 56 Deposition of hydroxyapatite crystals in atherosclerotic lesions along with osteoblast or osteoclast resembling cells in the arterial wall,3 as well as alterations in the OPG/RANKL axis and Wnt signalling3 30 could provide some pathophysiological clues linking CVD and osteoporosis. In the present study, examination of a small subset of our SLE cohort did not detect statistically significant associations between OPG and RANKL levels and high PTH or markers of atherosclerosis. However, larger studies along with exploration of other signalling pathways would be needed to confirm these results.
The major strength of the present study is the thorough characterisation of potential contributors to both osteoporosis and atherosclerosis in an SLE cohort, which was the primary goal of the present work. We, however, acknowledge the limited power of the present report to reliably identify comparative differences between patients with SLE and controls due to the small number of individuals included as well as the limited sample size for several comparisons does not allow for accurate inferential conclusions. Moreover, no data on vascular calcification were available which could explore the idea of calcium mobilisation from bones to vessels, as previously suggested through Wnt signalling mechanisms.30 Furthermore, the rates of fractures in the present study seem to be lower compared with previous reports, potentially reflecting genetic differences, different rates of adherence to vitamin D, calcium supplements and bisphosphonates or heterogeneous SLE populations requiring different steroid doses.19 Finally, a small subset of patients included in the study had stroke and coronary disease and therefore they had possibly experienced procedures such as coronary artery bypass graft surgery or carotid endarterectomy which could affect the evaluation of carotid plaque.
Conclusions
In conclusion, in the present study, in line with previous observations in healthy and autoimmune populations, an interplay between impaired bone health and atherosclerotic disease is revealed in patients with SLE as well. Moreover, we suggest high PTH serum levels as a potential biomarker of atherosclerosis in these patients, further strengthening the idea for adequate vitamin D supplementation in these individuals.
References
Footnotes
Presented at Data from this manuscript have been previously presented in an abstract form https://ard.bmj.com/content/78/Suppl_2/1720.2
Contributors Conception and design: CPM, HMM. Experimental procedure: CS. Administrative support: AS. Provision of patients and controls: HMM, CPM, MG, AS. Collection and assembly of data: MG, CPM, AS. Data analysis and interpretation: CS, MG, CPM. Manuscript drafting: MG, CPM. Final approval of manuscript: all authors.
Funding This study was supported by Hellenic Rheumatology Society and Grant code 70/3/11260.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the Ethics Committee of the General Hospital of Athens “G.Gennimatas”.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.