Article Text

Abstract
There is currently no uniform definition of cutaneous lupus erythematosus (CLE) upon which to base a study population for observational and interventional trials. A preliminary questionnaire was derived from and sent to a panel of CLE experts which demonstrated consensus agreement that (1) there is a need for new definitions for CLE (2) CLE is distinct from systemic lupus erythematosus and that a CLE grouping scheme should remain apart from current systemic lupus erythematosus schema (3) current CLE grouping schemes are inadequate around communication, prognostic information and to meet the needs of researchers, clinicians, patients and payers.
- Health services research
- Qualitative research
- Systemic Lupus Erythematosus
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background/Introduction
Cutaneous lupus erythematosus (CLE) remains an ill-defined set of disorders, often grouped together based on common clinical features, histopathological findings, laboratory abnormalities, association with underlying systemic lupus erythematosus (SLE) or combinations thereof. In 1981, Dr James Gilliam and Dr Richard Sontheimer proposed a grouping ‘classification’ schema to deal with the heterogeneity inherent to this set of disorders.1 Since that time, a variety of other grouping schemes have been proposed with variable uptake by the medical and scientific communities invested in CLE. There is currently no uniform definition of CLE upon which to base a study population for observational and interventional trials. This has led to inconsistency among studies in the field. In addition, the current grouping systems are heterogeneous, inconsistent, and none have been formally adopted by the ‘expert’ community of investigators and clinicians committed to these disorders.
At the 3rd International Meeting on Cutaneous Lupus Erythematosus (ICCLE) held May 2013 in Edinburgh, Scotland, a scientific meeting was called at which nominal groups of international CLE experts were formed around stating the need for change and to generate item lists that characterise CLE. Facilitated, open-ended concept-mapping and brain-storming sessions were used to generate these item lists. The expressed goal was to agree upon an approach to consensus around (1) uniform definition(s); (2) grouping schemes; and (3) clarifying an understanding of the complex relationship between cutaneous and systemic disease involvement. Based on the input from the ICCLE meeting key stakeholder groups were defined, lists of CLE-defining characteristics were generated and the use of a Delphi consensus method was agreed upon.
The Delphi technique is a method of consensus-building using a series of iterative questionnaires to collect data from a panel of selected experts/stakeholders in a given area of interest. The iterative nature of the process, together with controlled anonymous feedback at each questionnaire stage, subject anonymity and a predefined stop criterion, allow convergence towards a consensus ‘answer’.2 ,3 There are many examples of relevant Delphi exercises in this area of the field, including a Delphi consensus process around the development of classification criteria for systemic sclerosis using experts in this disease state.4
In follow-up to the ICCLE meeting, a ‘pre-Delphi’ questionnaire was put forth to a relevant stakeholder group including paediatric and adult dermatologists, rheumatologists and dermatopathologists. The goal of this questionnaire was to further build a database of international participant stakeholders and more broadly query the relevant participant pool regarding the need for uniform definitions, revision of grouping schema and defining the CLE/SLE relationship as an expert community.
Methods
Figure 1 describes a process overview beginning with the ICCLE meeting. Invitations to complete the 12-question survey were sent to 81 expert participants. The 12 questions presented were those outlined and agreed upon by the concept-mapping process by the participants at the ICCLE meeting. Survey results were collected anonymously over a 3 month period. Descriptive statistics were used to evaluate responses: the median score is reported as the preferred measure in a Delphi process (a measure of central tendency that is minimally distorted by outliers). Survey responses were graded on a continuous scale from 0 to 100 (0=complete disagreement with the proposed statement, 50=neutral response, 100=complete agreement with the proposed statement). A median response of 70 or greater was predefined as ‘consensus agreement’, a median response of 30 or lower was predefined as ‘consensus disagreement’, median scores between 30 and 70 were predefined as ‘no consensus’ among participants.
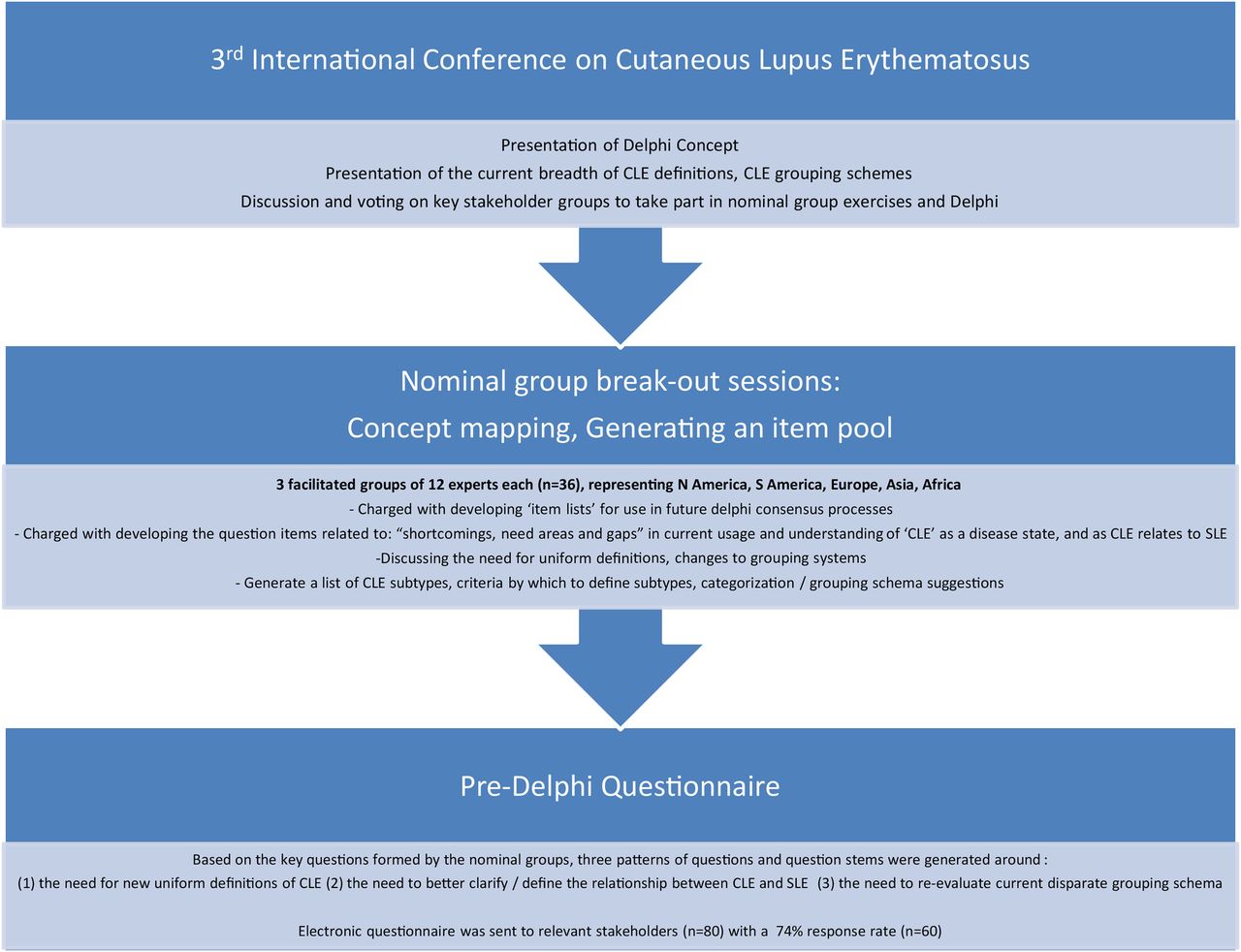
Summary flow diagram leading to pre-Delphi exercise.
The survey questionnaire was designed and implemented using RedCAP software.5
Results
The survey response rate was (n=60/81) 74% with a group comprised predominantly of dermatologists (n=58, 96.7%); rheumatologists (n=5, 8.3%), dermatopathologists (2, 3.3%). Paediatric subspecialists were lacking in the initial survey. Survey participants self-reported their geographic location to be: North America (n=39, 65%), Europe (n=15, 25%), Asia (4, 6.7%), South America (n=1, 1.7%), Africa (n=1, 1.7%). The Middle East and Australia were not represented in the initial survey.
Table 1 demonstrates the median and per cent of respondents by agreement for each of the 12 questions posed. Based on prespecified consensus criteria as noted above, there is consensus agreement on two-thirds of the survey items: questions 1, 3–6, 8, 9 and 12. Complete agreement is highest for question 1 (46.7%), question 6 (45.8%) and question 4 (45.0%). Consensus disagreement was found to questions 2 and 7, though variability is high for both (IQR of 67.0 and 49, respectively). Of the respondents 22.4% completely disagree with question 2. No consensus was found to questions 10 and 11. Details of the data distribution of each question are found in the histogram distribution of scores (figure 2).
Median and per cent of respondents by agreement

{kind=link}
{kind=link}
Histograms of question scores.
Discussion and future directions
Interpretation of the survey results presented above may be best described in three thematic groups: (1) the need for new definitions of CLE (questions 8, 9, 12) (2) the need to better clarify/define the relationship between CLE and SLE (1, 2, 3) (3) the need to re-evaluate current disparate grouping schema (4–7, 10, 11). There was consensus among this group of questions, indicating that the expert panel of participants agreed that there is a need for new definitions for CLE as current definitions impede communication between physician colleagues and in physician-patient interactions. With regards to the CLE-SLE relationship, there was consensus agreement that CLE is distinct from SLE and that a CLE grouping scheme should remain apart from current SLE schema which otherwise include mucocutaneous disease items. Finally, with regards to the current grouping schema, there was consensus that the current schemes are inadequate around communication, prognostic information and to meet the needs of researchers, clinicians, patients and payers. However among this question pool, there was no consensus agreement that the current grouping schemes affected treatment decisions or failed to inform about risks during pregnancy. The pre-Delphi exercise was largely about establishing (1) where confusion and gaps exist around CLE terminology (2) prioritising the group's efforts with regards to where we will focus our resources moving forward with the Delphi process. We hope that this article will encourage other relevant stakeholders in the CLE Delphi process to come forward and take part in helping to improve the inconsistencies in the field. Each of the general themes build upon one another and because the pre-Delphi exercise has demonstrated consensus that even definitions are lacking, we will begin with a stepwise approach (A) definitions (B) grouping schemes/‘classification criteria’ (C) ‘diagnostic criteria’. Building on these results, the steering committee has moved to proceed with a formal Delphi consensus process with an initial focus on ‘defining CLE’, which should be a good platform for the subsequent processes to achieve an international classification scheme. In the vasculitis literature, analogous processes have been used successfully to first define, then build classification and diagnostic criteria.6 These same processes may later expand to include diagnostic, classification criteria as well as outcomes measures (distinct from SLE diagnostic and classification systems), such as those modelled by the OMERACT group for developing outcome measures in rheumatoid arthritis.7
Footnotes
-
Contributors JFM and VPW had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. JFM, VPW and JD: study concept and design. JFM and VPW: acquisition of data. JFM and VPW: analysis and interpretation of data. JFM, FN, FF, MJG, MH, BM, JS, JD and VPW: drafting of the manuscript. JFM, FN, FF, MJG, MH, BM, JS, JD and VPW: critical revision of the manuscript for important intellectual content. JFM: statistical analysis. VPW: obtained funding. VPW and JD: study supervision. Cara Joyce: administrative, technical or material support.
-
Funding Cara Joyce, Tulane University (New Orleans LA), provided biostatistical support. This work was supported by the Department of Veterans Affairs (Veterans Health Administration, Office of Research and Development, Biomedical Laboratory Research and Development to VPW) as well as Departmental Funds from the BWH Department of Dermatology. JFM is a consultant for Biogen IDEC, Amgen, Abbvie, Eli Lilly, and licensed a questionnaire to Abbvie. He has received grant from Biogen IDEC. JS is a consultant for AbbVie, Biogenetica International Laboratories, Leo Pharma, Merck-Serono, Novartis, Pierre-Fabre, Sandoz, Toray Corporation and is a speaker for AbbVie, Astellas, Actavis, Adamed, Berlin-Chemie Mennarini, Bioderma, Fresenius, Janssen-Cilag, Leo Pharma, Takeda and Vichy. JD is a consultant and speaker for Janssen-Ortho, Abbvie, Amgen, Leo Pharma, Celgene, Roche and Novartis and has received grants from Abbie and Celgene. MJG is a consultant for Abbvie, Janssen, Novartis and Celgene, and is a speaker for Abbvie, Janssen and Leo. He has received funding from Janssen, Pfizer, Novartis, Leo and Abbvie.
-
Competing interests None.
-
Ethics approval Partners IRB/Brigham and Women's Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.