Article Text

Statistics from Altmetric.com
Membranous lupus nephritis (MLN) is characterised by proteinuria, a risk of the development of nephrotic syndrome and progressive deterioration in renal function. Despite the usage of various immunosuppressive agents, no solid, evidence-based recommendations for the treatment of MLN have been established and new therapeutic strategies are needed in therapy-resistant cases.1
During the past few years, rituximab has evolved as a promising new agent in severe lupus nephritis.2,–,4 The aim of this study was to evaluate the clinical and histopathological response to treatment with rituximab plus cyclophosphamide in patients with severe and therapy-resistant MLN.
Six female patients with MLN confirmed at a recent renal biopsy were included. The patients were selected for having proteinuria of 2 g/24 h or greater and recent/previous failure of conventional immunosuppressive agents. All patients were treated with ACE and/or, angiotensin II receptor blockers. In all cases, at least four of the American College of Rheumatology criteria for systemic lupus erythematosus were fulfilled.5 The patients were treated during the time period of 2002–6 (table 1).
Main clinical characteristics, treatment, laboratory parameters and histopathological evaluation before onset of treatment with rituximab plus cyclophosphamide, at 6 and 24 months follow-up and at repeat biopsy.
The protocol has previously been reported in detail.3 Briefly, rituximab 375 mg/m2 was given once a week for 4 weeks combined with two doses of cyclophosphamide 0.5 g. Glucocorticoids were increased to 0.5 mg/kg during the treatment weeks and quickly tapered thereafter. CD19 B cells in peripheral blood were analysed by flow cytometry (limit for detection <0.01×109/l).
Renal evaluation at baseline and up to 2 years included urine analysis (dip slide procedure), urine sediment and investigation of 24 h protein excretion. Repeated renal biopsies were performed after 6 months. All biopsies were graded according to the WHO classification6 and evaluated for activity and chronicity indices.7 Renal disease activity and response to therapy were assessed by the British Isles lupus assessment group (BILAG) index.8 The amount and resorption of electron dense deposits (EDD) in the glomerular basal membrane was determined by electron microscopy and evaluated by using an arbitrary scale (see table 1). All biopsies were evaluated in a blinded manner.
For comparison of variables at baseline and follow-up, Student's t test was used. A p value of less than 0.05 was considered significant.
At baseline the mean prednisolone dose was 15 mg/day (2.5–40) and 10.5 mg/day (7.5–15) (p=0.34) after 6 months. The mean serum creatinine before treatment was 138 μmol/l (range 50–351). A decrease was noted in all but one patient (no 3) at 6 months of follow-up (mean 102, range 41–214) (p=ns). Serum albumin increased from a mean of 26 g/l (17–36) to 35 (33–37) (p=0.024). Twenty-four hour albuminuria decreased from a mean of 5.0 g/day (2.4–7.1) to 1.2 (0.0–4.0) (p=0.023).
In five patients evaluated, all had complete peripheral blood B-cell depletion as defined, after the fourth rituximab infusion. At rebiopsy a reduction in subepithelial EDD (p=0.05) and a significant increase in resorption of basal membrane EDD were observed (p=0.018).
The histological classification including activity and chronicity indices, BILAG data, subepithelial deposits and resorption phenomena and B-cell depletion time during follow-up are shown in table 1.
In this study we demonstrate an improvement in clinical and histopathological outcomes in MLN after treatment with rituximab, notably all patients previously resistant to conventional immunosuppressive therapy. Proteinuria was significantly reduced and serum albumin levels increased at 6 months. All patients improved clinically with long-standing effect and further improvement at 2 years follow-up. In addition, a reduction in subepithelial EDD with increased resorption phenomenon was observed in the basal membrane at repeated renal biopsy (figure 1). The clear clinical improvements paralleled the resorption of EDD in the subepithelial layer. These findings support the possibility that the histopathological changes act as a prerequisite for long-lasting clinical improvements. Although the patients were resistant to conventional therapy before treatment, concomitant therapy with cyclophosphamide and glucocorticoids may have augmented the therapeutic effects. Despite the lack of efficacy of rituximab treatment in lupus nephritis in the LUNAR trial,9 our data provide evidence that rituximab may serve as a therapeutic option in severe therapy-resistant MLN.
{kind=link}
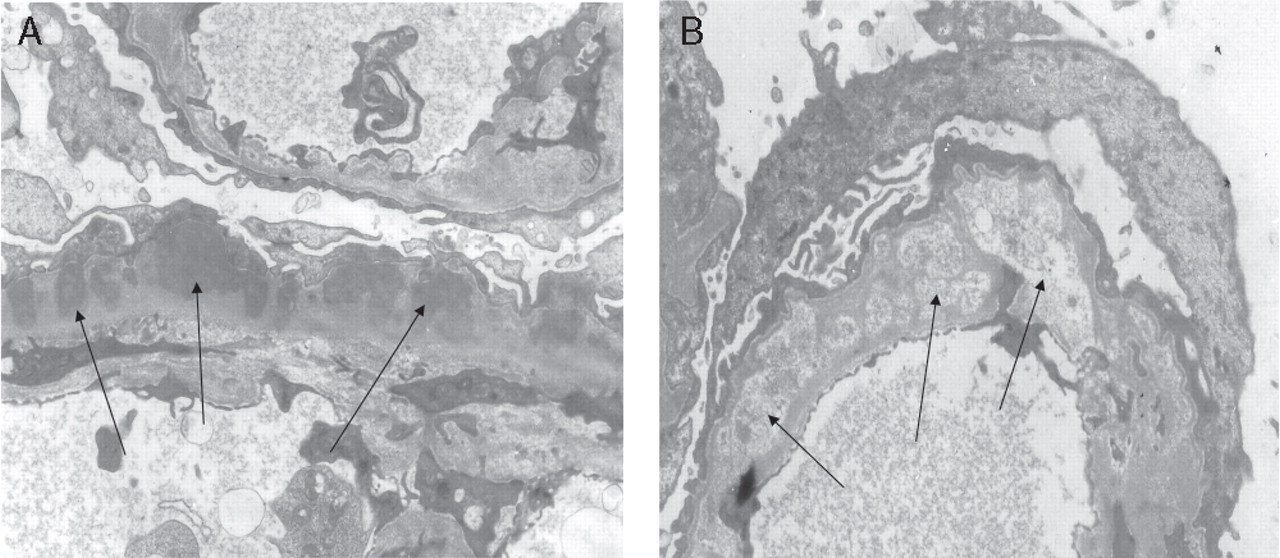
Electron microscopic pictures from one patient (no 1) at baseline (A) and 7 months after rituximab (B). 1(A) demonstrates subepithelial and intramembraneous electron dense deposits in the basal membrane. 1(B) shows resorption phenomenon in the basal membrane depositions.
Footnotes
-
Competing interests TJ and IG have received honoraria (less than US$10 000 each author) from Roche.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Regionala etikprövningskommittén, Stockholm and the Swedish Medical Product Agency.
-
Provenance and peer review Not commissioned; externally peer reviewed.