Article Text

Abstract
Objectives To assess the prevalence and severity of ultrasonographic abnormalities of the hand and wrist of asymptomatic patients with systemic lupus erythematosus (SLE) and compare these findings with those from patients with SLE with musculoskeletal signs or symptoms and healthy controls.
Methods We conducted a prospective cross-sectional study that evaluated bilaterally, with grey-scale and power Doppler (PD) ultrasound (US), the dorsal hand (2nd to 5th metacarpophalangeal and 2nd to 5th proximal interphalangeal joints) and wrist (radiocarpal, ulnocarpal and intercarpal joints) of 30 asymptomatic patients with SLE, 6 symptomatic patients with SLE and 10 controls. Synovial hypertrophy (SH) and intra-articular PD signal were scored using semiquantitative grading scales (0–3). Individual scores were graded as normal (SH≤1 and PD=0) or abnormal (SH≥2 or PD≥1). Global indexes for SH and PD were also calculated. US findings were correlated with clinical and laboratory data and disease activity indexes.
Results US detected SH (score ≥1) in 77% asymptomatic patients with SLE, mostly graded as minimal (score 1: 63%). 23% of the asymptomatic patients with SLE showed abnormal US PD findings (SH≥2 or PD≥1). SH was present in all symptomatic patients with SLE, mostly graded as moderate (grade 2: 67%), and with associated PD signal (83%). SH (score 1) was identified in 50% of controls, however, none presented abnormal US PD findings. SH index in the asymptomatic SLE group was higher than in the control group (2.0 (0–5) vs 0.5 (0–2), median (range), p=0.01) and lower than in the symptomatic SLE group (7.0 (4–23), median (range), p<0.001). No significant correlation was demonstrated between US PD findings and clinical or laboratory variables and disease activity indexes.
Conclusion A small subgroup of asymptomatic patients with SLE may present subclinical joint inflammation. Global US scores and PD signal may be important in disease evaluation and therapeutic monitoring.
- Systemic Lupus Erythematosus
- Synovitis
- Ultrasonography
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Joint involvement is one of the most common features of systemic lupus erythematosus (SLE), with up to 95% of patients experiencing arthralgia or arthritis during the course of their disease.1 While multiple joints can be affected, nearly 50% of patients report difficulties in daily life performance due to hand symptoms.2 Traditionally, SLE arthritis is considered to be mild, reversible and non-erosive, with only 5–15% of cases progressing to deforming arthropathy, either erosive—as in rhupus syndrome (an overlap of SLE with rheumatoid arthritis (RA))—or non-erosive—as in Jaccoud’s arthropathy.3 ,4 In routine clinical practice, joint involvement is usually assessed with physical examination and radiographical studies. However, this approach has been shown to have a low sensitivity for joint abnormalities when compared with ultrasound (US) evaluation or MRI, suggesting that the burden of joint inflammation may be underestimated in the current clinical practice.5 The value of US with power Doppler (PD) in inflammatory arthritis has been extensively demonstrated in the literature, with similar sensitivity and specificity in the detection of synovitis in comparison with MRI, with the advantage of being more accessible and less expensive.6–8 While US shows the morphology of the synovial membrane, PD identifies increased vascularisation within it, allowing for the detection of active joint inflammation.9 It is known that in RA synovial abnormalities are present before clinically evident arthritis develops, and that early treatment can limit erosive changes and avoid disease progression.10 In this context, US PD has nowadays an established role in the detection of subclinical joint inflammation in RA, namely to predict progression in patients with clinical remission.11 ,12
Although there is evidence that US PD is a valuable technique in the evaluation of musculoskeletal symptoms in SLE, the prevalence of subclinical joint abnormalities in SLE remains to be defined.13 ,14 Furthermore, while it is known that minimal synovial proliferation may be seen in up to 50% of healthy subjects, the distinction between ‘normal’ synovial hypertrophy (SH) and pathological subclinical synovitis in SLE still requires clarification.15–18
The aim of this study was to assess the prevalence and precise grading of US abnormalities of the hand and wrist in asymptomatic patients with SLE, while comparing these findings with a group of patients with SLE with musculoskeletal signs or symptoms and with healthy controls.
Patients and methods
Patients and study design
We conducted a prospective cross-sectional study which included patients fulfilling the 1997 revised American College of Rheumatology (ACR) criteria for SLE,19 under standard of care, and on stable medication in the preceding 4 weeks. Patients were sequentially recruited from the population of the two outpatient autoimmune disease units from Centro Hospitalar de Lisboa Central (Lisbon, Portugal) between January 2014 and July 2015. A subset of these patients has been previously characterised.20 We excluded patients with a known diagnosis of rhupus syndrome (defined as patients with SLE also satisfying the classification criteria for RA)21 or Jaccoud’s arthropathy and mild deforming arthropathy (according to the Jaccoud’s Arthropathy Index),4 ,22 as well as patients with known osteoarthritis, trauma or surgery of the hand or wrist. Healthy controls had no personal or familiar history of autoimmune diseases and denied previous hand or wrist trauma and osteoarthritis. The study was approved by the Hospital Centre Ethics Committee and performed according to the principles of good clinical practice and to the Declaration of Helsinki. Informed consent was obtained from all enrolled patients.
Clinical and laboratory evaluation
Patients with SLE underwent a medical interview from which demographic, clinical data and previous history were recorded, together with a detailed physical examination according to the European League Against Rheumatism (EULAR) recommendations.23 Patients were then classified as asymptomatic (if musculoskeletal symptoms or signs were absent) and symptomatic (if musculoskeletal signs or symptoms were present).
Disease activity was assessed using the SLE Disease Activity Index (SLEDAI-2K),24 and organ damage was assessed using the ACR/Systemic Lupus International Collaborating Clinics (SLICC) score.25 Active disease was defined as a SLEDAI score equal or superior to 3.26 Anti-nuclear antibodies (ANA) were detected by indirect immunofluorescence using HEp-2 epithelial cells as the substrate (American Type Culture Collection CCL 23). The serum dilution was 1/160, and a titre equal to or greater than 1:160 was considered positive. Serum samples were diluted 1/10 for detection of antibodies against double-stranded DNA (anti-dsDNA) on Crithidia luciliae. Positive results were quantified by ELISA for IgG. Laboratory evaluation also included erythrocyte sedimentation rate, C3 and C4 complement levels by nephelometry and ELISA for rheumatoid factor (RF) and anti-citrullinated protein IgG antibodies (anti-CCP).
Grey-scale and PD ultrasonography
Patients and controls underwent bilateral musculoskeletal US examination with PD evaluation of the hand and wrist, performed on the same week as the medical interview. All US scans were performed simultaneously by two radiologists with experience in musculoskeletal radiology, blinded to clinical and laboratory data, using a Logiq E9 machine (General Electric Medical Systems, Milwaukee, USA) with a 6–15 MHz linear array probe operating at 15 MHz. PD evaluation was performed with a PD frequency of 10 MHz, gain 50% and low wall filter.27 For each US evaluation, an adequate amount of warm gel was used, and compression with the probe was avoided, to accurately evaluate synovial vascularisation. US examinations were performed with comparable technical and environmental factors. Using a multiplanar scanning technique according to EULAR guidelines for musculoskeletal US in rheumatology,28 the following joints were scanned bilaterally, on the dorsal side: radiocarpal, ulnocarpal, intercarpal; 2nd–5th metacarpophalangeal (MCP) and 2nd–5th proximal interphalangeal (PIP) joints (total of 22 joints per person). The first MCP and interphalangeal joints were not scanned to avoid the bias of possible coexisting osteoarthritis.
SH was defined as hypoechoic intra-articular tissue that was non-displaceable and poorly compressible and which may or may not exhibit PD signal, according to definitions provided by the Outcome Measures in RA Clinical Trials (OMERACT) Special Interest Group for Musculoskeletal US in Rheumatology.29 Synovial vascularisation was assessed with PD evaluation. Each joint was evaluated individually and classified for SH and intra-articular PD using two semi-quantitative grading methods, the Szkudlarek grading method,30 and the OMERACT–EULAR composite PDUS synovitis score (figure 1).31 The Szkudlarek method grades each parameter individually as follows: SH: 0—no synovial thickening, 1—minimal synovial thickening (filling the angle between the periarticular bones, without bulging over the line linking tops of the bones), 2—synovial thickening bulging over the line linking tops of the periarticular bones but without extension along the bone diaphysis, 3—synovial thickening bulging over the line linking tops of the periarticular bones and with extension to at least one of the bone diaphysis; PD: 0—no flow in the synovium, 1—single vessel signals, 2—confluent vessel signals in less than half of the area of the synovium, 3—vessel signals in more than half of the area of the synovium.30 The OMERACT–EULAR composite PDUS synovitis score is a composite score of synovial hyperplasia and PD signal: 0 (normal joint)—no grey-scale-detected synovial hyperplasia and no PD signal; 1 (minimal synovitis)—grade 1 synovial hyperplasia and ≤ grade 1 PD signal; 2 (moderate synovitis)—grade 2 synovial hyperplasia and ≤ grade 2 PD signal; or grade 1 synovial hyperplasia and grade 2 PD signal; 3 (severe synovitis)—grade 3 synovial hyperplasia and ≤ grade 3 PD signal, or grade 1 or 2 synovial hyperplasia and grade 3 PD signal.31 A reference atlas for grey-scale and PD semi-quantitative scoring of RA joints was also consulted for the purpose of grading abnormalities in the radiocarpal, ulnocarpal or intercarpal joints.32 To compare the groups of patients with SLE and controls, individual scores of SH and PD were dichotomised: SH scores of 0 and 1 and PD score 0 were considered normal; SH scores 2 and 3 and PD scores 1–3 were considered pathological.30 ,33 Decisions of individual joint scores were made by consensus between the two radiologists.
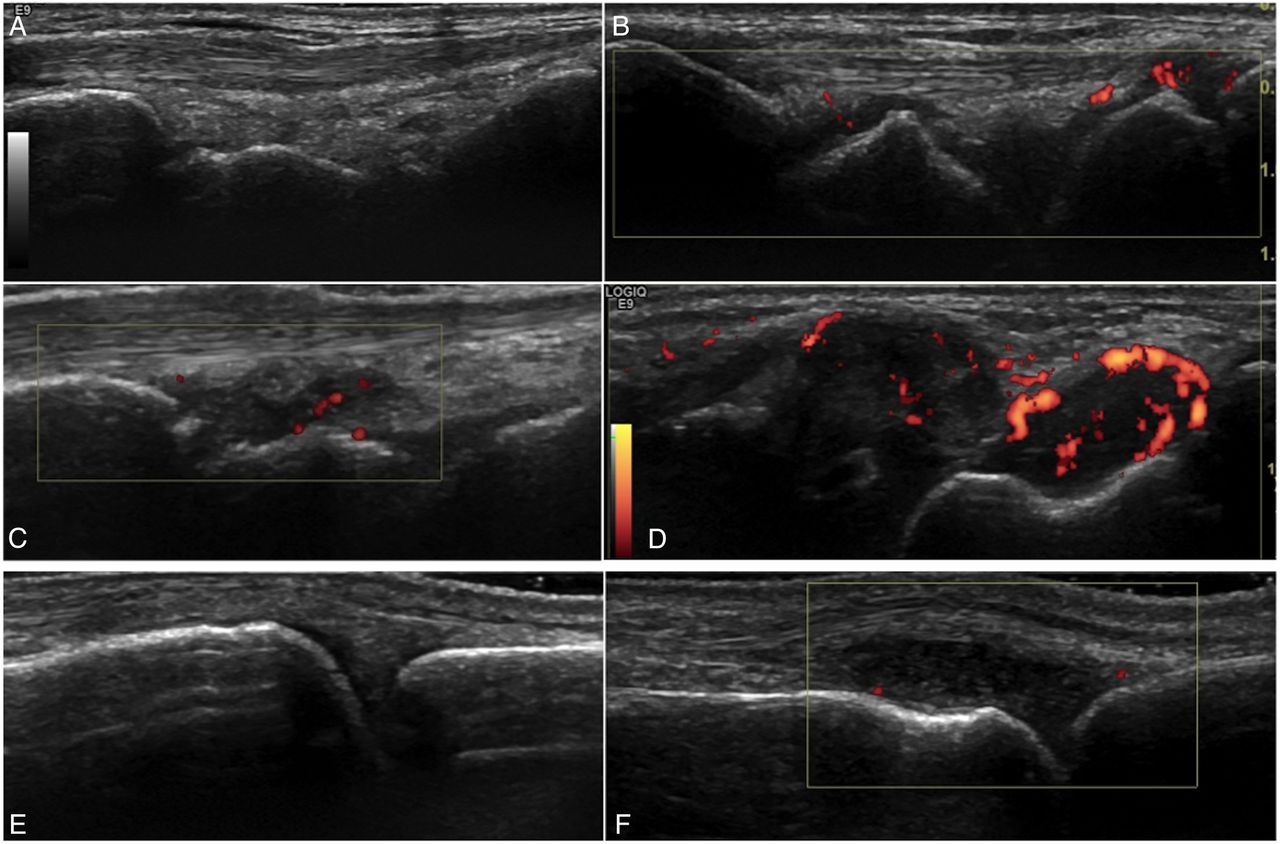
{kind=link}
Representative ultrasound images of patients with SLE. Images (A–D) show dorsal longitudinal scans of the radiocarpal joint with different degrees of synovial hypertrophy and PD, according to the Szkudlarek semi-quantitative grading method: (A) no synovial hypertrophy (grade 0); (B) minimal synovial hypertrophy (grade 1) with minimal PD signal (grade 1); (C) moderate synovial hypertrophy (grade 2) with minimal PD signal (grade 1); (D) severe synovial hypertrophy (grade 3) with moderate PD signal (grade 2). Images (E and F) show dorsal longitudinal scans of the metacarpophalangeal joints: (E) absence of synovial hypertrophy (grade 0); (F) severe synovial hypertrophy (grade 3) with minimal PD signal (grade 1). In these examples, the OMERACT–EULAR composite PDUS synovitis scores were equivalent to the synovial hypertrophy scores from the Szkudlarek method. EULAR, European League against Rheumatism; PD, power Doppler; OMERACT, Outcome Measures in RA Clinical Trials; SLE, systemic lupus erythematosus.
For the purpose of group comparisons, in addition to individual scores, we also calculated two global indexes for SH and PD, corresponding to the sum of individual scores for all joints assessed. SH index and PD index were calculated using the Szkudlarek grading method,14 ,34 and the Global OMERACT–EULAR Synovitis Score (GLOESS) was calculated using the composite PDUS synovitis score.31
Statistical analysis and sample size
Continuous variables were recorded as medians (range or IQR) and comparisons were made using Wilcoxon rank sum test. Dichotomous variables were examined by frequency distribution, recorded as proportions, and comparisons were made using the χ2 test or Fisher’s exact test. Correlations between variables were analysed with Spearman's correlation coefficient or with simple logistic regression, as appropriate. Nominal two-sided p values of<0.05 were considered statistically significant. Analyses were performed using STATA Statistical Software Release 13 (College Station, Texas, USA).
Based on data from Yoon et al (subclinical synovitis detected in 58.3% of asymptomatic patients with SLE and 5.6% of controls),14 for a 0.05 α-value and 90% power, and considering a 3:1 ratio, a sample size of 30 asymptomatic patients with SLE and 10 controls was calculated.
Results
Population characterisation
Thirty-six consecutive patients with SLE (34 females, 2 males) were enrolled in this study, with a median age of 41.5 years (IQR=35–53). Age and gender in the controls (n=10) were similar to those of the patients with SLE (median age: 33.5 years (IQR=29–49), p=0.2; female gender: 9 (90%), p=0.61).
The majority of patients with SLE (n=30, 83.3%) were asymptomatic, while the remaining six presented musculoskeletal signs or symptoms at enrolment. Demographic, clinical, laboratory and therapeutic features were homogenous between the two groups (table 1).
Demographical, clinical, laboratory and therapeutic characteristics of asymptomatic and symptomatic patients with SLE
All patients with SLE were positive for ANA, anti-dsDNA was present in 17 (47.2%), 3 (8.3%) were RF positive and 1 (2.8%) was anti-CCP positive. All patients with SLE have been treated with hydroxychloroquine during the course of their disease. Of these, 19 asymptomatic (63.3%) and 4 symptomatic (66.7%) patients were receiving oral prednisolone at the time of enrolment (median dose 5 mg, range 2.5–25 mg in the asymptomatic group; median dose 5 mg, range 3.75–10 mg in the symptomatic group; p=0.93).
Ultrasonographical findings
US findings at joint level
When considering the total number of joints examined, US detected a significantly higher prevalence of joints with SH (grade ≥1) in the SLE population, when compared with the control group (11.1% (88/792) vs 2.7% (6/220), p<0.001) (table 2).
Number of joints with SH and PD signal in each group
In the asymptomatic SLE group, the prevalence of joints with SH (grade ≥1) was also significantly higher than in the control group (8.2% (54/660) vs 2.7% (6/220), p=0.005) and significantly lower than in the symptomatic patients with SLE (8.2% (54/660) vs 25.7% (34/132), p<0.001).
The prevalence of abnormal SH (score ≥2) and positive PD signal in the asymptomatic SLE population was 0.7% (5/660) and 1.4% (9/660), respectively. None of these findings were identified in the joints of the healthy controls.
US findings at population level
US detected SH (grade ≥1) in 29 of the 36 (80.6%) patients with SLE, and particularly in 23 of the 30 (76.7%) asymptomatic patients with SLE (table 3).
Prevalence of US PD findings and global US PD scores in each group
In the asymptomatic SLE group, most SH was graded as minimal (grade 1: 19 out of 30 patients, 63.3%). Abnormal US PD findings (SH ≥2 or PD signal ≥1) were seen in 7 (23.3%) asymptomatic patients with SLE.
In the symptomatic SLE group, SH was present in all the patients, and mostly graded as moderate (grade 2: 4 out of 6, 66.7%). PD signal was present in 5 out of 6 patients (83.3%).
SH (grade ≥1) was identified in 5 out of 10 healthy controls (50%), however none presented abnormal SH (score ≥2) or a positive PD signal.
The SH index in the asymptomatic SLE group was higher than in the control group (2.0 (0–5) vs 0.5 (0–2), median (range), p=0.01) and lower than in the symptomatic SLE group (2.0 (0–5) vs 7.0 (4–23), median (range), p<0.001). GLOESS was equivalent to the SH index in asymptomatic patients with SLE and in the control group, being slightly higher than the SH index in the symptomatic patients with SLE (7.5 (4–23), median (range)).
PD index was higher in the symptomatic patients with SLE when compared with the asymptomatic patients with SLE (4.0 (0–8) vs 0 (0–3), median (range), p=<0.001) and to the controls (4.0 (0–8) vs 0 (0–0), median (range), p=0.001).
Clinical and laboratory associations with US findings
No correlation was demonstrated on univariate analysis between US PD variables (GLOESS, SH index, PD index, prevalence of abnormal US PD findings) and demographic, clinical and laboratory data (see online supplementary table SI). Disease activity and organ damage scores did not show significant correlation with US PD variables (see online supplementary tables SI and SII). Patients receiving oral prednisolone at the time of the evaluation had higher PD indexes compared with patients who were not taking this medication (see online supplementary table SIII).
supplementary tables
Discussion
The present study provides data on the US PD findings of a population of patients with SLE without musculoskleletal signs or symptoms, in comparison with symptomatic patients with SLE and healthy controls. In our study, US revealed SH of the hand or wrist in 8% of the examined joints and in 77% of patients with SLE who denied arthralgia and did not present abnormalities on physical examination. The majority of these patients presented minimal SH (score 1) without associated PD, which could be considered normal, according to previous literature.13 ,30 ,33 However, abnormal US findings (SH≥2 or PD signal) were seen in 23% of patients. We believe that these findings indicate subclinical joint inflammation. Accordingly, while minimal SH was detected in 50% of the controls, none presented abnormal SH (score≥2) or positive PD signal.
While a number of studies have recently described US findings in the SLE population, only some of these included patients who did not complain of musculoskeletal symptoms at the time of the US evaluation,5 ,35–39 and, to our knowledge, only one focused on asymptomatic patients.14 In these studies, the prevalence of US abnormalities in asymptomatic patients with SLE varied from 3% to 58%.5 ,13 ,36–38 This inconsistency is thought to be related to US reporting methodologies, mostly due to the lack of consensus about the definition of a positive US examination. Most studies defined synovitis as SH grade 1 or higher; however, grade 1 synovitis without PD can be found in healthy subjects and in patients with osteoarthritis.13 ,33 In addition, while the majority of studies described a semi-quantitative grading score in the methodology, results were most often presented as binary (synovitis/no synovitis), and the prevalence of each SH score was usually not addressed.13 Furthermore, to our knowledge, only a limited number of studies described global US scores in patients with SLE.14 ,39
Our study contributes to a better understanding of subclinical joint disease in patients with SLE, as it provides a detailed description of the US PD findings both at joint level and at population level and characterises the groups of patients and controls by using two sets of global US scores. SH index and GLOESS scores were similar in the asymptomatic SLE group; however, in the symptomatic group GLOESS values were slightly higher. We believe GLOESS may be advantageous, as it includes information about SH and PD signal in the same score. Although the prevalence of asymptomatic patients with SLE with SH did not reach statistical significance in comparison to healthy controls, both SH index and GLOESS were significantly higher in the asymptomatic SLE population when compared with the control group. Altogether, these findings encourage the use of global US scores for a more detailed joint evaluation in SLE, in clinical practice and in future trials.
Compared with the study of Yoon et al,14 our study detected a higher prevalence of SH (grade≥1) in asymptomatic patients with SLE. While the previous study identified joint effusion and/or SH in 58% of asymptomatic patients with SLE, we detected SH (grade ≥1) in 77% asymptomatic patients with SLE. This may be due to the larger number of joints examined in our study (22 joints per patient, in comparison with 3 joint recesses in the previous study—wrist, 2nd and 3rd MCP) and to the higher frequency of our linear array probe (15 MHz, in comparison to 10 MHz in the previous study). However, while the previous study classified these 58% of patients as having subclinical synovitis, only 23% of the asymptomatic patients with SLE in our study were classified as having subclinical joint inflammation.
In our study, patients with abnormal US PD findings did not show significant differences regarding demographic, clinical and laboratory data when compared with those with normal US PD findings. In addition, no significant correlation was found between US PD variables and disease activity or organ damage scores. This is in agreement with several previous studies, suggesting that global assessment of patients with SLE should be complemented by imaging modalities, such as US.35 ,37 ,39 Interestingly, patients under treatment with oral prednisolone had higher PD indexes. In addition, the prevalence of PD signal and PD indexes were significantly higher in the symptomatic patients with SLE when compared with the asymptomatic patients and controls, suggesting that PD signal could be considered a marker for active musculoskeletal disease.36
The most important limitations of our study are the moderate sample size (which may limit generalisability) and the high prevalence of steroid use among the SLE population (which could reduce the global inflammatory burden and result in lower prevalence and grading of the US PD findings). Furthermore, intake of non-steroidal anti-inflammatory drugs at the time of US imaging, a potential confounder in US PD evaluation, was not accounted for. Although US-detected subclinical joint abnormalities have been previously associated with the development of musculoskeletal symptoms, the prognostic value of these findings remains to be determined. Larger longitudinal studies are required to confirm the significance of subclinical US PD findings, specifically regarding the predictive value for the development of long-term joint damage.13 ,40
In conclusion, a small subgroup of patients with SLE without artralgia or clinical evidence of arthritis may present subclinical joint inflammation. Global US scores and PD signal may be important in disease evaluation and therapeutical monitoring.
References
Footnotes
Contributors All persons who meet authorship criteria are listed as authors, and all authors certify that they have made substantial contributions to the work to take public responsibility for the content. Each author agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication. Specific contributions made by each author: Category 1 – Conception and design of study: CAR, SP, LSV, MFMF: Acquisition of data: CAR, RMo, JFO, SP, LSV, MFMF: Analysis and/or interpretation of data: CAR, MFM-F. Category 2 – Drafting the manuscript: CAR MFMF – Revising the manuscript critically for important intellectual content: CAR, RM, JFO, SP, LSV, MFM-F. Category 3 – Approval of the version of the manuscript to be published: CAR, RM, JFO, SP, LSV, MFM-F.
Competing interests None declared.
Patient consent Obtained.
Ethics approval All procedures performed were in accordance with the ethical standards of the Institutional Ethics Committee ((Comissão de Ética do Centro Hospitalar de Lisboa Central; approval number 1115 (2014)) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.