Article Text

Abstract
Purpose Patients with systemic lupus erythematosus (SLE) have higher risk of developing a cardiovascular event than the general population, with multiple factors contributing to this increased risk, including systemic inflammation. We aimed to compare the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and other disease characteristics of SLE patients with and without left ventricular (LV) geometry abnormalities.
Methods This was a cross-sectional study nested of a SLE cohort. We recruited patients with SLE diagnosis according to the 2019 EULAR/ACR classification criteria, aged ≥ 18 years. A transthoracic echocardiogram was performed by two certified echocardiographers blinded to clinical information. Disease activity was assessed with SLEDAI. SLE patients with LV geometry abnormalities were included and matched by age and gender to SLE patients with normal LV geometry. Distribution was evaluated with the Kolmogorov-Smirnov test. Comparisons were performed with Chi-square or Fisher’s exact test for qualitative variables, and Student’s T-test or Mann-Whitney’s U-test for quantitative variables. A p-value < 0.05 was considered significant.
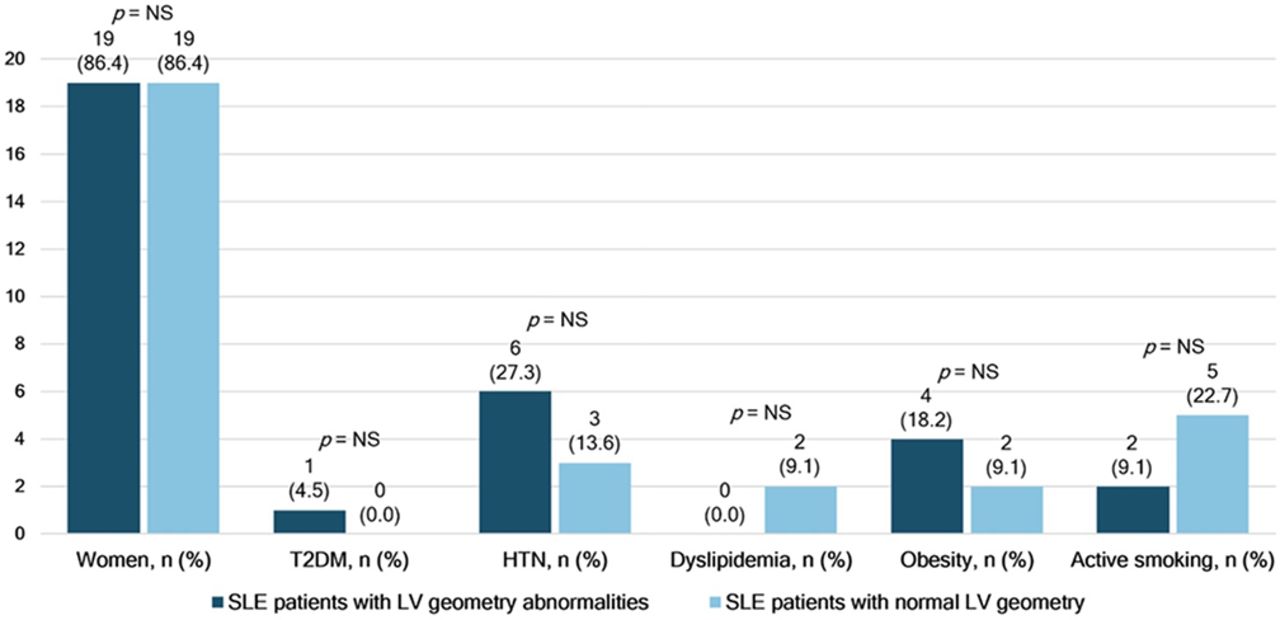
Results A total of 44 SLE patients were included, 22 with LV geometry abnormalities and 22 with normal LV geometry. Mean age of SLE patients with LV geometry abnormalities was 35.1 ± 12.2 years, compared to 35.4 ± 9.4 years of SLE patients with normal LV geometry, p = 0.923. There were no significant differences inn demographic characteristics between both groups. Demographic characteristics are shown in Figure 1. We found that SLEDAI was significantly higher in SLE patients with LV geometry abnormalities (26.45 vs 17.33, p = 0.016). Comparisons of clinical characteristics between groups are shown in Table 1.
Comparison of disease characteristic of SLE patients with and without LV geometry abnormalities
{kind=link}
Comparison of demographic characteristic of SLE patients with and without LV geometry abnormalities
Conclusions SLE patients with LV geometry abnormalities had higher SLEDAI than patients with normal LV geometry. A transthoracic echocardiogram may be useful detect early cardiovascular abnormalities in SLE patients with high disease activity, and therefore should be considered as part of the cardiovascular evaluation of these patients.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.