Article Text

Abstract
Objective Whether using provider-attributed end-stage renal disease (ESRD) cause of systemic lupus erythematosus (SLE) in national surveillance data captures the entire population of patients with SLE and ESRD remains uncertain. Our goal was to examine attributed cause of ESRD in US surveillance data among patients with SLE who have developed ESRD.
Methods Data from a national registry of treated ESRD (United States Renal Data System (USRDS)) were linked to the population-based Georgia Lupus Registry (GLR). The provider-attributed cause of ESRD was extracted from the USRDS for each validated patient with SLE in the GLR (diagnosed through 2004) who initiated treatment for ESRD through 2012. The percentage of these patients with SLE whose ESRD was subsequently attributed to SLE in the USRDS was calculated, overall and by patient characteristics.
Results Among 251 patients with SLE who progressed to ESRD, 78.9% had SLE as their attributed cause of ESRD. Of the remaining 53 patients, 43.4%, 18.9% and 15.6% had ESRD attributed to hypertension, diabetes mellitus type II and non-SLE-related glomerulonephritis, respectively. Attribution of ESRD to SLE was higher among patients aged ≤30 (87.9–93.9%) vs >30 (52.6%; p<0.001) but did not differ by sex or race. Having Medicaid (86.2%) or no insurance (93.5%) was associated with greater attribution of ESRD to SLE than having private insurance (72.5%; p=0.02), as was having two or more providers state a diagnosis of SLE (89.0% vs 73.5% with a rheumatologist diagnosis alone; p=0.008).
Conclusions These estimates indicate that USRDS-based studies may underreport ESRD among US patients with SLE. However, observed patterns of differential attribution of ESRD cause, particularly by age, suggest that providers may be correctly attributing ESRD to causes other than SLE among some patients with SLE.
- Epidemiology
- Lupus Nephritis
- Health services research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Among 251 systemic lupus erythematosus (SLE) patients from a U.S. population-based registry, who subsequently progressed to end-stage renal disease (ESRD), 79% had SLE as their attributed cause of ESRD in national administrative data.
Attribution of ESRD to SLE was higher among younger patients (88–94% and 53% among patients aged <30 and >30 years, respectively) but it did not differ by sex or race.
These estimates indicate that national studies that rely on administrative data may underreport ESRD among SLE patients, particularly among older SLE patients.
Introduction
The study of US patients with end-stage renal disease (ESRD) attributed to systemic lupus erythematosus (SLE) is possible through the United States Renal Data System (USRDS).1 The USRDS captures all treated ESRD in the USA, due to the universal Centers for Medicare & Medicaid Services (CMS) coverage of ESRD treatment for Social Security-eligible patients, regardless of patient age or disability status. The USRDS includes data on the provider-attributed cause of ESRD from the CMS ESRD Medical Eligibility Form 2728 (CMS-2728), which is required for all treated patients with ESRD. Several investigators have leveraged these data to estimate the population-based incidence of SLE-attributed ESRD2–5 and to demonstrate disparities in this incidence by age,4–6 sex,4 race,2 ,4–6 socioeconomic status,7 ,8 access to care9 and geography.4 ,6 Our group also recently examined wait time to transplant and graft failure10 and quality of ESRD care11 ,12 in patients with ESRD attributed to SLE using the USRDS.
However, the degree to which this method, which relies upon provider identification of SLE as the cause of ESRD at the start of treatment, captures the entire population of patients with SLE and ESRD remains uncertain. One prior validation study13 conducted using biopsy samples prior to 2001 suggested potentially low sensitivity of this attributed cause. Recently, we linked the population-based Georgia Lupus Registry (GLR)14–16 to the USRDS to estimate ESRD incidence among patients with SLE in metropolitan Atlanta.17 Using these linked data, we aimed to examine the attribution of ESRD cause among patients with known SLE who had progressed to ESRD.
Patients and methods
Data sources and study population
GLR. The primary aim of the GLR was to more accurately estimate the prevalence and incidence of SLE in 2002–2004 in Atlanta, Georgia (Fulton and DeKalb Counties).14–16 Investigators partnered with the state health department under a public health surveillance exemption to the Health Insurance Portability and Accountability Act to comprehensively search for and review cases. Potential SLE cases were identified from multiple sources, including hospitals; providers in rheumatology, dermatology and nephrology; commercial and hospital-based laboratories; regional pathology laboratories; lupus research databases and population databases, including the USRDS, Veterans Affairs data, Medicaid claims data, and state mortality and hospital discharge data. The presence of a suggestive pathology report, laboratory test and/or diagnostic code (International Classification of Diseases, 9th revision (ICD-9)) for SLE (710.0) or related conditions that might evolve into SLE—including discoid lupus (695.4), other specified connective tissue disease (710.8) and other unspecified connective tissue disease (710.9)—in any of these sources flagged patients as potential SLE cases.16 Medical records for all potential cases with residence in Fulton or DeKalb County in 2002–2004 were fully abstracted by trained abstractors. Patient date of SLE diagnosis, fulfilment of classification criteria, age, sex, race and other abstracted medical information were available in the GLR. The project was reviewed and approved by the Emory University and Georgia Department of Public Health Institutional Review Boards.
USRDS. The USRDS data1 originate primarily from the CMS and the United Networks for Organ Sharing. Date of initiation of ESRD treatment (through 30 September 2012), attributed cause of ESRD, age and insurance at ESRD start, and pre-ESRD nephrology care (2005+ only) were obtained from the USRDS. The USRDS also provided inpatient diagnostic codes for any hospitalisations ≥90 days after ESRD start (when Medicare coverage is established for all patients with ESRD, regardless of initial insurance). Up to ten discharge codes for each hospitalisation event were available.
US Census. Publicly available data on characteristics of US residential neighbourhoods, as defined by census tracts, were obtained from the 2000 US Census ( http://www.census.gov) via the Minnesota Population Center (http://www.nghis.org).18 Aggregate census tract-level data on racial composition, education and poverty were extracted.
Data linkage. Identifiers (Social Security number, date of birth, sex, first name and surname) on incident patients with SLE from the GLR were sent to the USRDS for a probabilistic match to identify those who progressed to ESRD from diagnosis of SLE (2002–2004) to the last date of follow-up currently available from the USRDS (30 September 2012). First patient residential addresses from the GLR were geocoded, which identified the census tract for spatial linkage with Census data. The GLR-USRDS data linkage was approved by the Emory Institutional Review Board.
Study population. SLE cases were defined by a combined case definition previously described:14 (1) the presence of ≥4 American College of Rheumatology (ACR) criteria19 in the medical record, or (2) the presence of three ACR criteria plus a treating, board-certified rheumatologist's final diagnosis of SLE; or (3) <4 ACR criteria plus a biopsy consistent with class II–VI lupus nephritis. Among the 1666 SLE cases by this definition in the GLR, 284 (17.0%) were identified in the USRDS as having started ESRD treatment in the USA between 1 January 1979 and 30 September 2012. Patients whose ESRD treatment start date preceded their SLE diagnosis date (n=31) or who lacked an attributed cause of ESRD (n=2) were excluded, leaving 251 patients with SLE for the analysis of attributed ESRD cause.
Study variables and definitions
Attributed cause of ESRD. The attributed cause of ESRD was defined by the single ICD-9 code listed on the CMS-2728, which is completed by the dialysis provider (usually the nephrologist) within 45 days of dialysis start. Attribution to SLE was defined by CMS-2728 ICD-9 code 710.0.
Patient characteristics. Patient demographics, including age at SLE diagnosis, sex, race and ethnicity, were obtained from the GLR. Age at ESRD start was available from the USRDS. Census tract-level sociodemographic variables, including percentage black residents, percentage residents living below poverty and percentage residents not completing high school, were available from the US Census and were assigned to individuals based on patient residence at the time of GLR data collection (2002–2004). Insurance at the start of ESRD (private, Medicaid, other and none) and reported pre-ESRD nephrology care (collected 2005+ only) were available from USRDS data, via the CMS-2728.
Duration of SLE prior to ESRD start was calculated as the time from date of SLE diagnosis (from GLR) to the date of ESRD start (from USRDS). Information on whether patients had renal biopsies prior to 2004, physician-stated SLE-related diagnoses and ACR criteria were obtained from the GLR. The 11 ACR criteria19 were defined by medical record-extracted data, available through 2004.
Statistical analysis
Overall patient characteristics were summarised by means, medians or percentages, as appropriate. Attribution of ESRD to SLE was defined as the percentage of patients with SLE who progressed to ESRD whose providers recorded SLE as the cause of ESRD on their CMS-2728. All attributed causes were tabulated, and attribution of ESRD cause was examined by patient characteristics. The effects of (1) using inpatient ICD-9 diagnostic discharge codes for hospitalisations subsequent to ESRD treatment initiation, in addition to the provider-attributed cause on the CMS-2728 and (2) restricting the population to those with biopsy-proven lupus nephritis on capture of SLE cases were also examined. Stata V. 14 (StataCorp, College Station, Texas, USA) was used for all analyses.
Results
Characteristics of patients with SLE who developed ESRD
Overall, the mean age at SLE diagnosis among 251 Atlanta-area patients with SLE who had ESRD was 25 years, with a third being <18 years (table 1); on average, patients were 39 years old when they started ESRD treatment. Table 1 shows that the majority were female (85%) and black (92%) and that these patients lived in neighbourhoods that were predominantly black (median, 89% of residents in census tract). Patients’ residential neighbourhoods also had median values of 11% and 13% of residents living below poverty and not finishing high school, respectively. Most patients had private insurance (40%) or Medicaid (28%) at the start of ESRD; 14% were not insured (table 1). Most were diagnosed with SLE by a rheumatologist, either alone or in combination with a nephrologist or dermatologist, and 69% had had at least one renal biopsy (table 1). Among patients with at least one biopsy, 149 (86.1%) had a biopsy consistent with lupus nephritis. The median duration of SLE prior to the start of ESRD treatment was 8 years, and 32% and 43% had had SLE <5 and >10 years, respectively, prior to ESRD start (table 1). Most had a physician-stated diagnosis of SLE (88%) or SLE in combination with connective tissue disease (9%) (table 1). The most common ACR criteria met by these patients were renal (96%), ANA (95%), haematological (92%) and immunological (73%) (table 1).
Selected characteristics of 251 Georgia Lupus Registry patients who initiated treatment for ESRD (through 2012), on or after the date of SLE diagnosis, overall and by attributed cause of ESRD in the United States Renal Data System
Patients with ESRD attributed to SLE were younger at SLE diagnosis and more likely to have Medicaid than patients with ESRD attributed to other causes; no differences by race, sex or neighbourhood sociodemographics were noted (table 1). Having an SLE diagnosis, having that diagnosis from more than specialist and having greater numbers of ACR criteria were all associated with greater likelihood of attribution of ESRD to SLE versus other causes (table 1). Among the individual criteria, malar rash, arthritis, immunologic criteria (positive anti-DNA, anti-Smith or anti-cardiolipin antibodies; positive Russell viper venom time/mixing test or false-positive syphilis), haematological criteria and photosensitivity (not statistically significant) were more common among patients with ESRD attributed to SLE versus other causes, whereas prevalence of renal, discoid rash and ANA criteria did not differ by attributed cause (table 1). Of patients with at least one biopsy, 90.1% vs 68.8% of those with ESRD attributed to SLE versus other causes had biopsies consistent with lupus nephritis.
Attribution of ESRD cause in patients with SLE
Of the 251 ESRD cases, 198 (78.9%) were attributed to SLE on the CMS-2728 (table 2 and figure 1A). Most of the 53 of 251 ESRD cases that were not attributed to SLE were attributed to hypertension (HTN) (23/53, 43%) and diabetes mellitus type II (10/53, 19%), with 8 (16%) patients having ESRD attributed to non-SLE glomerulonephritis (figure 1A). Among patients with SLE who also had CMS hospitalisation data subsequent to ESRD start (n=196), capture of SLE increased from 77% by CMS-2728 alone to 91% and 96% by CMS-2728 or the presence of inpatient diagnostic discharge codes for SLE (in two or more hospitalisations or at least one hospitalisation, respectively; table 2). Among the 149 cases with biopsy-defined lupus nephritis in the GLR through 2004 who subsequently developed ESRD, 85.2% had their ESRD attributed to SLE in national surveillance data. In contrast, among the 24 patients with biopsy data that were not consistent with lupus nephritis and 78 patients without biopsy data, 58.3% and 73.1%, respectively, had their ESRD attributed to SLE (p=0.004).
Identification of SLE by attributed cause of ESRD in the USRDS combined with inpatient diagnostic codes, among Georgia Lupus Registry (GLR) patients who initiated treatment for ESRD (through 2012) and were subsequently hospitalised
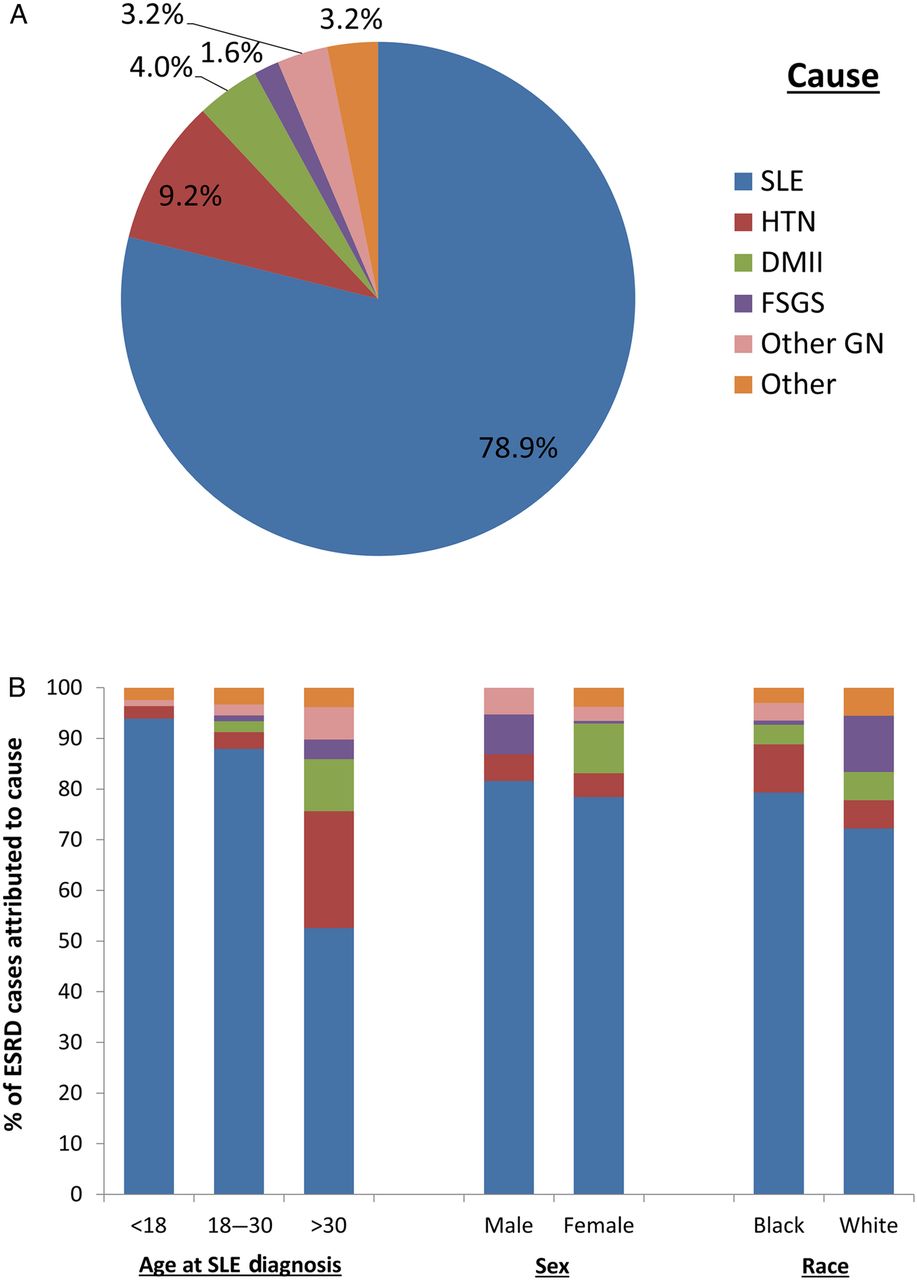
Attributed cause of end-stage renal disease (ESRD) among 251 patients with SLE in the Georgia Lupus Registry who progressed to ESRD (1979–2012), overall (A) and by age, sex and race (B). SLE, systemic lupus erythematosus; HTN, hypertension; DMII, diabetes mellitus type II; FSGS, focal segmental glomerulosclerosis; other GN, glomerulonephritis not attributed to SLE. Other includes tubular necrosis, IgA nephropathy, scleroderma, diabetes mellitus type I, multiple myeloma, other renal disorder and uncertain aetiology.
Differential attribution of ESRD cause by patient characteristics
Attribution of ESRD to SLE was higher among patients aged ≤30 (88–94%) compared with patients aged >30 (53%; p<0.001; table 3). Among those aged >50 (n=15), only three (20.0%) had their ESRD attributed to SLE. Attribution of ESRD to SLE did not differ by sex, race or neighbourhood sociodemographics (table 3). Among the 149 patients with biopsy-proven lupus nephritis prior to 2004, black patients with SLE-ESRD did have higher attribution of their ESRD to SLE than their white counterparts (86.5% vs 62.5%), but the difference was not statistically significant (p=0.10). Those with Medicaid (86%) and no insurance (94%) were more likely than those with private (73%) or other (71%) insurance to have their ESRD attributed to SLE (p=0.02; table 3). There was a non-statistically significant trend towards higher attribution of ESRD to SLE among patients with renal biopsies (table 3). Attribution of ESRD to SLE was highest among those diagnosed with SLE by a nephrologist (82%) or by a combination of providers (89%; table 3). Diagnosis of SLE without other connective tissue disease was also associated with high attribution (84% vs 46% among those with SLE and other connective tissue disease; table 3). There was a trend towards higher attribution of ESRD to SLE among patients with more severe disease by ACR criteria, but the differences were not statistically significant; however, attribution of ESRD to SLE was particularly high among patients with malar rash (88%) and photosensitivity (89%; table 3). There were no trends over time by year of ESRD start (table 3).
Attribution of ESRD to SLE in the USRDS, among GLR patients who initiated ESRD treatment through 2012, overall and by patient characteristics
The majority of the attributions of ESRD to HTN (18/23, 78.3%) and diabetes mellitus type II (8/10, 80.0%) were among patients aged >30 years (figure 1B). Among those aged >50 years, 13% and 60% of ESRD cases were attributed to diabetes mellitus type II and HTN, respectively. ESRD was more commonly attributed to diabetes mellitus II among females than males and to HTN among blacks than whites (figure 1B).
Among those 53 patients with SLE whose ESRD was not attributed to SLE, 46 had hospitalisations subsequent to ESRD; of these, 21 (45.6%) did not have diagnostic codes for their non-SLE attributed ESRD cause for any of their hospitalisations. However, this varied by attributed cause: only 5.0% of patients with HTN as cause did not have matching codes in their hospitalisation data, vs 33.3%, 62.5% and 100% of patients with ESRD attributed to diabetes mellitus type II, focal segmental glomerulosclerosis (FSGS) and glomerulonephritis, respectively (figure 2). Overall, 97.8% of patients with non-SLE attributed causes of ESRD had at least one hospitalisation with a code for SLE.

{kind=link}
{kind=link}
Presence of inpatient diagnostic codes for attributed cause of end-stage renal disease (ESRD) among 46 patients with systemic lupus erythematosus (SLE) in the Georgia Lupus Registry who progressed to ESRD (1979–2012) and had subsequent hospitalisations but whose ESRD was not attributed to SLE. HTN, hypertension; DMII, diabetes mellitus type II; FSGS, focal segmental glomerulosclerosis; other GN, glomerulonephritis not attributed to SLE. Other includes tubular necrosis, IgA nephropathy, scleroderma, diabetes mellitus type I, multiple myeloma, other renal disorder and uncertain aetiology.
Discussion
We found that, among a population of patients diagnosed with SLE in Atlanta through 2004 who subsequently started treatment for ESRD, attribution of ESRD cause to SLE using the CMS-2728 was 79%. This means that approximately one in five patients with SLE who progress to ESRD may be missed when the USRDS is used to identify the population of US patients with SLE who have developed ESRD. A prior validation study that compared biopsy results from a Southeastern registry (with data on glomerular disease biopsies performed in 1979–2000) and CMS-2728-attributed causes showed that only 27% of patients with a biopsy indicating SLE had SLE as their attributed ESRD cause13—much lower than both our overall estimate and the more directly comparable estimate of attribution of ESRD to SLE among patients with biopsy-proven lupus nephritis (85%). The small sample size (n=30 biopsies indicating SLE) and more complete data on attributed cause of ESRD likely explains some of these differences, since the prior study considered missing attributed cause to be a mismatch and the attributed cause was missing in more than half of the cases.13
We have provided an updated estimate of the sensitivity of USRDS data in capturing the US population of patients with SLE and all-cause ESRD. However, without a gold standard that provides a definitive diagnosis for each GLR patient (eg, renal biopsies) prior to ESRD start, we cannot estimate the sensitivity of this method to capture ESRD that is truly due to SLE. Further, we are unable to determine the population of patients with ESRD living in Atlanta during the same time at risk for ESRD (rather than just at ESRD start) as the GLR patients, due to unknown residential mobility in and out of the area over time. We also cannot identify individuals who are not in the GLR who have ESRD attributed to SLE in the USRDS (potential false-positive cases), among the same source population from which the GLR was drawn. Thus, we cannot properly perform a true validation study and estimate other important aspects of validity of CMS-2728-attributed cause, including the specificity (probability that patients with ESRD without SLE will have their ESRD attributed to non-SLE causes) and the positive predictive value (probability that a patient with SLE-attributed ESRD actually has SLE).
The addition of diagnostic codes from CMS-covered hospitalisations subsequent to ESRD start to the CMS-2728 in identification of patients with SLE with ESRD increased capture of patients with SLE from 79% to >90%. However, diagnostic codes may be unreliable, and this method of identifying patients with SLE with ESRD to increase capture may be especially problematic in patients with SLE, who are not likely to have Medicare coverage prior to the start of ESRD (based on age ≥65 years or disability). Thus, hospitalisations that take place prior to ESRD start and before Medicare eligibility is established may be captured differentially. Additionally, these patients are likely to have secondary insurance that may cover hospitalisation costs, may lose ESRD coverage 3 years after kidney transplantation,20 or may die soon after ESRD start. Further, not all patients will be hospitalised after ESRD start. We found that 21% of these patients did not have any claim data for Medicare-covered hospitalisations subsequent to ESRD.
Attribution of ESRD to SLE was greatly reduced among older patients (53% among those aged >30 and only 20% among those aged ≥50). This is likely to reflect increasing comorbidity in older patients with SLE, particularly HTN and diabetes, which are, by far, the most common causes of ESRD in the general population1 and which are common in SLE, due to metabolic effects of chronic inflammation, steroid treatment or both.21–25 In fact, we found that many patients with non-SLE attributed ESRD causes such as HTN had subsequent inpatient codes for these conditions. This observation would suggest that these patients were likely to have the conditions listed as their attributed ESRD cause and that the non-SLE ESRD cause attributed by the provider may not have always been incorrect, even if it did not capture the SLE status of the patient. Studies of older patients with SLE-ESRD should recognise the limitation that patients with SLE with other comorbidities that are associated with ESRD may not be captured using only the dialysis provider-attributed cause of ESRD.
Age was associated with the most striking differences in attribution of SLE cause, but we generally did find differential attribution by other patient characteristics. While we did find that black patients with SLE who progressed to ESRD were more likely than their white counterparts to have their ESRD attributed to SLE (79% vs 72%), and that this difference was more pronounced among those with biopsy-proven lupus nephritis (87% vs 63%)—suggesting provider perceptions may play a role in recognition of SLE at ESRD start—neither difference was statistically significant. This is likely at least partially due to the small sample size of white patients progressing to ESRD in the GLR (n=18). Blacks were also more likely than whites to have their ESRD attributed to HTN rather than SLE. While attribution of ESRD cause to SLE was not differential by sex overall, females were more likely than males to have their ESRD attributed to diabetes mellitus type II. Having Medicaid or no insurance was associated with greater attribution to SLE than private insurance, which may partially reflect the ages of the patients with each type of insurance.
Interestingly, among those patients with pre-ESRD nephrology care information, those without nephrology care were more likely to have their ESRD attributed to SLE, although this association was not statistically significant. Nephrologists may be more likely to be aware of renal biopsy results that indicate non-SLE-related kidney disease and also to provide care pre-ESRD and post-ESRD start and thus attribute ESRD to other comorbid causes. Having at least two providers stating the diagnosis was associated with ESRD being attributed to SLE nearly 90% of the time, vs 73% with a rheumatologist alone, indicating the potential importance of communication between providers in recognition of SLE in ESRD. More severe SLE and biopsy history were associated with higher attribution of ESRD to SLE, relative to milder SLE and no biopsies performed, but these associations were not statistically significant. Longer duration of SLE prior to ESRD was not associated with greater attribution. More visible symptoms of SLE, including malar rash and photosensitivity, were associated with slightly higher attribution than other symptoms, but whether these symptoms persisted at ESRD start is unknown. Despite substantial changes to the CMS-2728 in 1995 and 2005, there was no increase in attribution over time.
Additional limitations deserve mention. First, these estimates may not be generalisable to other US SLE populations. We had limited power to detect differential attribution of ESRD cause by patient characteristics and particularly to stratify on or adjust for multiple covariates. Given the number of exposures assessed, it is possible that some statistically significant associations are due to chance alone. Non-CMS-eligible patients (eg, undocumented residents) and patients who moved out of the USA between SLE diagnosis and start of ESRD treatment would not be captured by USRDS. However, these estimates apply to studies with the same limitations. We also did not have data on individual socioeconomic status. Data on medications, including prescribed immunosuppressant medications and patient adherence to these regimens, were not available in the GLR. It is possible that younger patients were more often prescribed fertility-preserving immunosuppressant regimens and/or had lower adherence to their prescribed regimens, leading to more clinically apparent lupus nephritis at ESRD presentation and, thus, greater attribution of ESRD to SLE among this population. Only one cause is allowed per patient on the CMS-2728 form, which may decrease attribution to SLE: for example, FSGS could be secondary to lupus nephritis but still listed as the attributed cause of ESRD; these patients would remain uncaptured by attempts to identify the US SLE-ESRD population using data on the attributed cause, even if they are recognised by providers as patients with SLE. Finally, although renal biopsy information was collected, when available, in the GLR, attempts to validate non-SLE-attributed ESRD causes using biopsy data would be confounded by indication and subject to selection bias as well. Furthermore, since GLR case ascertainment ended in 2004, no clinical data, including biopsy results, are available after this time; even among patients with biopsy-proven lupus nephritis at a single time point, other conditions related to treatment or complications of SLE and lupus nephritis could still develop and lead to ESRD.
Despite these limitations, this study provides an updated estimate of sensitivity of USRDS data to capture US patients with SLE who have progressed to ESRD, regardless of cause. Additionally, our findings of differential attribution of ESRD cause by age and severity of SLE suggest that older patients or patients with milder cases of SLE, whose ESRD may be attributed to comorbid conditions—perhaps even resulting from prolonged SLE treatment—could have been excluded from previous studies based on attributed ESRD cause alone incidence of SLE-attributed ESRD.2–12 These results contribute to the appropriate interpretation of past and future US population-based studies of incidence and quality of care in ESRD patients with SLE.
Acknowledgments
Some of the data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the authors and in no way should be seen as an official policy or interpretation of the US government.
References
Footnotes
Contributors All contributors meet the criteria for authorship and approved the submitted version of the manuscript.
Funding This research was supported by the Lupus Foundation of America. The Georgia Lupus Registry was supported in part by the CDC, and by cooperative agreement CDC-RFA-DP08-806 and earlier by cooperative agreement PA03022 from the CDC. This publication was supported by the Grant or Cooperative Agreement Number, DP005119, funded by the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services.
Competing interests None declared.
Ethics approval The Emory University institutional review board and the Georgia Department of Public Health provided ethics approval for this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement USRDS data are publicly available by request (http://www.usrds.org). Census data, including the American Community Survey, are publicly available (http://www.census.gov or http://www.nhgis.org.)