Article Text

Abstract
Objective There is a pressing need for high-quality, comprehensive research to describe the natural history, best treatments, access to care and disparities in care for patients with childhood-onset SLE (cSLE). Building on a previously published survey study of cSLE clinicians and researchers to describe research priorities in cSLE, the primary objective of this study was to conduct expert interviews to define high-priority areas for cSLE research.
Methods Individuals with identified multidisciplinary expertise in cSLE were recruited worldwide using purposive sampling technique. Experts participated in open-ended, semistructured qualitative interviews. Interviews were designed to elicit expert perspectives on research priorities, optimal research approaches, and factors that facilitate and hinder advancing cSLE research. Interviews were digitally recorded, transcribed and de-identified for analysis. Analysis for underlying themes of cSLE expert perspectives was performed using a constant comparative approach.
Results Twenty-nine experts with diverse clinical and research backgrounds participated. Themes emerged within five domains: (1) expanding disease knowledge; (2) investigator collaboration; (3) partnering with patients and families; (4) improving care to optimise research; and (5) overcoming investigator barriers. Choosing a singular area of focus was difficult; experts identified many competing priorities. Despite the numerous priorities that emerged, experts described several existing and potential opportunities for advancing cSLE research.
Conclusions In addition to the priorities identified by cSLE experts in this study, the opportunities for advancing cSLE research and care that were proposed should be used as a foundation for creation of a cSLE research agenda for both research and funding allocation.
- Qualitative research
- Lupus Erythematosus, Systemic
- Patient Care Team
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
WHAT IS ALREADY KNOWN ON THIS TOPIC
Although there have been significant advancements in the understanding and treatment of childhood-onset SLE (cSLE), significant knowledge gaps remain.
WHAT THIS STUDY ADDS
This qualitative study examined perspectives from a diverse group of clinicians and researchers with expertise in areas relevant to cSLE to identify barriers as well as research strategies to advance understanding and care of patients with cSLE.
Experts had difficulty selecting a singular area of focus to delegate resources reflective of many areas of need; identified priorities encompassed expanding knowledge of the disease itself, partnering with patients and improving their care to optimise research, and enabling investigator collaboration as well as overcoming individual investigator barriers.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
The proposed solutions to barriers to advancement of cSLE research in this study should help guide a cSLE research agenda and may inform future funding priorities.
Introduction
SLE is a chronic, relapsing autoimmune disease affecting multiple organ systems; an estimated 10%–20% of patients with SLE have childhood-onset SLE (cSLE), defined as SLE diagnosed prior to 18 years of age.1 cSLE has been shown to be more aggressive than adult-onset disease; children and adolescents suffer greater complications of the disease than adults, including more widespread organ involvement and higher disease activity.2 3 Given the early onset of cSLE, patients often experience significant burden due to comorbidities and immunosuppressive treatment over their lifespan.1 3 Although there are similarities between cSLE and adult-onset disease, there are unique considerations in the paediatric population, such as puberty, neurodevelopment, disease and medication effect on growth, drug metabolism, and medication efficacy,2 in addition to the need to partner with the child’s caregiver/family. Knowledge gaps remain in these areas, and there is a pressing need for high-quality, comprehensive research efforts to define the natural history, best treatments, access to care and disparities in care for patients with cSLE.4
In 2015, the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) released an SLE research plan on behalf of the National Institutes of Health (NIH) which included broad areas for potential focus. cSLE (defined as a special population within the plan) made up a very small part of the overall research objectives. More recently, the Addressing Lupus Pillars for Health Advancement (ALPHA) project, a two-phase study, conducted expert interviews to inform a global survey of SLE experts to identify, prioritise and develop strategies for advancing SLE research, care and access as phase I of the study. Although paediatric rheumatologists were included in both the initial interview and survey components, only 6% of survey respondents primarily practised paediatric rheumatology. Responses of phase I of the ALPHA survey indicated that the lack of attention to paediatric issues is a barrier to SLE drug development and clinical care5; however, specific aspects of these issues were not detailed. Subsequently, phase II of the ALPHA study proposed actionable solutions to the identified research barriers from phase I of the study. Increased representation of paediatric patients in clinical trials was named as a solution to the previous barriers that had been identified in phase I of the study.6
To expand on the NIAMS-identified objectives and ALPHA study results, the Childhood Arthritis and Rheumatology Research Alliance (CARRA) and the Lupus Foundation of America (LFA) partnered to identify key knowledge gaps and strategies for advancing cSLE research. An initial objective of this collaboration was to prioritise cSLE research domains by surveying rheumatologists, nephrologists and dermatologists with expertise in cSLE.7 The previously published survey study identified the highest prioritised domains as SLE nephritis, clinical trials, biomarkers, neuropsychiatric disease and refractory skin disease.7
Building on this survey study, the objective of the current qualitative interview study was to further characterise and elaborate on high-priority areas of cSLE research. This follow-up study examined perspectives from multidisciplinary and international providers with expertise in cSLE care and research aiming to identify (1) areas of high priority in cSLE research; (2) best research approaches to address these areas; and (3) barriers and facilitators to advancing cSLE research.
Methods
Study design and patient and public involvement
Individual interviews were conducted to elicit perspectives from cSLE experts, to further characterise and elaborate on the priority domains, and identify new domains. Patients were not recruited to be part of this study and there was no public involvement.
Setting and participants
Using purposive sampling, 39 individuals with a range of expertise in cSLE were invited to participate in semistructured, individual interviews. Investigators identified experts through review of authors for cSLE research publications, review of investigators and collaborators within CARRA, and discussion with leaders in cSLE research. We aimed to sample individuals with expertise in clinical care and/or research related to cSLE, specific clinical and research areas (eg, central nervous system/mental health, nephrology, dermatology, cardiology, immunology) and a variety of research approaches (basic science, genetics, clinical trials, clinical and outcomes research, quality improvement/implementation science). Adult rheumatologists with clinical and/or research expertise in transition to adult care were included, as were several paediatric rheumatologists outside North America for a global perspective.
Twenty-nine individuals from 6 different countries and 23 different institutions were interviewed. The majority of participants practised within the USA and Canada (collectively making up 87% of the interviewees) (table 1).
Expert demographics (N=29)
Experts came from paediatric rheumatology (72%), paediatric nephrology, child psychiatry, adolescent medicine, adult rheumatology and medicine/paediatric rheumatology. They varied in their years of experience after completing training, with providers who had been in practice from 6 to 15 years making up the largest group (41%), followed by those practising more than 25 years (28%).
Data collection
Two interviewers (AC and LC) trained in qualitative interviewing techniques employed a semistructured guide (online supplemental 1) designed to explore experts’ ideas and recommendations on advancing cSLE research. Topics included (1) advances and deficits in the current state of cSLE research, to identify priority areas encompassing disease pathology, comorbidities and healthcare utilisation; (2) optimal research methodologies to investigate identified priority areas; and (3) barriers and facilitators to advancing cSLE research. To further define their thoughts on addressing high-priority research areas, participants were asked: ‘If you could give $10 million to cSLE research, is there a type of project that you think would have the biggest impact?’ Interviews were conducted by phone between January and May 2020 and averaged approximately 35 min (range 20–70 min). They were digitally recorded, transcribed and de-identified. Interviewees consented verbally at the time of the interview.
Supplemental material
Data analysis
Consistent with a constant comparative approach to analysis, experts’ views on the state of cSLE research were iteratively examined to uncover the range of priorities among them.8 9 AC and LC read and synthesised each expert’s interview transcript to capture their observations and recognise points of difference and consensus across experts that would indicate shared priorities.
Nearly half of the interview transcripts were independently analysed and synthesised by both LC and AC, followed by a joint review for alternative interpretations or missed themes. Their independent identification of themes converged within the first set of six interview transcripts. The remaining transcripts were synthesised by AC without secondary review. Next, the themes and excerpted text were organised into broad domains (eg, collaboration, funding, drug development). Together the authors (LC, AC, AH and AMK) explored the compilation of themes, domains and text to characterise the nature of the experts’ perspectives and explore intersections within and across themes.
Results
The priorities proposed by experts included not only ‘what’ to study, but the infrastructure and support needed to carry out that research. Several notable themes emerged and were categorised into five domains: (1) expanding disease knowledge; (2) investigator collaboration; (3) partnering with patients and families; (4) improving care to optimise research; and (5) overcoming investigator barriers. Illustrative quotes are shown in table 2.
Illustrative quotes for qualitative themes for advancing cSLE research
Expanding disease knowledge
Genetics and environment
Experts indicated a need for greater understanding of the underlying genetic pathways of the disease for both identifying risk in preclinical states and determining best treatments (table 2, Q1). Experts pointed out that genetic knowledge as it relates to disease phenotype brings us closer to targeted medications (Q2–Q3). They also acknowledged a need to better understand the relationship between ‘genetic predisposition’ and environment in order to assess susceptibility. Studying the impact of environmental risk factors (violence, poverty, trauma, socioeconomic status, etc) on the development and course of disease may advance approaches to treatment (Q4).
Need for biomarkers
Experts described cSLE as a heterogeneous disease and emphasised the need for biomarkers to better characterise each individual’s disease. They also identified biomarkers as critical to predicting organ involvement as well as a way to enable targeted therapy and potentially lead to new drug targets (Q5–Q6). Experts noted the need for biomarkers and targeted therapy frequently in the context of research devoted to cSLE nephritis and neuropsychiatric disease, given the significant morbidity associated with these disease manifestations (Q7).
Paediatric clinical trials
Experts described the efficacy of therapies for cSLE as being largely extrapolated from adult data and highlighted the need for paediatric clinical drug trials to advance therapeutic options in cSLE. Experts voiced frustration that if a medication is not effective in an adult study, then it will never be known if it would be effective in treating patients with cSLE, and that there is a delay between medications’ use in adult care versus use in paediatric care (Q8). Medications were also discussed from the perspective of adherence and the need for medications that are more palatable to patients with less side effects and that work quickly (Q9).
Longitudinal outcomes
Experts said that longitudinal studies are critical to better understanding the long-term effects of treatment as well as long-term organ damage and mortality, especially in the context of nephritis and neuropsychiatric disease (Q10). When designing such studies, experts suggested researchers consider the quality, standardisation and organisation of data sources such as electronic medical records (EMRs) or registries. Many experts noted that longitudinal design is particularly suited to studies of transition from child to adulthood and to examining the long-term effects of medications. Patient registries were discussed as a tool to follow patients longitudinally, specifically the CARRA registry (Q11). It was noted, however, that longitudinal data capture may be limited by insurance changes and transition to adult care (Q12). The increasing sophistication of the EMR was noted as an opportunity to capture these data, but the cost of such studies was identified as a limiting factor. Additionally, experts said that standardised data collection is needed across centres/sites to consistently share information for registries and databases to be useful.
Investigator collaboration
Multicentre collaboration
Given the rarity of the disease, collaboration among centres was identified by experts as a necessity in advancing cSLE research. Investigators need to come together to advance this work with multicentre studies (Q13). Experts pointed to CARRA as a vehicle for research collaboration, especially with the patient registry; it has served to examine variation in care among centres and improve care overall.
International priorities and collaboration
Experts outside of North America explained that international collaboration is particularly important for this rare disease because it increases the number of patients available to participate in studies, in turn enabling samples that represent the total population of children with cSLE. While in North America and Europe the focus is on advancing research, other areas of the world have more urgent needs for investment in basic healthcare, education and advocacy for patients with cSLE (Q14). They also pointed out challenges to fostering international collaboration (eg, regulatory barriers, Institutional Review Board approvals). One expert stated that international collaboration has been more successful on ‘the general aspects of the disease’ but would benefit from collaboration on biomarker studies and genetic studies (Q15).
Multidisciplinary collaboration
Multidisciplinary collaboration was also identified as essential to advancing cSLE research. Experts noted that understanding the multiple impacted organ systems in cSLE requires expertise from specialists across disciplines (eg, nephrologists, neurologists, dermatologists) to investigate the disease in a ‘nuanced and deeper way’ (Q16). Beyond subspecialties the need for partnership between clinicians and scientists from a variety of backgrounds (eg, immunologist, translational scientist, molecular biologist, geneticist, etc) was also emphasised, with experts indicating that a ‘team science’ approach is needed, including the potential of more basic science representation at CARRA meetings as an opportunity for collaboration (Q17–Q18).
Relationship with pharmaceutical industry
Experts noted the general cost of drug development and the unique challenges of drug development in rare diseases as barriers to new cSLE medication options. One expert noted that there needs to be better alignment between the pharmaceutical companies’ motivations and the Food and Drug Administration’s needs (Q19).
Partnering with patients and families
Recruiting and engaging patients
Experts identified recruitment of patients in research as an important research priority, and barriers to recruitment such as lack of adequate staff or time on the part of the provider were discussed (Q20). One expert pointed out that attention to a diverse recruiting staff could encourage more patients, particularly those that would strengthen the representatives of the population in studies. Experts indicated that increased inclusion of diverse patients in research is necessary to capture a representative patient population which limits our understanding of the disease (Q21). The need to engage patients, not only parents, in studies was also emphasised especially in the adolescent population (Q22). Experts emphasised the need to include the family in any research that involves clinical intervention and the importance of involving patients at each ‘phase’ of a project to get their input (Q23).
Including outcomes important to patients
Experts acknowledged, some emphatically, the importance of registering patients’ definitions of success to guide the interpretation of assessments and interventions (Q24). In particular, patient-reported outcomes (PROs) are mechanisms to challenge assumptions about success that may be built into the design of a study. Examples of patients’ concerns include effects of cSLE on education, employment, extracurricular activities and psychosocial well-being (Q25).
Improving care to optimise research
Quality improvement: intersection of healthcare delivery and outcomes
Several experts acknowledged the importance of quality improvement efforts to standardise care across individuals and institutions (Q26). One expert provided examples of the benefits of quality improvement studies, such as monitoring vaccinations, detecting avascular necrosis and osteoporosis, and lipid monitoring (Q27). Experts also noted that how an individual is able to navigate the complex healthcare system—which can be overwhelming for a patient and family—is tied to a patient’s outcome. Effective healthcare delivery is intimately tied to understanding the patient’s support system and the psychosocial impact of the disease (Q28). Therefore, financially prioritising research and support (such as patient navigators) around healthcare delivery was seen as a necessity for advancing cSLE care and ultimately research (Q29). Additionally, standardising the implementation of studies in clinical settings was a concern, particularly in terms of recruitment and ensuring the buy-in and commitment from clinicians to carry out study activities consistently (Q30–Q31).
Optimising mental health
Experts raised questions about the effect of psychological stress from the disease or disease activity and long-term outcomes. They called out the clinical conundrum of determining whether patients’ psychiatric symptoms are a manifestation of primary disease activity or an expression of coping with chronic disease and encouraged devoting resources to develop diagnostic tools to differentiate between the two (Q32). Experts also noted the relationship between mental health and poor adherence to treatment and suggested that improvement in mental health screening may significantly impact outcomes (Q33–Q34).
Improving adherence and transition to adult care
While some experts said that there has been progress on research around adherence, it was identified as a priority given that non-adherence remains a major barrier to the care and outcomes of patients with cSLE (Q35). Experts highlighted the need for research around best practices for promoting adherence, especially for therapies where patients do not experience immediate effect. Experts frequently discussed research and support around adherence in relation to the transition from paediatric to adult care. This was identified as a very vulnerable time for patients and an area where more resources should be dedicated to promoting successful transition to an adult rheumatologist (Q36–Q37).
Overcoming investigator barriers and identifying opportunities
Protected time and funding for research
Many experts identified the lack of time to obtain funding and complete projects as a major barrier to advancing cSLE research. They explained that providers have competing demands, and the obligations of clinical care leave little time to conduct high-quality studies (Q38). Providing time and funding for collaborative projects helps enable patients to be enrolled in studies and for collaborative research organisations to succeed, for example.
Experts noted that current models of compensation—largely based on procedures and volume—are problematic for paediatric rheumatologists given rarity of diseases that they treat, which limits the institutional resources that they are allocated. Experts highlighted the importance of advocating for funding, with one interviewee stating that advocacy is needed to “convince the powers above to come out with [Requests for Applications] for childhood SLE conditions” (Q39). They also expressed the need for more robust funding mechanisms for cSLE projects, with special attention to opportunities for young investigators and trainees considering a research career (Q40).
Mentoring for young investigators
Experts expressed concern about the next generation of researchers due to the major obstacles with funding and beginning in a research-focused career in cSLE (Q41). They were selective about mentees because of this difficulty and the credentials and passion required to persevere. To be successful in a cSLE research career, experts said that young investigators need strong mentorship from more senior researchers, a need that currently cannot be met by the limited pool of senior researchers and their availability. One expert identified adult rheumatologists as a potential mentoring resource given the similarities between cSLE and adult-onset SLE. Other solutions proposed include creating mentorship programming specific to cSLE research with protected time for mentors and organised opportunities for networking among senior cSLE researchers and early investigators.
A path forward: establishing a paradigm for advancing cSLE research
Experts noted the challenges in establishing a clear direction for cSLE research. When asked how they would spend a hypothetical grant of $10 million for cSLE research, nearly a quarter of them explicitly emphasised the difficulty choosing a single focus and some divided the money across multiple methodologies or lines of enquiry. Collection of patient biosamples (blood, urine and tissue) from diagnosis through their disease course for longitudinal characterisation of disease was the most frequent response, with over a third of experts detailing a project related to better understanding of disease biomarkers. These projects were often discussed as a mechanism to enable more targeted drug development. Despite the question’s focus on cSLE research, a fifth of experts indicated that they would spend the money on improving healthcare access and delivery, which was identified as both a major barrier to advancing cSLE research and an important determinant of the patient’s overall outcome.
One expert suggested the following approach to prioritisation in response to the 10-million-dollar question:
I would probably target pathogenesis of the disease with genetic and immunophenotypic disease stratification to somehow get into the disease mechanism as much as possible…one of my teachers said, when you have the biggest emergency there is still time to run once around the hospital and to refresh your thoughts, and then kind of do the best rational thing, the optimal rational thing. So, sometimes you need time to reflect on different aspects and see what is feasible, what is doable, and would have the biggest impact. —Expert U
Another expert asserted the importance of starting from a paradigm rather than a priority, explicating the tension between numerous and varied priorities, and calling out how difficult it is to prioritise research efforts when there is “so much to be done.”
So this is a problem we have in the field – we have a problem that there’s so much to be done, it’s really difficult to prioritize. And the question is – what is the basis for prioritization? Is the basis number of people affected…or should you give higher priority to things that are easier to do? Is it based on feasibility or should you give higher priority to things that are an emerging cool technology or biology…We don’t have agreement on what we should say are the features on which to prioritize…we’ve prioritized kidney disease and neuro – brain disease because it’s a higher mortality and morbidity. That’s another way to prioritize things…But what we really need isn’t to know what to work on. What we really need is to know how to work on it…People have been trying, trying, trying in both the pediatric and adult arena to address a whole array of lupus phenomenon. And our lack of progress isn’t because we don’t know where to focus. So prioritization is helpful if you want to know where to put all your money or where to start. But I don’t think that the lack of progress is because of people not working in a certain area…we haven’t figured out a path of investigation – a path of research that advances the science and the knowledge well enough. —Expert G
Similarly, two other experts stated the value of being intentional about setting such a direction, with one (Expert X) noting that in the field of autoinflammatory disease “they now have paradigms for how to study it and we still don’t have a good paradigm for how to understand and study lupus.”
Discussion
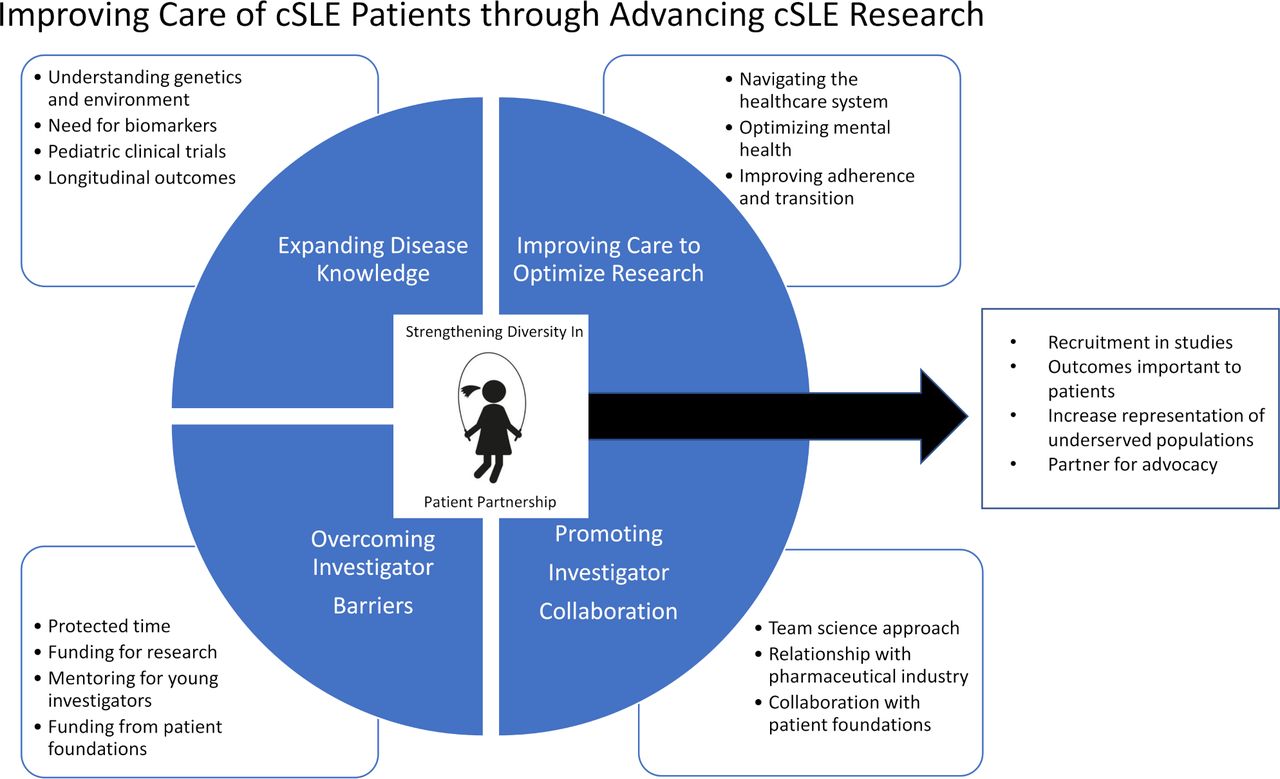
While there have been advances in understanding disease mechanisms and treatment of cSLE in the last decade, significant needs remain, underscoring the necessity of a focused research agenda for allocation of available resources. Expanding on the findings from the ALPHA study5 6 and CARRA-LFA survey regarding cSLE research priorities,7 we elucidated approaches to address cSLE research priorities, exploring both barriers and opportunities to advancing cSLE research. Multidisciplinary experts in our study identified research priorities represented by five domains: (1) expanding disease knowledge; (2) investigator collaboration; (3) partnering with patients and families; (4) improving care to optimise research; and (5) overcoming investigator barriers. Many interviewees had difficulty selecting a single priority, and the need for a broader paradigm framework for cSLE investigation was identified. Additionally, and notably, partnership with patients emerged as a unifying factor for advancing research (figure 1).
{kind=link}
A visual representation of study themes. The figure proposes that research priorities for cSLE are captured by five interrelated themes, which include disease knowledge, investigator collaboration, improving care to optimise research, investigator barriers and patient partnership (depicted in the centre of the figure). Patient engagement, patient partnership and health equity in research endeavours are central to the development of any proposed research agenda, and the other four themes rely on engagement of patients and health equity for their advancement. cSLE, childhood-onset SLE.
We identified not only barriers but also numerous opportunities for progress (box 1). Our findings represent an initial step in formulating a research agenda and funding priorities for the cSLE community.
Opportunities for advancing childhood-onset SLE (cSLE) research
Collaboration
Interdisciplinary collaboration across subspecialties and scientific disciplines to engage in a team science approach.
Multicentre and multinational collaboration to develop larger representative cSLE patient cohorts with diverse disease manifestations.
Efforts to reduce regulatory barriers to collaboration (eg, Institutional Review Board, Food and Drug Administration).
Longitudinal data
Address gaps in clinical care, with attention to enhance standardised, comprehensive and longitudinal data collection.
Longitudinal patient registry data collection from paediatric disease onset through adulthood.
Data management and infrastructure support across centres/sites to share standardised electronic medical record data and link to other data sources (eg, registries, administrative data).
Patient involvement in research
Improve healthcare delivery, with particular focus on underserved populations, to empower participation in research.
Engage patients and families to determine meaningful research questions and outcomes and to enhance recruitment of diverse populations.
Include patient-reported outcomes in study design.
Include diverse staff on research teams.
Investigator support
Increase funding opportunities for early investigators to pursue cSLE-related projects.
Dedicated mentorship programming for cSLE research, including funded protected time for cSLE mentors.
Facilitated networking among senior researchers and early investigators.
Experts identified a need for a path of investigation in lupus research, described as a paradigm framework to guide ‘how’ to do the research, which would also inform ‘what’ to research. A comparison was made to the field of autoinflammatory disease research, which has seen recent significant advances due to international and interdisciplinary collaboration, and harnessing of genomic and molecular technologies to link genotype to biological pathways to phenotype.10 This has resulted in better diagnostic tools and target immunosuppressive treatment in autoinflammatory disease. A similar paradigm for lupus research, addressing the complexity and heterogeneity of the disease, would be optimal to guide lupus investigation towards improving patient care. Experts emphasised the importance of a research agenda that promotes collaboration among investigators with different expertise (immunology, genetics, basic science, translational science, etc). With regard to translating findings to the clinical setting, experts also identified biomarker and drug development as prominent priority areas, acknowledging the unique regulatory and ethical considerations that exist in studies involving paediatric patients.
One promising model of investigation is the Accelerating Medicines Partnership (AMP),11 12 which has enabled successful collaboration between the NIH, pharmaceutical companies and non-profit organisations, bringing together individuals of varying backgrounds and expertise to push the science forward. The AMP initiative has supported ‘team science’ studies in the adult SLE population, for example, with one published study using single-cell RNA sequencing technology to examine heterogeneity of lupus nephritis and skin disease, and identifying cellular changes on skin biopsy as a potential biomarker for lupus nephritis.11 A trans-NIH initiative (across specialties) could be another potential opportunity for multidisciplinary collaboration to understand lupus disease heterogeneity given the multiorgan involvement in cSLE. Fostering team science collaboration inclusive of cSLE (both within cSLE and SLE research in general) will be critical to advancing research and discovery in cSLE, furthering knowledge of potential targets for more effective and less toxic medications (box 1). Furthermore, although there has been advancement in cSLE trials in recent years,13 treatment development in cSLE will likely require innovative smaller trials with specific endpoints given the rarity and heterogeneity of the disease.14
Another potential area for collaborative research is creating purposeful synergy between existing and newly created cSLE observational registries in order to optimise the breadth and depth of the data collected. Longitudinal observational registries which capture the full breadth of patient demographics, disease manifestations, treatments and response are critical to understanding cSLE’s natural history and short-term and long-term outcomes. Harmonisation of data fields can allow for comparison or combination of related registries, which may be essential when describing less common disease manifestations or treatments. These registries are even more powerful when paired with biosample collection, allowing for determination of both clinical and biologic factors which may contribute to fluctuations in disease activity and outcomes.
Although there was significant emphasis on research of the disease itself and its manifestations, patients’ barriers to engaging with the healthcare system (eg, transportation to clinic, reliable methods to communicate with providers) were a less expected, yet significant finding. This echoes priorities in the 2015 National Public Health Agenda for Lupus developed by a collaborative of the LFA, the Centers for Disease Control and Prevention, the National Association of Chronic Disease, and leading lupus and public health advocates,15 calling for improved lupus care coordination, self-management programmes, resources and identification of health disparities. Notably, SLE mortality risk is significantly impacted by race, with black females having increased mortality from SLE as compared with other individuals with SLE.16 17 Additionally, although individuals from racial minority groups make up a large proportion of patients with SLE in the USA, white participants are over-represented in SLE randomised control trials.18 Health equity research is therefore greatly needed to eliminate ongoing health disparities in SLE.15
To address the lack of adequate representation of racial minority groups in SLE research, a 2019 conference among patients with SLE, SLE physicians, clinical trialists, treatment developers from biotechnology, social scientists, patient advocacy groups and US government representatives explored solutions for increasing diversity in SLE research studies.19 Best practices for clinicians and researchers were developed, which included reflecting on how personal and institutional culture lead to racial bias in research questions and study design, the need to avoid making assumptions about the ‘kind’ of patient who would participate in a trial, and increasing recruitment of under-represented minorities to the field of rheumatology. Experts in our study expressed several opportunities to address these issues, including having a diverse research staff, including outcomes that are important to patients and utility of funding for patient navigators (box 1).
cSLE researchers face significant challenges—namely funding and protected time from clinical obligations—that impede their participation in multicentre studies or to procure data for registries to support longitudinal studies of diverse cohorts. As experts pointed out, this milieu discourages the number of early career faculty who pursue research careers, leading to fewer cSLE investigators and an inevitable lack of diversity in their research backgrounds. Academic institutions have created programmes to address this need,20–22 but it remains a critical issue across paediatric subspecialties and particularly in cSLE research given the small size of the paediatric rheumatology field.
As one of the smallest paediatric subspecialties, often with small institutional divisions,23 interinstitutional mentorship is crucial for trainees and early career faculty in paediatric rheumatology. The ACR/CARRA Mentoring Interest Group24 25 has established connections between individuals at different institutions for career mentorship. Even with funding (such as a mentored career development award, eg, NIH K award), the number and availability of mentors for cSLE research are limited. Grants that protect time for mentors, K24-like funding and Request for Application opportunities related to research mentorship from the LFA or Lupus Research Alliance are potential solutions to foster investigator mentoring (box 1). Patient advocacy efforts through private foundations could also fill such a role (figure 1).
There are a number of strengths in our study. To our knowledge, this is the largest qualitative study of cSLE experts regarding cSLE research priorities. The group of experts had diverse backgrounds, including their disciplines (eg, nephrology, dermatology, medicine/paediatrics rheumatology), years in practice and research backgrounds. There was also international representation. A limitation of our study is that patients were not included in our study, risking misalignment between patients’ priorities and those of experts. A follow-up study is planned to include patients’ perspectives, priorities and perceived barriers to being involved in research.
In conclusion, the findings of this study highlight the importance of a collaborative research framework and the interdependence of the essential components needed to advance cSLE research and patient care. These findings can inform an actionable research agenda that incorporates the complexity of foundational challenges that investigators in cSLE research face. Funding and limited infrastructure remain a major limitation, yet the potential solutions posited by experts should be prioritised in future request for applications for work related to cSLE.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted with institutional review board approval from the University of Utah (IRB 00127132).
Acknowledgments
This study was supported by the Childhood Arthritis and Rheumatology Research Alliance and the Lupus Foundation of America. The authors would also like to thank the individuals who participated in the interviews.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors were involved in drafting the manuscript. All authors read and critically revised the manuscript for intellectual content, approved its final version prior to submission and agree to be accountable for all aspects of the work.
Funding The authors received funding from the Lupus Foundation of America through the LFA-CARRA Lupus Research Prioritization Study.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.