

Abstract
Objective. Intravenous cyclophosphamide (IV CYC) in combination with high doses of corticosteroids is considered the “gold standard” of therapy for lupus nephritis (LN). However, the optimal dose of corticosteroids needed has not been defined. We evaluated the efficacy of a monotherapy with IV CYC in patients with a first episode of LN (duration ≤ 6 months).
Methods. Forty patients with LN received IV CYC (12 pulses). Prednisone alone was administered and dose-adjusted to control extrarenal manifestations. Response after 24 months was defined as normalization of creatinine level, inactive urinary sediment, and proteinuria ≤ 0.2 g/day [complete response (CR)] or ≤ 0.5 g/day [partial response (PR)].
Results. CR was achieved in 25 (62.5%) and PR in 8 (20%) patients. Mean starting dose of prednisone was 23.9 ± 23.8 mg/day. In a posthoc analysis, we separately analyzed patients initially treated with prednisone doses ≥ 20 mg/day (Group A, n = 19) or < 20 mg/day (Group B, n = 21). CR was achieved in 52.6% (Group A) versus 71.4% (Group B; p = 0.37); and PR in 26.3% versus 14.3%, respectively (p = 0.58). During longterm followup (10.4 ± 3.1 yrs), 37.8% experienced a renal flare. Thirty patients (81%) still have normal renal function. Renal outcome was irrespective of initial prednisone doses (p = 0.46, Pearson chi-square test of independence).
Conclusion. Our rates of CR and PR and longterm outcomes were comparable with rates after treatment with a combination of IV CYC with high doses of corticosteroids. These data warrant randomized controlled trials evaluating different doses of corticosteroids in LN.
Nephritis is a common, serious manifestation of systemic lupus erythematosus (SLE)1. In 10%−30% of such patients, the kidney disorder progresses to endstage renal disease (ESRD) within 15 years of diagnosis1,2,3,4. Intravenous cyclophosphamide (IV CYC) is widely used as an effective but also toxic regimen that enables a high rate of disease remission and preserves kidney function5,6,7,8. Therapeutic strategies to reduce the toxicity of IV CYC have shown similar efficacy compared with the traditional US National Institutes of Health (NIH) IV CYC regimen9,10. All regimens include moderate to high doses of oral or intravenous corticosteroids (GC). However, the optimal GC dose needed for successful induction treatment has not been ascertained in randomized studies. GC themselves are known to be associated with severe side effects and contribute to about 25% of longterm damage in SLE11,12. In addition, the majority of studies report that the development of cardiovascular complications is associated with GC therapy13,14. Recent guidelines confirm the lack of evidence from randomized trials to support any particular regimen of GC use in either the induction or maintenance of lupus nephritis (LN)15,16. Thus, controversy remains over the optimal use of GC in terms of their effects on disease activity, clinical outcome, and/or associated toxicity.
Risk stratification allows identification of patients at lower risk for renal dysfunction, for whom less aggressive therapy is likely to be beneficial. For example, prompt diagnosis after the onset of nephritis and subsequent initiation of appropriate therapy is associated with improved outcomes regardless of the histologic subclass17,18. We hypothesized that in LN that is diagnosed early, high GC doses do not have significant clinical effect concerning the response to induction treatment and longterm renal outcome. Thus, the rationale of our study design was to avoid as much GC as possible. We therefore decided to refrain from use of not only oral GC but also methylprednisolone pulses. We prospectively studied the outcome of patients with LN who were treated with IV CYC and GC doses solely adapted to extrarenal disease activity.
MATERIALS AND METHODS
Patients
Patients with SLE according to the American College of Rheumatology (ACR) revised criteria19 and a first episode of LN (duration ≤ 6 months) were eligible for this study. Disease onset was defined as the time the patient fulfilled the ACR criteria for SLE. Disease duration was defined as the period from disease onset to the time of the baseline examination. The time of onset of nephritis was defined as the first clinically evident renal disease with proteinuria (> 0.5 g/day) and hematuria [> 5 dysmorphic red blood cells (RBC)/hpf]. Patients with severe extrarenal lupus [active cerebral lupus, severe hemolytic anemia (hemoglobin < 7 mg/dl), thrombocytopenia (< 50,000/mm3), or leukopenia (< 1000/mm3)] were excluded, because they received methylprednisolone pulse treatment. In addition we excluded those with a relapse of LN, patients with liver disease, and pregnant patients. Renal biopsy specimens were assessed by immunofluorescence and light microscopy and categorized according to the 1982 World Health Organization classification20.
Immunosuppressive treatment protocol
All patients received 12 IV CYC pulses over a period of 24 months (6 monthly pulses followed by 6 quarterly pulses). The initial CYC dose was 0.5 g/m2 body surface area; subsequent doses were increased by 250 mg according to the white blood cell (WBC) count nadir measured on Day 14, with a maximum of 1500 mg per pulse. In addition, all patients received mesna (sodium-2-mercaptoethane sulfonate) to prevent hemorrhagic cystitis. Hypertension was treated initially with angiotensin-converting enzyme inhibitors, unless contraindicated. The use and dose of prednisone was based solely on the presence of mild to moderate extrarenal SLE manifestations, with subsequent dose tapering based on extrarenal activity as considered necessary by the treating physician. No additional methylprednisolone pulse therapy was administered in any patient for induction of remission of LN.
Patients were evaluated monthly within the first 6 months and quarterly thereafter. At each visit, a complete physical examination was carried out including blood pressure as well as routine laboratory testing [blood count, urinalysis, 24-h urinary protein, serum creatinine, creatinine clearance rate, serum complement component 3 (C3) level, and anti-dsDNA antibody]. Disease activity was assessed using the Systemic Lupus Activity Measure (SLAM)21. Accumulated organ damage was measured according to the Systemic Lupus International Collaborating Clinics damage index (SLICC/ACR-DI)22. Adverse events (e.g., infections) were recorded.
The study was approved by the local ethics committee of the University of Duesseldorf and written informed consent was obtained from all patients.
Study endpoints
Complete response (CR) after 24 months (12 pulses of IV CYC treatment) was defined as proteinuria < 0.2 g/day together with inactive urinary sediment (≤ 10 RBC/μl, ≤ 10 WBC/μl, no cellular casts) and normalization of creatinine level for at least 3 months. Partial response (PR) was defined as proteinuria ≤ 0.5 g/day together with inactive urinary sediment and normalization of creatinine level for at least 3 months. Patients who did not meet these criteria were regarded as nonresponders. Renal flares during longterm followup were defined as persistent increase of proteinuria (≥ 500 mg/day) together with recurrence of active urinary sediment (increased hematuria with or without reappearance of cellular casts) and/or increase of serum creatinine (≥ 25%) due to active disease, which required more intense immunosuppressive therapy.
Statistical analysis
All statistical tests were performed with the R software version 2.12 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org). Descriptive statistics are reported as means ± SD, ranges, frequencies, or proportions as appropriate. The numbers (percentage) of responders and nonresponders were calculated for each factor, overall and by treatment group (prednisone < or ≥ 20 mg/day). Differences among study groups were analyzed by tests of equal proportions, Student’s t tests, and Pearson’s chi-square test of independence. Differences were considered statistically significant when 2-sided p values were < 0.05. Time to event analysis was performed according to the Kaplan-Meier method.
RESULTS
Baseline data and treatment
Between February 1995 and December 2004, 67 patients with SLE were diagnosed with active LN at the Department of Rheumatology. Twenty-six patients were not eligible for our study (19 had previously been treated for LN, 2 were pregnant, and 6 were critically ill with severe multiorgan involvement). A total of 41 patients met our inclusion criteria. One patient developed toxic hepatopathy after 2 IV CYC treatments and was therefore not included in the analysis. The remaining 40 patients were all white (33 women, 7 men), had a mean age of 29.7 ± 10.1 years, and had a mean SLE duration of 3.5 ± 2.8 years. Three (7.5%) presented with renal impairment (serum creatinine > 1.2 mg/dl) and 20 (50%) presented with a 24-hour urinary protein ≥ 2.5 g. Seven patients had previously been treated with azathioprine and 1 with cyclosporine. In 38 patients, the type of LN was verified by renal biopsy; in the remaining 3 patients no biopsy could be performed because of coagulation abnormalities. Baseline clinical and laboratory data are outlined in Table 1.
Characteristics of all patients with SLE at baseline. Results are mean ± SD or n (%).
Response after 24 months
All patients completed the entire course of therapy with statistically significant reductions from baseline of SLAM scores, hemoglobin, proteinuria, complement, and anti-dsDNA levels (Table 2). After 24 months, 25 patients (62.5%) met the criteria for CR and 8 (20%) for PR. Baseline data for complete and partial responders were comparable (Table 3). The group that achieved CR comprised fewer patients with 24-h urinary protein ≥ 2.5 g at baseline (40% vs 87.5%); however, this difference did not reach statistical significance (p = 0.053; Table 3).
Change of measures in all 40 patients during followup. Results are mean ± SD.
Differences at baseline between patients with or without response after 24 months. Results are mean ± SD or n (%).
Outcome in patients treated with different prednisone doses
The mean daily starting dose of prednisone was 23.9 ± 23.8 mg/day. To investigate any prednisone effect, we performed a subgroup analysis, comparing patients who had been treated with prednisone ≥ 20 mg/day at baseline [high-dose: 21 patients (52.5%)] or prednisone < 20 mg/day [low-dose: 19 patients (47.5%); Table 4]. As expected, patients in the high-dose group had significantly higher SLAM scores at baseline. These patients experienced arthritis and serositis more often, had significantly lower hemoglobin, and had lower levels of complement C3 (Table 4). The mean cumulative dose of prednisone equivalents after induction treatment (Week 24) was 3.23 ± 1.37 g (high-dose group) and 1.46 ± 0.62 g (low-dose group). Of note, there were no statistical differences in the response rates when comparing patients of the 2 groups: CR was achieved in 52.6% versus 71.4% (p = 0.37) and PR in 26.3% versus 14.3% (p = 0.58) of patients in the high-dose and low-dose prednisone group, respectively (Table 4). Renal outcome was irrespective of initial prednisone doses as determined by Pearson’s chi-square test of independence (p = 0.46).
Differences between patients treated with prednisone < and ≥ 20 mg/day at baseline. Results are mean ± SD or n (%).
Adverse events during treatment period
We recorded at least 1 infection in 21 patients (52.5%). Major infectious complications included herpes zoster in 3 patients (7.5%) and 1 pneumonia caused by Mycoplasma pneumoniae treated in hospital. New onset of leukopenia (≤ 3000/μl) was diagnosed in 9 patients. We observed no significant differences concerning the rate of infections in relation to the initial prednisone dose [61.4% (high-dose) and 52% (low-dose)]. Permanent amenorrhea developed in 5 (15.1%) of 33 female patients (mean age at treatment 47 ± 19.2 yrs, range 19−66 yrs).
Longterm followup
All patients were evaluated regularly after completing the treatment protocol. Treatment following IV CYC consisted of hydroxychloroquine (HCQ) alone (18 patients), HCQ and mycophenolate mofetil (MMF; 13 patients), MMF alone (4 patients), and no specific SLE treatment besides low-dose prednisone (5 patients). Two patients died, 5 and 13 months, respectively, after the last IV CYC treatment. The cause of death in the first case was an anesthetic complication during termination of an unplanned pregnancy at age 26 years with otherwise stable SLE. In the second case, the cause of death was attributed to sepsis and treatment-resistant multisystem flare in a 21-year-old patient who had stopped all her medications prior to this event. One patient was lost to followup. The remaining 37 patients were followed for a mean of 10.4 ± 3.1 years. Fourteen (37.8%) of these 37 patients experienced a renal flare, 11 of them (78.5%) during the first 5 years after treatment. We could detect no significant differences concerning the flare rate in respect to longterm treatment.
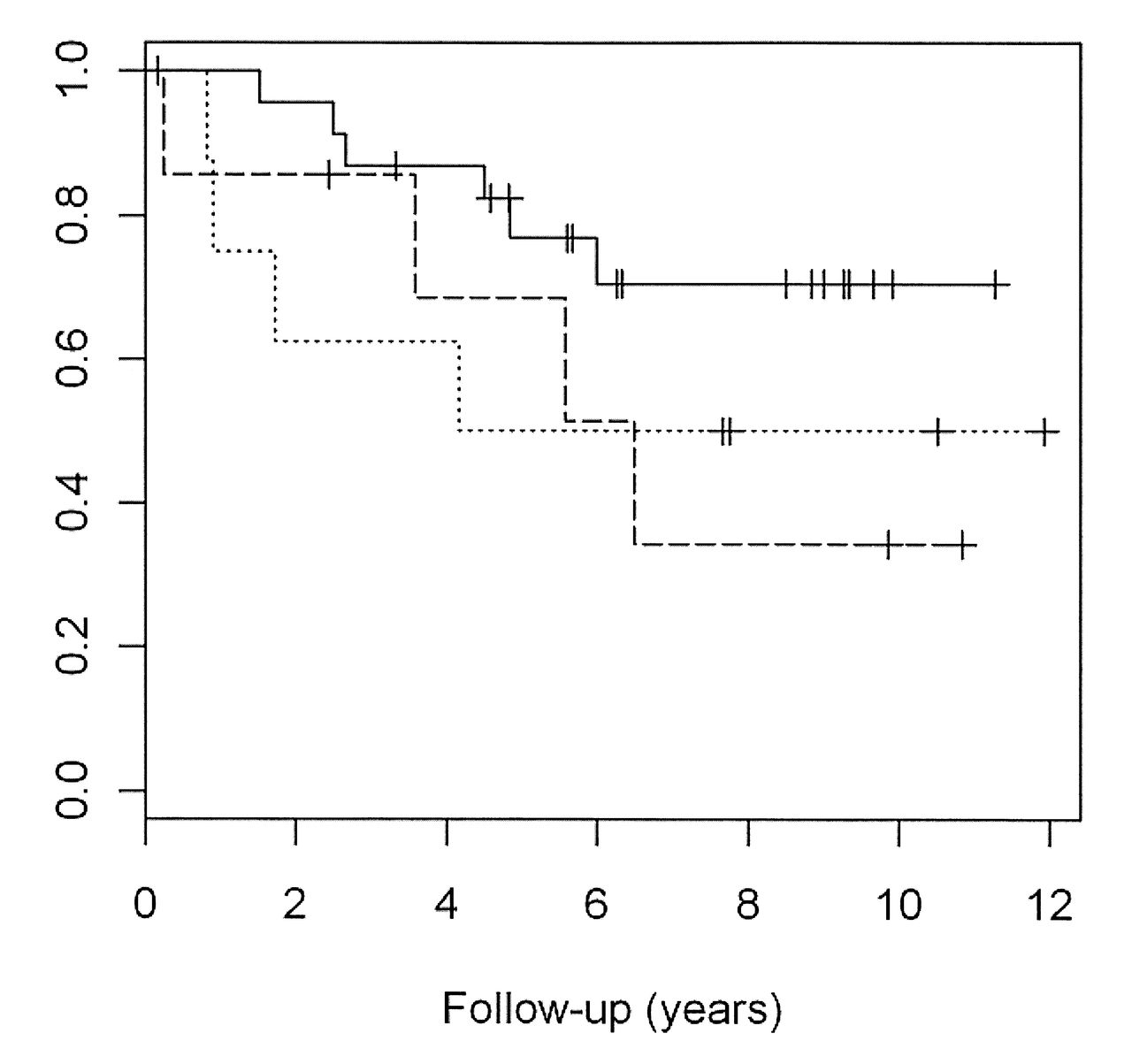
Six of the 25 patients with CR (24%) after IV CYC experienced a flare, compared to 4 of the 8 patients (50%) with PR and 4 of the 7 patients (57.1%) with no response. Dependence between response category and occurrence of renal flares was not significant (p = 0.16; Figure 1). The Kaplan-Meier curves shown in Figure 2 indicate that the cumulative probability of an absence of flare did not differ between patients in respect to the initial prednisone regimen. All patients who experienced a flare received additional immunosuppressive therapy (MMF, n = 12, or retreatment with IV CYC, n = 2). At the last investigation, 2 patients had developed ESRD and 5 patients developed doubling of serum creatinine. The mean serum creatinine of 35 patients who did not develop ESRD did not differ significantly regarding the initial prednisone treatment (1.06 ± 0.73 mg/dl in the low-dose and 1.45 ± 1.42 mg/dl in the high-dose group; p = 0.92).

Kaplan-Meier analysis of the probability of flare during longterm followup in patients achieving complete response (solid line), partial response (dotted line), or nonresponse (dashed line) after treatment. The HR for renal flare in the complete-response group compared with the nonresponse group was 0.39 (95% CI 0.11−1.4, p = 0.15) and 0.87 (95% CI 0.22−3.5, p = 0.85) compared with the partial response group.

Kaplan-Meier analysis of the probability of an absence of flare during longterm followup in patients treated with ≥ 20 mg prednisone (solid line) versus patients treated with < 20 mg prednisone at baseline (dotted line). The HR for renal flare in the low-prednisone group compared with the high-prednisone group was 0.73 (95% CI 0.25−2.12, p = 0.57).
Almost all patients (92%) were still treated with low-dose prednisone (mean 4.6 mg/day). The mean prednisone dose in these patients at baseline was 23 ± 22 mg/day. In addition, 67.5% were receiving HCQ, 32.4% MMF, and 5.4% azathioprine. No avascular necrosis was noted during longterm followup. One patient developed osteoporotic fractures. Two patients experienced symptomatic coronary artery disease (myocardial infarction). One patient with a long history of smoking developed lung cancer. Five female patients experienced 6 normal pregnancies.
DISCUSSION
In our prospective observational study, we report the outcome of 40 white patients with a first episode of LN treated with an induction regimen consisting of IV CYC without additional methylprednisolone pulses or high doses of oral GC commonly used for induction of remission. After 24 months, 25 patients (62.5%) met the criteria for CR and 8 patients (20%) for PR. Our study was neither designed nor powered to answer questions concerning specific predictors for complete or partial remission. While cross-study comparisons must be regarded with caution, the rates of response we observed were comparable with outcomes reported from studies using a combination of IV CYC with moderate to high doses of GC. In the NIH study, for example, renal remission at 5 years was obtained in 85% of patients in the methylprednisolone plus IV CYC combination group8. The Euro-Lupus Nephritis trial reported renal remission in 71% (methylprednisolone plus low-dose IV CYC group) and 54% (methylprednisolone plus high-dose IV CYC group) after a median of 41 months9. Definitions for CR and PR were similar in the 2 trials.
We report a mean followup of 10 years in 37 of 40 patients. It is well established that longterm followup is needed before conclusions can be drawn regarding efficacy of any immunosuppressive regimen over another in avoiding ESRD in LN5. At the time of the last examination, 81% of our patients had normal serum creatinine. Rates of ESRD were low in our cohort (5.4%) and were in accord with studies investigating extended followup of > 10 years in patients with similar ethnic and disease background (5%−9% in the Euro-Lupus Nephritis trial)23. One explanation for this might be that 95% of our patients had proteinuria below 0.5 g/day at the end of the treatment protocol. Patients in whom control of proteinuria is achieved have much better renal survival rates at 5 and 10 years (94% for both in our study) than patients who fail to achieve remission (46% at 5 years, 31% at 10 years)24. Fourteen (37.8%) out of 37 patients experienced a renal flare, mostly during the first 5 years after treatment. This corresponds to flare rates of 28%−45% described in the literature, depending on duration of followup10,25,26,27,28,29. Again, we were not able to detect differences concerning the probability of flares in the 2 prednisone groups.
There are, however, some specific characteristics of our study population that influence the generalized applicability of our results. Clinical risk factors for disease progression, evident at the time of initial presentation, included elevated serum creatinine at the time of renal biopsy, hypertension, nephrotic range proteinuria, and black and Hispanic race and ethnicity10,28,29. Although 38 of our patients had biopsy-proven proliferative LN, only 6 (15%) presented with renal impairment and 20 (50%) with proteinuria ≥ 2.5 g/day compared with 64% and 62%, respectively, in the NIH study7. Second, the duration of nephritis before treatment was 6 months at the longest and we treated the first episode of LN in each patient. The mean duration of nephritis was 24 ± 6.9 months in the NIH study and 26% of patients enrolled in the Euro-Lupus Nephritis trial had a prehistory of renal disease8,9. The likelihood of a successful initial outcome is greater if therapy for LN is initiated relatively early in the course of the disease regardless of the histological subclass10,18. This issue was addressed in a study of 91 patients with LN who were followed for a median of 6 years. There was a much higher rate of ESRD among patients who had clinically recognized renal disease for ≥ 6 months prior to biopsy (47 vs 14 per 1000 patient-yrs in patients who had an earlier biopsy)18. Third, all patients in our study were white in contrast to the higher percentage of African Americans (20%−50%) randomized into the NIH studies or in recent randomized trials7,8,30. African American patients with LN tend to have a worse prognosis compared with white patients17,31,32.
It should be emphasized, however, that the patients treated in our study mirror those of the patient population currently treated in our lupus clinic. Our survival rate (95% at 10 yrs) is well in line with that seen in a large series of 1000 European patients with lupus who were followed in a prospective observational study (88% survival at 10 yrs in the nephritis subgroup)33. Currently, milder cases of proliferative LN, for which less aggressive treatment is certainly justified, are frequently diagnosed because of prompt assessment of kidney involvement, particularly in patients with lupus in whom proteinuria or active urinary sediment without proteinuria is detected and investigated very early during regular followup visits.
Recently, an open study compared 2 different GC doses for induction treatment in LN34. Patients with active proliferative LN received mycophenolate sodium and were randomized to standard-dose or reduced-dose GC. The reduced initial GC dose was half that of the standard-dose group (i.e., prednisone 25 mg/day or 50 mg/day). In the study, 64.2% of 81 patients were white and the mean time since biopsy was 2.2 ± 3.1 months. Remarkably, there was no significant difference concerning response rates between the 2 study groups. The mean cumulative dose of prednisone equivalent to Week 24 was 7.1 ± 1.2 g in the standard-dose group and 4.6 ± 1.0 g in the reduced-dose group. Interestingly, in our study, the mean cumulative dose of prednisone equivalent at the same timepoint was 3.23 ± 1.37 g in our high-dose group.
We observed low rates of major infections (10%). Within the NIH study, severe infections like herpes zoster occurred in 21% of the combination therapy group8. Within the Euro-Lupus Nephritis trial, infections requiring inpatient antimicrobial therapy were noted in 16.6%9. During longterm followup, none of our patients developed avascular necrosis, which, for example, was common in the NIH study and was most prevalent in the groups that received methylprednisolone (18% and 22%, respectively, vs 11% IV CYC alone)8.
Our study had an open-label design, which risks the introduction of bias. However, this may have been diminished because (1) all patients received the same CYC dosing regimen; (2) the prednisone dose was given irrespective of renal function and was guided by extrarenal manifestations; and (3) allocation to the high- or low-dose prednisone group was undertaken post hoc. Nevertheless, the results cannot be uncritically applied to all patients with lupus, in particular to patients with severe extrarenal disease or patients treated with either the Euro-Lupus cyclophosphamide regimen or with MMF.
On the other hand, our approach with prednisone dosing according to extrarenal manifestations takes into account that individual treatment decisions frequently have to be made in clinical practice. Thus, although caution should be exercised in extrapolating our results to other LN populations, our findings suggest that GC dosing could be reduced in the presence of concomitant use of immunosuppressive treatments like IV CYC without loss of efficacy for the management of LN. Our preliminary findings therefore clearly warrant a controlled study comparing different GC dosing regimens in patients with LN.
Acknowledgment
The authors thank Martina Kümmel, Rheumazentrum Rhein-Ruhr, for revising the manuscript and Dalina Verbica for data entry.
- Accepted for publication July 11, 2012.








{kind=link}
{kind=link}