Article Text

Abstract
Objective Systemic lupus erythematosus (SLE) disproportionately affects women and often develops during their reproductive years. Research suggests that some women who receive cyclophosphamide as treatment for SLE experience earlier decline in menstrual function, but reproductive health among women with SLE who have not taken this drug is less well understood. This study aims to better understand the relation between SLE and reproduction by assessing early secondary amenorrhoea and pregnancy in women treated with and without cyclophosphamide from a population-based cohort with large numbers of African-Americans.
Methods Female patients with SLE, ages 20–40 at time of diagnosis, who were 40 years or older at the time of the survey were included in this analysis (N=147). Participants in the Georgians Organized Against Lupus (GOAL) study were asked about their reproductive histories including early secondary amenorrhoea, defined as loss of menstruation before age 40.
Results Women who were cyclophosphamide naïve had an increased prevalence of early secondary amenorrhoea compared with population estimates, 13–17% compared with 1–5%. Factors associated with early secondary amenorrhoea in women not treated with cyclophosphamide were marital status and receipt of a kidney transplant. Treatment with cyclophosphamide doubled the prevalence after adjustment for patient characteristics. Over 88% of women reported being pregnant at least once, and about 83% of these had a child, but the majority of pregnancies occurred before diagnosis.
Conclusions SLE diagnosed in early adulthood may affect women's reproductive health even if they are not treated with cyclophosphamide. Better understanding of other factors related to reproductive health in this population will improve clinicians' and patients' abilities to make treatment and family planning decisions.
- Systemic Lupus Erythematosus
- Outcomes research
- Cyclophosphamide
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Systemic lupus erythematosus (SLE) disproportionately affects women of childbearing age, making reproductive health an important issue for this patient population. There are several physical and psychological factors that may play a significant role in the ability of women with SLE to achieve their desired family size. One such physical factor is primary ovarian insufficiency (POI), typically defined as cessation of menstruation before the age of 40 with elevated levels of follicle-stimulating hormone. POI can cause infertility in patients with lupus and the hypoestrogenism places these patients at increased risk of osteoporosis and cardiovascular disease, both of which are already a challenge for patients with lupus on long-term corticosteroids.1–3
Much of the literature thus far on reproductive health in women with SLE has focused on the effects of treatment with cyclophosphamide.4–6 This alkylating agent has been reported to reduce ovarian reserve in women with lupus and cancer survivors.7–10 These effects have been observed to increase with age at treatment and cumulative dose in women with lupus.9–13 Studies have observed sustained secondary amenorrhoea occurring in 11–59% of women treated with this drug. Some variation in these results may be due to differences in whether gonadotropin levels were measured to confirm that sustained amenorrhoea was due to ovarian insufficiency.9 ,12 However, in these patients it is difficult to differentiate the effects of cyclophosphamide from the effects of disease activity and other concomitant medications.
Recent research suggests that SLE itself may impair fertility even in those not treated with cyclophosphamide. One study found lower anti-Müllerian hormone (AMH) levels, a marker of ovarian reserve, in women with SLE who had not taken cyclophosphamide compared with healthy women.14 Another small study found lower AMH in women recently diagnosed with SLE who had not yet received treatment compared with age-matched controls. Autoimmune oophoritis may provide a possible explanation for these findings.15 Elevated anticorpus luteum antibody levels have been associated with ovarian dysfunction in patients with lupus.16 Additionally, patients with lupus often experience comorbid conditions, such as end-stage renal disease and autoimmune hypothyroidism, and are often on long-term medications, such as non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids that may contribute to reduced fertility by impairing ovulation.17–19 However, these relationships are not well understood.
The goal of this study is to better understand the reproductive health of women from a well-established population-based cohort diagnosed with lupus as a young adult who were not treated with cyclophosphamide compared with those who receive this drug. It also assesses factors that may be related to impaired fertility in the cyclophosphamide-naïve group. The primary aim of this study is to estimate the prevalence of developing secondary amenorrhoea before the age of 40. Second, this study assesses whether there is an association between experiencing amenorrhoea and becoming pregnant in this patient population among those treated with and without cyclophosphamide.
Methods
Data for this study were collected using the Georgians Organized Against Lupus (GOAL) cohort. Recruitment and data collection methods, as well as the socio-demographic characteristics of patients with SLE, have been described previously.20 Briefly, the primary source of SLE enrolees is the Georgia Lupus Registry (GLR), a population-based registry designed to more accurately estimate the incidence and prevalence of SLE in Atlanta.21 Implemented through a partnership between the Georgia Department of Public Health and Emory University, Emory investigators were able to identify potential patients with SLE and validate their diagnosis without patient consent (under the Health Insurance Portability and Accountability Act Privacy Rule, 45 Code of Federal Regulations, parts 160 and 164), thereby creating the foundation for this population-based cohort.
All those with validated SLE in the GLR were invited to join GOAL, of which >70% accepted. The remaining GOAL participants were recruited from lupus clinics at Grady Memorial (a large safety-net hospital in Atlanta) and Emory University Hospitals and from community rheumatologists in metropolitan Atlanta so that a diversity of patients with SLE were maintained. GOAL participants continue to reflect the socioeconomic characteristics of the GLR, which was an urban population of whom about 80% were African-American and over half of the participants were either on Medicaid/Medicare or were uninsured. Between September 2013 and July 2014, 655 patients with SLE completed the research survey, which included questions on pregnancy and fertility. Male patients and women diagnosed outside of their reproductive years, 20–40 years of age, were excluded from this analysis. Women <20 years old at diagnosis were excluded because SLE and its treatments may have an impact on primary amenorrhoea and reproductive development in these women leading to different reproductive outcomes than women diagnosed as young adults who have already experienced menarche.
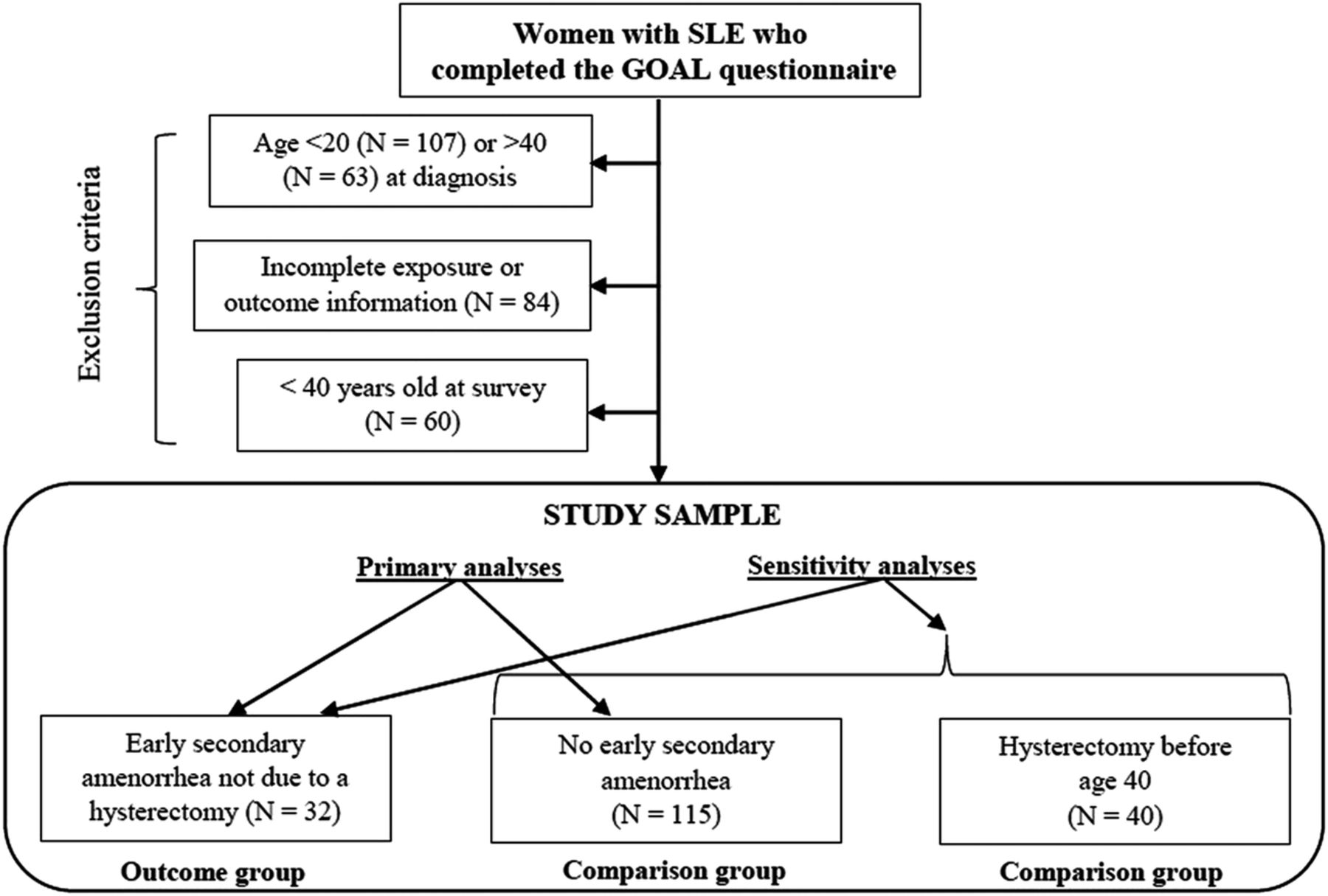
The main outcome of interest, secondary amenorrhoea, was measured by self-report of whether the woman's menstrual periods stopped before the age of 40. In order to investigate secondary amenorrhoea related to hypogonadism, women were only considered to have the outcome of interest if they indicated their period stopped without a hysterectomy. This group was compared with women whose periods had not stopped and women who were currently pregnant. Women who had a hysterectomy were at risk for early secondary amenorrhoea until the time of their hysterectomy, but we do not have this timing information. Therefore, these women were excluded from the primary analyses, but to address this time at risk we conducted sensitivity analyses in which women who had a hysterectomy were included with those women who did not experience secondary amenorrhoea before the age of 40. Women below the age of 40 at the time of the survey were also asked if they had stopped menstruating. However, we excluded these women who were not yet 40 years old because they might still experience early secondary amenorrhoea before reaching this age (figure 1).

{kind=link}
Flow chart depicting the exclusion criteria for this study and which women were included in the primary and sensitivity analyses. GOAL, Georgians Organized Against Lupus; SLE, systemic lupus erythematosus.
Additional outcomes of interest included whether the woman was ever pregnant and whether she had a child and whether these events occurred prior to and after their lupus diagnosis. Cyclophosphamide use was characterised by ever or never use before the age of 40. Other demographic and disease-related characteristics were also obtained from the questionnaire. The self-administered version of disease damage, the Brief Index of Lupus Damage (BILD), was calculated for each woman as an indicator of disease severity. This score typically includes whether a woman has had a hysterectomy before the age of 40, but because this is related to the outcome of interest, in this analysis we recalculated the score without this factor.22
Bivariate analyses were conducted to compare the demographic and disease characteristics between women who were treated with cyclophosphamide and those who were not. The prevalence of early secondary amenorrhoea and pregnancy was evaluated separately by cyclophosphamide treatment status. p Values were calculated using χ2 and Fisher's exact test. Separate multivariable regression models were used to estimate the association between cyclophosphamide and the prevalence of three outcomes: early secondary amenorrhoea, ever being pregnant and having at least one child, controlling for the demographic and disease characteristics. Two additional models were constructed to assess the association between early secondary amenorrhoea and the outcomes ever being pregnant and having at least one child. These models were adjusted for cyclophosphamide use in addition to demographic and disease characteristics. To estimate adjusted prevalence ratios, we first attempted to use the log-binomial model. However, when this model failed to converge we used Poisson regression with a robust variance estimator as has been recommended. The robust variance estimator is necessary because without it Poisson regression applied to a binomial model will overestimate the error.23 The covariates in each model were chosen based on established relations in the literature. All analyses were conducted in SAS V.9.4. The Emory University Institutional Review Board approved this study.
Results
There were 331 women diagnosed with SLE between 20 and 40 years old who completed the GOAL questionnaire by July 2014. Of these, 247 (74.6%) responded to questions regarding cyclophosphamide use and early secondary amenorrhoea. Sixty (24.3%) were younger than 40 years old at the time of the survey. In the remaining 187 women, 22.5% (N=42) had previously been treated with cyclophosphamide. Among those treated, 31.0% (N=13) reported early secondary amenorrhoea without a hysterectomy and 21.4% (N=9) had a hysterectomy. In women who were cyclophosphamide naïve, 13.1% (N=19) experienced early secondary amenorrhoea without a hysterectomy and 21.4% (N=31) had a hysterectomy before the age of 40 (see online supplementary table S1). Therefore, after excluding the 40 women who had a hysterectomy, the final sample size was 147.
supplementary tables
In the final study population, 22.4% (N=33) of women had previously been treated with cyclophosphamide. These women were more likely to have achieved higher education compared with women who did not receive this treatment. The prevalence of secondary amenorrhoea was 39% in women treated with cyclophosphamide and 17% in cyclophosphamide-naïve women (table 1).
Demographic characteristics of women with lupus by treatment status with cyclophosphamide
Most women reported being pregnant at least once (N=114, 88.4%) and 83% of these women had at least one child. The majority of pregnancies occurred prior to the lupus diagnosis with 58% (N=66) of women who had a pregnancy only being pregnant before diagnosis. Only 16 women who had not been pregnant before their diagnosis reported a pregnancy after developing lupus. Women treated with cyclophosphamide were slightly less likely to have ever been pregnant compared with those not treated with this drug; this difference was not statistically significant (66.7% vs 80.7%). Among women who were cyclophosphamide naïve, there were no differences in the number of pregnancies or children between those with early secondary amenorrhoea and those without it. However, among women who took cyclophosphamide, women who also experienced early secondary amenorrhoea were less likely to have ever been pregnant (64% vs 94%) and less likely to have had at least one child (55% vs 86%). This difference was driven by differences in the number of pregnancies conceived before the lupus diagnosis. No differences were observed between these groups in reproductive health after diagnosis, but, few women became pregnant after their lupus diagnosis (table 2).
Reproductive health by cyclophosphamide status and self-report of early secondary amenorrhoea
Women who had been treated with cyclophosphamide had over twice the prevalence of early secondary amenorrhoea compared with those who were cyclophosphamide naïve (prevalence ratio (PR)=2.4, 95% CI 1.3 to 4.4). The association did not meaningfully change after adjustment for demographic and disease-related characteristics (adjusted PR=2.3, 95% CI 1.1 to 4.7). Women treated with cyclophosphamide had a similar prevalence of ever being pregnant (adjusted PR=0.8, 95% CI 0.7 to 1.0) and having a child (adjusted PR=0.8, 95% CI 0.6 to 1.0) compared with cyclophosphamide-naïve women. Early secondary amenorrhoea was also not related to ever being pregnant or having children after adjustment for important covariates (adjusted PR=0.9, 95% CI 0.8 to 1.1 and adjusted PR=0.8, 95% CI 0.6 to 1.1 respectively) (table 3).
Comparison of the prevalence of early secondary amenorrhoea, ever being pregnant and ever having a child by cyclophosphamide status and whether the women experienced early menopause
An exploratory analysis was performed only among women who were cyclophosphamide naïve to investigate other factors that may be associated with early secondary amenorrhoea in this group. These results showed that women who experienced secondary amenorrhoea before age 40 were more likely to have never married (58% vs 17%) and to have received a kidney transplant (11% vs 0%). However, only two women in the study received a kidney transplant. Secondary amenorrhoea was also more common in this population among women who were treated with methotrexate (table 4). There was a slight increase in use of hydroxychloroquine, mycophenolate mofetil and steroids among women who experienced early secondary amenorrhoea, but the numbers were small and not meaningfully different. There was no association between steroid type, duration of use and maximum dose taken in the previous year but this analysis may also have been underpowered (results not shown). In sensitivity analyses including women who had a hysterectomy, most of the results did not meaningfully change with the exception that the prevalence of secondary amenorrhoea was slightly reduced (see online supplementary tables).
Association between demographic and clinical characteristics and early secondary amenorrhoea among women who were not treated with cyclophosphamide
Discussion
This study found that cyclophosphamide was associated with a more than two times greater prevalence of secondary amenorrhoea before age 40 among women diagnosed with SLE in early adulthood compared with women who were cyclophosphamide naïve. The prevalence of those reporting loss of their period before the age of 40 unrelated to a hysterectomy was 31–39% in women who took cyclophosphamide and 13–17% in those who did not, depending on whether women who had a hysterectomy were included in the denominator. Even the lower estimates are much larger than the prevalence in the general population. Estimates depend on the definition used, but studies that considered premature menopause, loss of a menstrual cycle for at least six months and premature ovarian insufficiency have found these outcomes in 1–5% of the general population.24 ,25 This finding underscores the potential fertility effects of lupus among patients not treated with cyclophosphamide.
Although the results suggest that women with lupus have an increased risk of POI, >88% of the study population had experienced a pregnancy and the majority of these women had a child. One likely reason for these results is that almost all pregnancies occurred before the women received their diagnoses. Women may not become pregnant after diagnosis because of reduced fertility or already having achieved their desired family size by the time of the diagnosis. Alternatively, this may imply that the psychological and other physical effects of the disease, such as fear of disease exacerbation, use of medications contraindicated for pregnancies, fatigue and other disease symptoms, may make these women hesitant to pursue expanding their families even if they remain fertile. However, pregnancy outcomes among women with lupus have become more favourable and attitudes among providers have shifted to not necessarily view lupus as a contraindication for pregnancy under the right conditions.26 Therefore, another reason for this decrease in pregnancies after diagnosis may be that having lupus places women in a more difficult socioeconomic position so that they avoid pregnancy and further economic strain.20 The bivariate results showed that women treated with cyclophosphamide and who reported early secondary amenorrhoea were much less likely to ever have a pregnancy or a child compared with the other three groups. Most of this difference was due to women in the other three groups being more likely to have a pregnancy or child before their diagnosis. In subsequent analyses (results not shown), we did not find differences in demographic characteristics that could explain this effect. Therefore, these women may have other underlying fertility problems, which may or may not been related to SLE.
The results of this study for those treated with cyclophosphamide are similar to those published in previous studies that have found sustained secondary amenorrhoea in 11–59% of these patients.9 ,12 In one study of patients with lupus, under the age of 45, 30% of women treated with cyclophosphamide developed subsequent amenorrhoea and ovarian insufficiency was confirmed in 26% of women by measuring hormone levels.12 Similarly, another study found that 36% of patients experienced amenorrhoea after treatment with cyclophosphamide and permanent amenorrhoea after cessation of treatment occurred in 27%.27 Estimates of menstrual irregularities in patients with lupus who were cyclophosphamide naïve are limited and varied in the previous literature. One study found that no woman in this group experienced a cessation of menstruation lasting for at least 12 months compared with approximately 30% of women exposed to cyclophosphamide, but the average age of women in this study was 32 years old.4 Alternatively, another study found that about 53% of women experienced menstrual irregularities before the age of 40.28
The reasons for this seemingly early decrease in menstrual function beyond treatment with cyclophosphamide are unclear. We did not observe an association with disease severity as determined by disease damage, which is consistent with some previous studies18 ,28 although others have detected an association.29 ,30 End-stage renal disease has been associated with amenorrhoea in some patients with lupus.19 To explore this association, we assessed our outcomes according to whether the woman received a kidney transplant or was on dialysis for >6 months. We saw an association between secondary amenorrhoea and the first characteristic but not the second. However, the number of women who had these treatments for renal disease was small, and therefore our estimates may not be stable.
Among women who were cyclophosphamide naïve, we also observed a trend that those previously treated with methotrexate had a higher prevalence of amenorrhoea. Methotrexate is considered teratogenic and is not recommended for use during pregnancy but is generally not considered gonadotoxic.31 ,32 However, recent studies of patients with childhood-onset lupus and patients treated for an ectopic pregnancy suggested an association with a reduction in ovarian function.33 ,34 In contrast, a study of short-term use of methotrexate in patients newly diagnosed with rheumatoid arthritis did not find a decrease in AMH levels.35 To assess whether the trend seen for methotrexate may simply be an indicator of other disease characteristics, we also compared the prevalence of early secondary amenorrhoea between those treated with mycophenolate mofetil and hydroxychloroquine. These drugs are frequently used to treat symptoms of SLE, but we would not expect either to be associated with early amenorrhoea. As expected, similar percentages of women who had and had not experienced secondary amenorrhoea reported use of these drugs. Corticosteroid use was not associated with amenorrhoea in our study, even when considered by years of use and recent maximum dose, but most women in the study had taken corticosteroids at some point in their treatment. Although high doses of corticosteroids have been associated with menstrual irregularities in other disease groups, our finding is consistent with at least one other study in patients with lupus that has failed to detect an association.28 We also found an association between never being married and a higher prevalence of early secondary amenorrhoea. Such an association has also been observed with POI in the general population.24
This population-based study benefits from a number of strengths including a larger sample size compared with many previous studies on reproductive health in patients with lupus and avoids the referral bias that may be seen in cohorts from academic centres. Additionally, our study population consists of a higher percentage of African-American women in comparison to other lupus populations that have been researched, which is reflective of the demographic of patients in this region. This particular group tends to have more severe disease, which can in turn further impact pregnancy outcomes,36 ,37 and African-American women with lupus are more affected by other reproductive conditions, such as fibroids, than white women.38 ,39
Another strength of this study is that we examined secondary amenorrhoea in addition to pregnancy and number of children. This is important because early secondary amenorrhoea is significant for all women, not just those who would like to have more children. Previous studies have primarily focused on pregnancy outcomes to assess reproductive health in women with lupus, but becoming pregnant depends on more than fertility, including a woman's desire for children, whether she has a committed partner and psychological factors. Additionally, women who are diagnosed at older ages may have all the children they desire before symptoms arise. This distinction is highlighted by our findings that early secondary amenorrhoea was not associated with ever being pregnant or having a child in our study population.
Despite our findings, this study has several limitations. First, our primary outcome of interest, early secondary amenorrhoea, was measured by self-report from a question asking the woman whether her menstrual periods stopped before the age of 40. This does not meet the standard definitions of premature menopause or POI, and it is difficult to know how women interpreted this question. Although secondary amenorrhoea for many women in the study is likely due to POI, other causes may include thyroid disease, hyperprolactinemia related to kidney disease and functional hypothalamic amenorrhoea. Ideally serum markers of POI would have been measured to confirm this as the reason for secondary amenorrhoea. Previous studies with this information have confirmed POI as the cause in most women who reported secondary amenorrhoea.
Because the information for this study was obtained from a cross-sectional design, we assessed the prevalence of secondary amenorrhoea instead of the incidence. Without timing information, this also means that we were unable to determine whether secondary amenorrhoea occurred after SLE diagnosis or cyclophosphamide use, and therefore we are unable to establish temporality. Women may also not accurately recall the exact age when their period stopped, and if women with lupus are more aware of their health than women in the general population they may be more likely to remember if they experience secondary amenorrhoea before the age of 40 that would affect our comparison with estimates from the general population.
Although we were able to separate those who experienced menopause due to a hysterectomy, we do not know if the women's menstrual cycles were influenced by other factors such as hormonal contraceptive use, which may mask the signs of menopause. It is possible that a lack of oral contraceptive use could partially explain the increase in early secondary amenorrhoea that we observed, but we were not able to assess this. There is evidence that oral contraceptives delay the age at menopause,40 but in a large community-based cohort study, the adjusted average age of menopause was different by less than a year between groups who had taken oral contraceptives and those who had not. Therefore, it is unlikely that a lack of ovarian protection from these medications could fully explain the large prevalence we observed.
Self-report of prior medication use may have also led to misclassification. Among the women who reported treatment with cyclophosphamide, some did not have timing information and therefore may have received treatment after the age of 40 but would be considered exposed in this study. Any bias resulting from this misclassification would likely be towards the null because these women would likely be more similar to the unexposed group so their misclassification as exposed would dampen the estimated prevalence of early secondary amenorrhoea. Additionally, we did not obtain information on the cumulative dose. No data were obtained on NSAIDs, which may be linked to temporary amenorrhoea in patients.41 Confounding by indication cannot be excluded as an explanation for our findings related to medication use. We tried to address this issue by adjusting for disease damage and by considering medications that we did not expect to be associated with reproductive health. However, because physicians are aware of the potential side effects of cyclophosphamide, women prescribed this drug are likely those for which other medications have not been effective. Another complication related to medication use is the concurrent or previous use of multiple forms of treatment. We do not directly address this in the article because we focused on ever use of the medications, but almost all women in the cohort had taken a steroid and at least one other type of medication with the combination of a steroid and hydroxychloroquine being the most common. Very few women had taken all of the medications of interest, and no single pattern of medication use dominated in this cohort.
Although our sample size was larger than other studies researching similar topics, the number of women who experienced early secondary amenorrhoea was small after stratification. This may have made some of our estimates unstable, prevented us from detecting certain associations such as those with cyclophosphamide and reproductive health after the lupus diagnosis or led to an overestimation of associations. Furthermore, our study population was too small to evaluate interaction in the multivariate analyses for covariates such as race. The original study sample was much larger than the number available for our analyses, but many women did not answer questions that were of primary interest. This could induce bias if women who were more concerned about their fertility and had more severe disease were more likely to answer these questions. The study sample also lacked a healthy comparison group. Therefore, we can only compare our results with population estimates without adjustment for demographic characteristics.
Finally, our results may not be generalisable to women diagnosed with SLE outside of early adulthood because we restricted our population to those diagnosed between 20 and 40 years old. Additionally, women had to survive to the age of 40 to be included in our study, which could introduce bias if survival is related to early secondary amenorrhoea. It may be that women who do not survive to the age of 40 would be those with more severe disease and/or those with less access to care. Among the women not treated with cyclophosphamide in our study, we did not find an association between early secondary amenorrhoea and disease damage as measured by the BILD score or between early secondary amenorrhoea and any of the socioeconomic characteristics assessed, but it is still a possibility that a lack of these associations resulted from the depletion of the most susceptible women before the start of our study. Women with early secondary amenorrhoea were more likely to have had a kidney transplant, but this affected only a small number of women.
More research is needed to better understand the reproductive health of women with SLE, including those who are not treated with cyclophosphamide. Future studies should aim to recruit larger and more diverse study populations so that differences between groups can be assessed. Specifically, African-American women with lupus are generally understudied and research should attempt to better understand the effects on fertility in this population. Healthy control groups and women recently diagnosed with lupus should also be included in studies to compare with those who have had the disease for a longer period of time. Data on the timing of reproductive health and medication use would improve the analysis and interpretation of results. Further, measuring AMH over time in patients with SLE could elucidate how ovarian reserve declines over the course of disease. Outcomes such as AMH are also useful because they are not influenced by psychological complications of lupus unlike pregnancy. Nevertheless, these psychological issues are also important and factors such as desire for children and comfort level with attempting pregnancy should be considered. In addition to the effect of cyclophosphamide on fertility, studies should continue to explore the effects of other exposures such as NSAIDs, steroids, hypothyroidism and autoimmune antibodies on fertility in this population. Specifically for medications, more data are needed to determine reasonably safe doses for women who desire to become pregnant in the future. Better understanding these factors and how they are related will improve clinicians' and patients' abilities to make treatment and family planning decisions.
Acknowledgments
The authors thank the patients who participated in the study.
References
Footnotes
Contributors All contributors meet the criteria for authorship and approved the submitted version of the manuscript.
Funding The Georgia Lupus Registry was supported in part by the CDC and by cooperative agreement CDC-RFA-DP08-806 and earlier by cooperative agreement PA03022 from the CDC. The Georgians Organized Against Lupus Cohort was supported in part by an investigator-initiated grant from GlaxoSmithKline. SSL is supported in part by the NIH (R01AR065493) and the CDC (U01DP005119). JHK was supported during this research by the Eunice Kennedy Shriver National Institute of Child Health and Human Development Reproductive, Perinatal, & Pediatric Training Grant (T32HD052460).
Competing interests None declared.
Ethics approval The Emory University institutional review board approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.