Article Text

Abstract
Objectives The interest on autoimmune diseases (ADs) and their outcome at the intensive care unit (ICU) has increased due to the clinical challenge for diagnosis and management as well as for prognosis. The current work presents a-year experience on these topics in a tertiary hospital.
Methods The mixed-cluster methodology based on multivariate descriptive methods such as principal component analysis and multiple correspondence analyses was performed to summarize sets of related variables with strong associations and common clinical context.
Results Fifty adult patients with ADs with a mean age of 46.7±17.55 years were assessed. The two most common diagnoses were systemic lupus erythematosus and systemic sclerosis, registered in 45% and 20% of patients, respectively. The main causes of admission to ICU were infection and AD flare up, observed in 36% and 24%, respectively. Mortality during ICU stay was 24%. The length of hospital stay before ICU admission, shock, vasopressors, mechanical ventilation, abdominal sepsis, Glasgow score and plasmapheresis were all factors associated with mortality. Two new clinical clusters variables (NCVs) were defined: Time ICU and ICU Support Profile, which were associated with survivor and no survivor variables.
Conclusions Identification of single factors and groups of factors from NCVs will allow implementation of early and aggressive therapies in patients with ADs at the ICU in order to avoid fatal outcomes
- Autoimmune Diseases
- Systemic Lupus Erythematosus
- Systemic Sclerosis
- Arthritis
- Outcomes research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Morbidity and mortality in patients with autoimmune diseases seen at the intensive care unit (ICU) is still high.
Infections and flare-up are major causes of ICU admission.
Delay in ICU admission increases risk of mortality.
Mixed-cluster analysis is a novel methodology establishing subgroups in real life.
Introduction
Autoimmune diseases (ADs) are chronic and heterogeneous conditions that affect specific target organs or multiple organ systems. These conditions share several clinical signs and symptoms, physiopathological mechanisms and genetic factors (ie, the autoimmune tautology).1 Their incidence ranges from 1 to 20 cases per 100 000 person-years and the estimated prevalence is about 3%.2 The impact of ADs resides in the high risk of morbidity and mortality they hold.3 The chronic nature of these diseases places a significant burden on the use of healthcare resources, which translate into elevated economic costs and low quality of life compared with the general population.
Patients with ADs may be admitted to the intensive care unit (ICU), making them a challenge to the intensivist.3–5 The prevalence of ADs in the ICU has changed in the past decades. In the past, the main ADs admitted to ICU, in order of frequency, were rheumatoid arthritis (RA), systemic lupus erythematous (SLE) and systemic vasculitis (SV). However, in the past decades SLE has been the most common AD reported.5 Mortality of patients at the ICU has been shown to be variable, ranging from 17% to 55%.5
Although patients with ADs may have diverse causes of admission to the ICU, acute flare of the disease and infection, mainly due to immunosuppression, is the most important.3–6 Since the expression of diseases varies depending on geography and ethnicity, and the information about ADs at the ICU in Latin America is scarce,3 ,7–9 the aim of this study was to describe factors related to mortality during ICU stay in patients with ADs assessed in a single-centre in Bogota, the capital of Colombia.
Materials and methods
Study design
A retrospective case series review was performed from 1 February 2013 to 31 January 2014 for all adult patients with ADs evaluated by the Center for Autoimmune Disease Research (CREA) at the ICU in Mederi Hospital Universitario Mayor, a tertiary hospital in Bogota, Colombia. The hospital provides 828 beds, of which 120 are at the ICU (ie, medical, surgical, cardiac, neurological, others). The main general criteria for admission to the ICU are unstable conditions (ie, respiratory failure, haemodynamic collapse) or risk of an unstable condition. Every clinical record was fully evaluated to determine past medical history and outcome. Records of patients were systematically reviewed using a protocol that sought information on demographics, clinical and laboratory characteristics. Classification criteria were considered to include the following ADs: SLE, RA, SV, scleroderma (SSc), and Sjögren’s syndrome (SS).10–15 Dermatopolymyositis (DPM) was classified by using Dalakas and Hohlfeld criteria.16 For antiphospholipid syndrome (APS) and autoimmune hepatitis (AIH), the 2006 updated classification criteria17 and the international AIH group criteria18 were used, respectively. In addition, other ADs were evaluated according to the respective classification criteria (ie, autoimmune thyroid disease, AITD).19 For patients admitted more than once to ICU in the same hospitalisation, only the first ICU admission was considered.
Variables
The causes of ICU admission were classified as follows: (1) infection, (2) flare-up of AD, (3) complications derived from the underlying AD (ie, cardiovascular disease (CVD)), (4) adverse effects of immunosuppressors and (5) acute serious illnesses that were unrelated to the autoimmune condition. Infection was defined as a process characterised by an inflammatory response to the presence of micro-organisms (MOs) or the invasion of normally sterile host tissue by those MOs. Sepsis and septic shock were defined in accordance with the Surviving Sepsis Campaign Guidelines 2012.20 ADs flare-up were defined as an exacerbation of a pre-existing AD condition.21–26 Complications were acute serious illnesses that are altered or magnified by ADs. The acute conditions triggering ICU admissions were classified as follows: (1) respiratory failure, (2) haemodynamic collapse and (3) others (ie, postoperative, metabolic failure, neurological risk, risk of respiratory failure or haemodynamic collapse).
Other data recorded were age, gender, duration of disease, polyautoimmunity (ie, the presence of more than one AD in a single patient) including multiple autoimmune syndromes (MASs) when three or more ADs coexisted.27–29 Comorbidities, immunosuppressors in the past 3 months, the time between hospital admittance and ICU admission (ie, length of hospital stay before ICU admission), length of ICU stay, the need of intensive care support (ie, mechanical ventilation (MV), vasopressor support, dialysis, plasmapheresis, blood transfusion) and the reduction in left ventricular ejection fraction using the definition available from American Heart Association for heart failure,30 were also variables registered. Pulmonary hypertension corresponded to a pulmonary arterial systolic pressure >50 mm Hg measured by transthoracic echocardiography.31 Abnormal acid–base blood balance was also recorded and dichotomised as normal or abnormal based on the Siggaard-Andersen nomogram.32 The classification of Vincent et al33 was used for shock. Other variables recorded were the Acute Physiology and Chronic Health Evaluation II (APACHE II) score,34 the organ dysfunctions and/or infection score,35 the sequential organ failure assessment score (SOFA),36 the PaO2:FiO2 ratio of arterial oxygen tension to inspired oxygen concentration according to the values for Acute Respiratory Distress Syndrome37 and the Glasgow scale.38 Finally, the treatment of AD during ICU was also registered.
Statistical analysis
The mixed-cluster methodology proposed by Lebart et al39 based on multivariate descriptive methods such as principal component analysis and multiple correspondence analysis was performed to summarise sets of related variables with strong associations and common clinical context. Thus, by means of this clustering technique, for each set of related variables, new cluster variables (NCVs) were derived. For example, length of hospital stay before ICU admission and length of ICU stay, two variables with a non-linear relation, yielded a NCV (ie, ‘Time ICU’) which corresponds to a categorical variable with three outcomes (see results).
The χ2 and Fisher's exact tests were performed to established differences between categorical variables (original and NCV) and mortality. Kruskal–Wallis test was performed for assessing possible differences in continuous variables on mortality status. Statistical analysis was performed in R 3.0.2.40
Results
During the time period study (ie, February 2013 to January 2014), 485 hospitalised patients were evaluated by the CREA, of whom 79 were seen at the ICU. Of these, 50 were selected for analysis as they fulfilled the inclusion criteria of AD, the other 29 patients were excluded because they did not fulfil the classification criteria of AD.
Baseline patient characteristics are shown in table 1. Most of the patients were women (78%). The mean duration of ADs was 49.43±79.48 months (data were missing in three patients), and the mean length of stay in ICU was 10.96±11.06 days. The most frequent ADs were SLE, SSc and RA observed in 46%, 20% and 18%, respectively (table 2). There were 13 patients (26%) with polyautoimmunity, of whom 4 (8%) had MAS. Eleven patients were newly diagnosed as having AD during hospitalisation.
Characteristics of patients with ADs admitted to the ICU
Reasons of AD admission to ICU
Twelve patients (24%) did not survive during ICU stay and their causes of death were sepsis in five, intracerebral haemorrhages in two and upper gastrointestinal bleeding, cardiac tamponade and hemoperitoneum secondary to kidney biopsy in each one. In two patients the cause of death was not determined.
Sixteen patients (32%) did not have a previous comorbidity. Conversely, 13 patients (26%) had chronic kidney disease and 18 patients (36%) had CVD. Most of the patients were on steroids (n=33 (66%)). Otherwise, disease-modifying antirheumatic drugs (DMARDs) were registered in nine patients (18%), antimalarial in eight patients (16%), immunosuppressors (ie, azathioprine, cyclophosphamide, mycophenolate mofetil) in eight (16%), and three (6%) patients were on anti-tumour necrosis factor drugs (ie, adalimumab, etanercept and infliximab, respectively).
Infection was the most frequent (36%) cause of admission. Thirteen patients presented with septic shock as the cause of ICU admission (table 2). Total sepsis events were observed in 33 patients (66%). Seventeen patients become infected after ICU admission, and five patients developed septic shock after ICU admission. Urinary tract infection and pneumonia were the most frequent infections observed during ICU stay, and were the most frequent cause of sepsis (38% and 20%, respectively). Abdominal sepsis was registered in five cases (ie, gastrointestinal and gynaecological), of which four cases were associated with urinary tract infection and pneumonia. Two cases had infective endocarditis. Septicaemia without identifiable source was registered in two cases. In summary, 21 patients had one source of sepsis and 12 patients had two sources of sepsis due to different MOs.
The use of intravenous IgG (IVIG) and plasmapheresis was more frequent than the use of immunosuppressors (ie, cyclophosphamide and anti-CD20 monoclonal antibodies) as treatment for disease flare-ups.
Factors associated with poor outcome (ie, death) were length of hospitalisation before entry to ICU, low Glasgow scores and length of MV (table 1). In the survivor group, seven patients (18.4%) were discharged on haemodialysis and four patients (10.5%) deceased after ICU discharge. Five patients (13.2%) were readmitted to the hospital before 30 days of discharge.
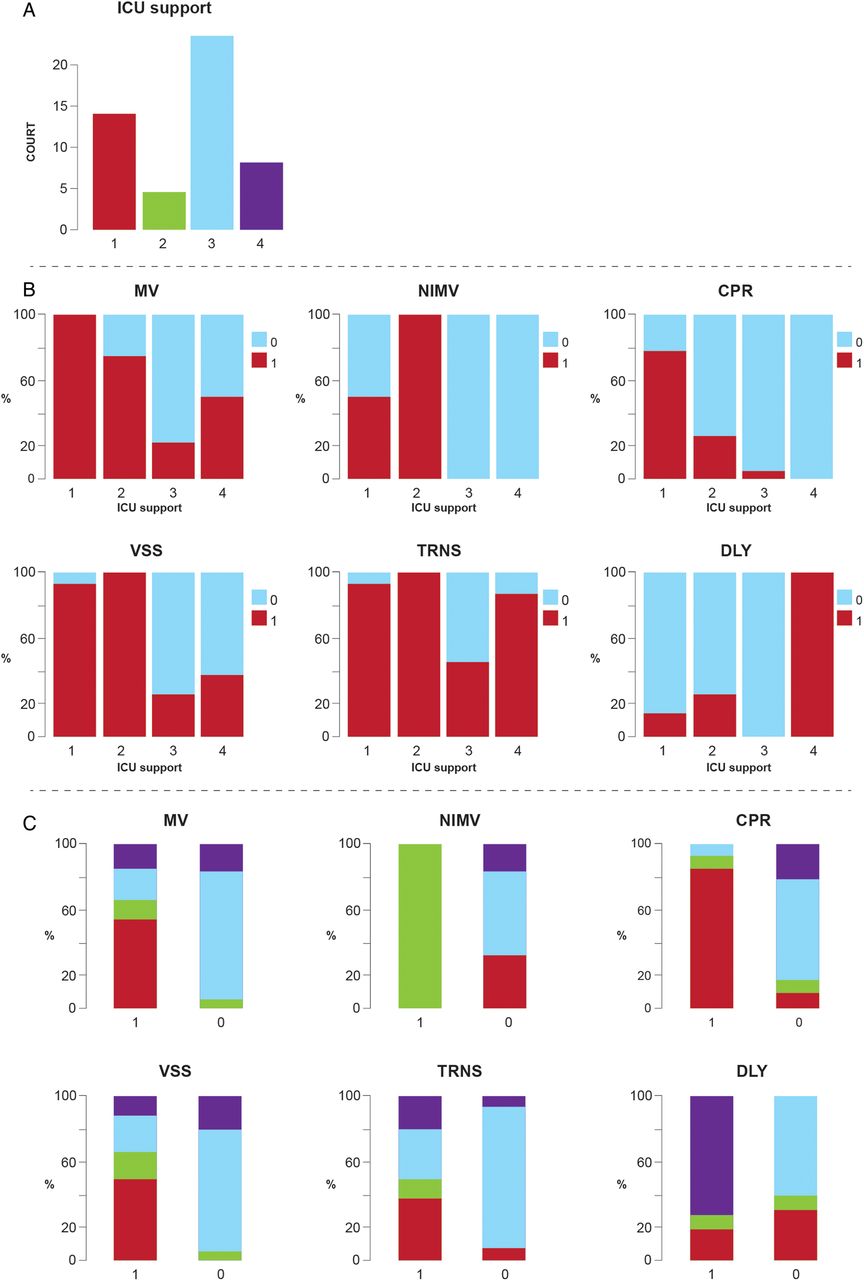
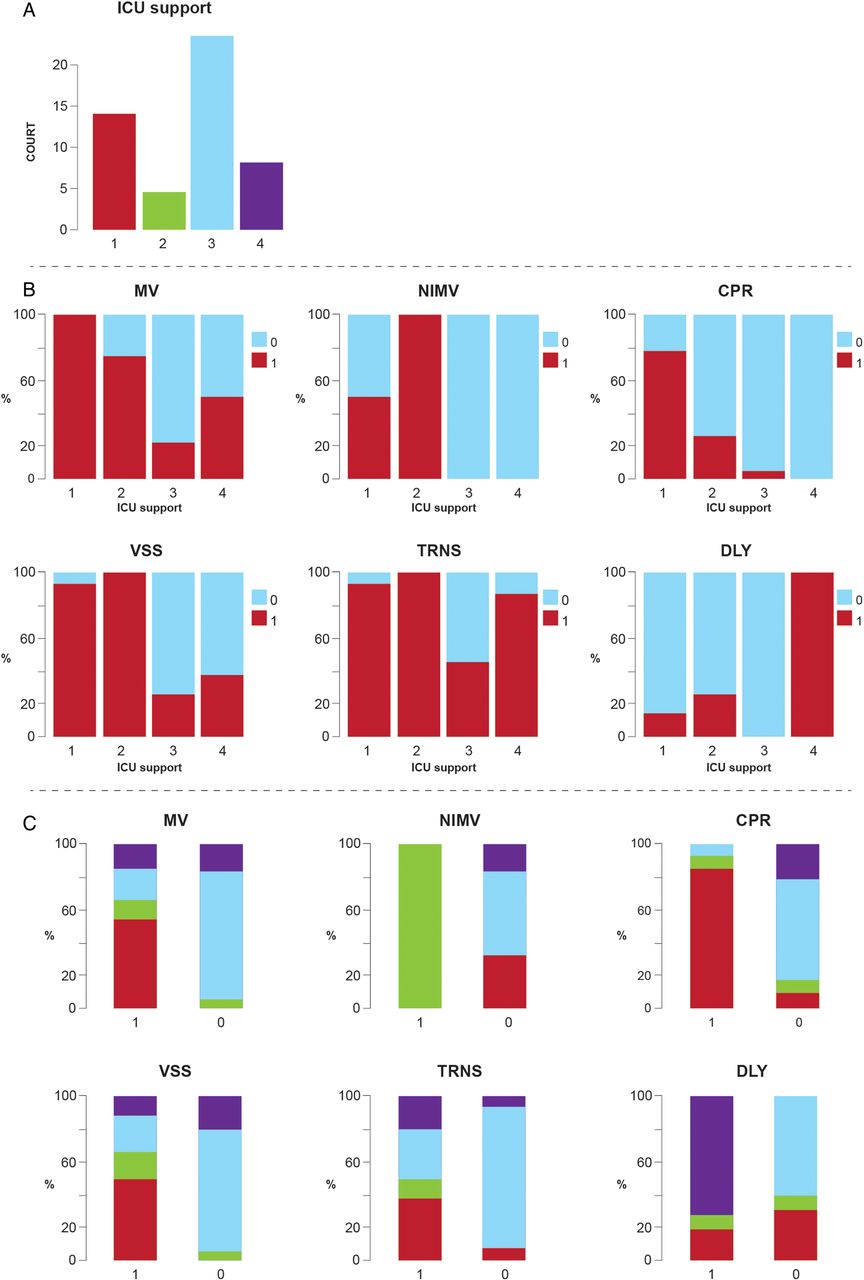
Two significant NCVs where found. First NCV was ‘Time ICU’ derived from length of hospital stay before ICU admission and length of ICU stay variables, which provided in turn three groups (figure 1). The second NCV was ‘ICU support profile’, derived from cluster analysis on outcomes of MV, non-invasive MV, cardiopulmonary resuscitation, vasopressor support, transfusion and dialysis variables. From this NCV, four groups where obtained (figure 2).
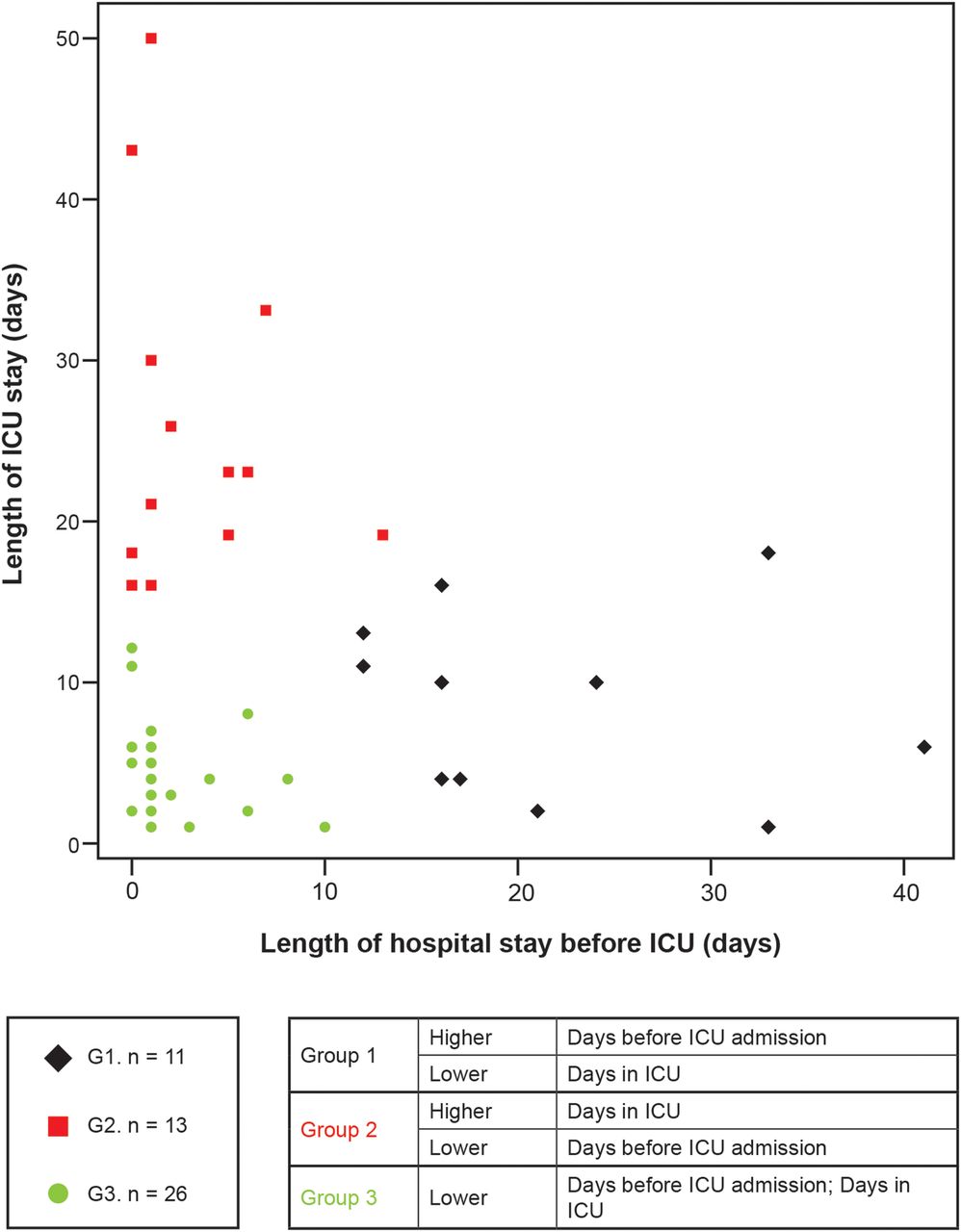
New cluster variable Time ICU. Within this cluster, three groups are observed, namely G1, G2 and G3. G1 was characterised by a short total ICU stay and long hospital stay before ICU admission. G2 had an opposite trend of that found in G1, that is, long total ICU stay and short hospital stay before ICU admission. Finally, G3 was related with short hospital stays before ICU and during ICU. Total days in ICU refers to the length of stay at ICU regardless the number of re-entries; Days before ICU admission refers to the length of hospital stay before ICU admission. ICU, Intensive care unit.
{kind=link}
{kind=link}
‘ICU support profile’ cluster. From this new cluster variable, four groups where obtained (A): (1) ICU support-G1, associated with high presence of all the studied supports except non-invasive mechanical ventilation and some sporadic dialysis; (2) ICU support-G2, associated with high presence of all the studied supports except CPR and DLY; (3) ICU support-G3, related with patients for whom little if any support was needed, and (4) ICU support-G4, associated with those patients requiring DLY and transfusion together with very few outcomes in other supports. (B) Profile of each group with respect to the original variables used to build the groups. (C) Profile of each original variable in terms of groups’ composition. 1: presence of the variable, 0: absence of the variable. CPR, cardiopulmonary resuscitation; MV, mechanical ventilation; NIMV, non-invasive MV; VSS, vasopressor support; TRNS, blood transfusion; DLY, dialysis.
For these two NCV we found that in Time ICU-G1 (short total ICU stay and long hospital stay before ICU admission) was associated with a higher risk of death in relation to Time ICU-G3 (short hospital stay before ICU and during ICU). Although this finding is explained by the association between mortality and long hospital stay before ICU admission (see table 1), this cluster analysis shows an interesting relation between total ICU stay and hospital stay before ICU admission. There were no patients with long duration on both variables. Patients in our study disclosed a long hospital stay before ICU admission and short ICU stay or vice versa. Similarly, ICU support-G1 (high presence of all the studied supports except non-invasive MV and dialysis) was associated with higher risk of death in relation to ICU support-G3 (little support needed) (table 1).
Discussion
The present study shows the 1-year characteristics and a mixed-cluster analysis of patients with ADs who required admittance to the ICU in a referral hospital in Bogota, Colombia. The most common diagnosis in our series was SLE, as has been already reported.3 ,7 ,8 However, the second AD was SSc, a result differing from previous studies.3 ,6–8 ,41 Although polyautoimmunity was frequently registered (26%), no significant influence of this condition on outcome was observed in this study. Our results indicate that in spite of the great progress on ICU resources and a better understanding of autoimmunity, there is still a high morbidity and mortality in patients with ADs seen at the ICU.
Known factors associated with mortality in patients with ADs admitted to the ICU are APACHE II, SOFA, length of stay, shock, comorbidities, vasopressors or immunosuppressive drugs.3 ,6 ,7 ,41–44 In our case series, the length of hospital stay before ICU admission, shock, vasopressors, MV, abdominal sepsis, Glasgow score and plasmapheresis were all factors associated with mortality.
Noteworthy, instead of considering each variable separately, we introduce the construction of NCVs as a novel methodology with the goal of establishing relevant clinical variables present together in a patient, since clinical manifestations do not appear isolated but rather in conjunction with others. With this approach, subgroups are identified allowing clinicians to better manage patients in real-life conditions.45
Previous studies and ours have identified that long hospital stay before ICU admission is a survival risk factor for patients with ADs.5 ,43 A delay in recognising patients with unstable conditions may worsen their survival rate. Thus, it is important to establish early detection programmes to identify patients at risk of mortality.20
The ICU support profile NCV disclosed four groups and represents life support manoeuvres (figure 2) used in the ICU. Some of these manoeuvres were already evaluated as individual variables; however, this analysis represent the interaction of groups of life support and the needed of life support due to organ failure (ie, worst prognosis).3 ,42 44 46 Plasmapheresis is a valuable treatment option for critically ill patients suffering antibody-mediated illness such as ADs and has been considered a relatively safe treatment of ICU patients.47 ,48 In the present case series plasmapheresis was associated with mortality, denoting severity of illness. Thus, this association should be considered as a bias (ie, confounding by indication).
Comorbidities in patients with ADs should be recognised as early as possible and treated promptly in the hope of avoiding systemic complications.3–5 ,49 Some important comorbidities such as CVD and chronic renal disease have a bad impact on the quality of life, patients’ survival and, as expected, increases the economic burden of disease.50 Nevertheless, in the present study comorbidities were not associated with mortality.
Previous works (table 3) have reported an ICU mortality ranging from 17% to 55%.3 ,6–8 ,41 ,42 ,44 ,46 ,50–53 In our study, the mortality rate was 24%, being one of lowest. Infections have ranged from 27% to 64%, and the flare up from 23% to 54%. These two are the main causes of ICU admission.3 ,6–8 ,41 ,42 ,44 ,46 ,50–53 Infection is favoured by immunosuppressive treatment and the immune response abnormalities inherent of ADs54–56 and may be developed in the community.57 An infection should always be ruled out at the time an AD flare-up is considered.3–5
ADs at the ICU (revision of the literature)
We would like to acknowledge the limitations of our study. Long-term survival of patients which has been related with a decrease in quality of life, disability and higher costs58 ,59 was not considered in the present work. In fact, four patients included in the total analysis died during the same hospitalisation once discharged from the ICU unit and were not consider into the ICU non-survivor group. Sample size precludes any inference of causality in the links between ICU mortality and related factors. Despite the meticulous study design, which was employed to control for confounding factors, the relation between plasmapheresis and non-survival could be attributed to confounding by indication due to hospital protocol.
Conclusion
We report a novel analysis of the outcome of patients with ADs admitted to the ICU. Detection of single factors and groups of factors from NCVs will allow implementation of early and aggressive therapies in order to avoid fatal outcomes.
Acknowledgments
The authors thank their colleagues at the Center for Autoimmune Diseases Research as well as Dario Pinilla and colleagues from the Mederi Intensive Care Unit at Mederi Hospital Universitario Mayor for their fruitful discussions and contributions to this work.
References
Footnotes
Contributors All the authors certifies that neither this manuscript nor the one with substantially similar content under our authorship has been published or is being considered for publication elsewhere (except as indicated in an attachment). We agree to allow the corresponding author to correspond with the editorial office to review the uncorrected proof copy of the manuscript and to make decisions regarding the release of information in the manuscript. The authors have given final approval of the submitted manuscript for which they take public responsibility for whole content.
Competing interests None declared.
Ethics approval Ethics Committee School of Medicine and Health Sciences, Universidad del Rosario, Bogotá, Colombia.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors have access to any data on which the manuscript is based and will provide such data on request to the editors or their assignees.