Article Text

Abstract
Objective To investigate second kidney biopsy as predictor of end-stage kidney disease (ESKD) in active lupus nephritis (LN).
Methods Patients with biopsy-proven LN (International Society of Nephrology/Renal Pathology Society 2003) who had undergone a second kidney biopsy between January 1990 and December 2018 were included. Clinical and histological findings at first and at second biopsy were analysed with Cox proportional hazard models to predict ESKD, defined as start of kidney replacement therapy. Survival curves were calculated with Kaplan-Meier method.
Results Ninety-two patients with LN were included, 87% females, mean follow-up 17.9±10.1 years. Reasons for second kidney biopsy encompassed nephritic flares (n=28, 30.4%), proteinuric flares (n=46, 50%) or lack of renal response (n=18, 19.5%). Class switch from first biopsy occurred in 50.5% of cases, mainly from non-proliferative towards proliferative classes. Class IV remained stable in over 50% of cases. Twenty-five patients (27.2%) developed ESKD, mostly belonging to the nephritic flare group (17/28, 60.7%). Independent predictors of ESKD at second biopsy were activity index (AI; (HR 95% CI) 1.20 (1.03 to 1.41), p=0.022), chronicity index (CI; 1.41 (1.09 to 1.82), p=0.008) and 24h-proteinuria (1.22 (1.04 to 1.42), p=0.013). AI≥2 (log-rank p=0.031), CI >4 (log-rank p=0.001) or proteinuria ≥3.5 g/day (log-rank=0.009) identified thresholds for higher ESKD risk. In a subgroup analysis, glomerular activity and tubular chronicity mostly accounted for AI and CI association with ESKD. No histological or laboratory predictors emerged at first biopsy (95% CI): AI: 0.88 to 1.19; CI: 0.66 to 1.20; proteinuria 0.85 to 1.08.
Conclusions Findings at second but not at first kidney biopsy in patients with persistently active or relapsing LN inform about ESKD development in a long-term follow-up.
- Lupus Nephritis
- Lupus Erythematosus, Systemic
- Inflammation
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Second biopsy may add pieces of information in defining lupus nephritis (LN) course.
WHAT THIS STUDY ADDS
We provide evidence that second diagnostic kidney biopsy is more informative than the first biopsy in predicting end-stage kidney disease (ESKD).
We identify thresholds for activity index ≥2, chronicity index >4 and proteinuria ≥3.5 g/day at the time of second biopsy as factors that predict subsequent ESKD in patients with persistently active or relapsing LN.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This study identifies handy parameters at second biopsy to be followed up which may significantly influence patient prognosis.
It supports the utility of second biopsy for a better long-term stratification of patients with active LN, regardless of class switch.
The identification of high AI in the second kidney biopsy as long-term prognostic factor might have therapeutic implications.
Introduction
The performance of a second kidney biopsy in patients with lupus nephritis (LN) has been a matter of debate for a long time.1–6 In fact, while it is accepted that an early renal response is associated with a better renal outcome,7–10 predictors of renal dysfunction and end-stage kidney disease (ESKD) are difficult to pinpoint in a short-to-mid timeframe, when an overt decline of renal function may not be apparent.11 In this regard, the validity of clinical predictors is still debated,12 whereas increasing evidence suggests that a second biopsy may provide more solid information concerning the risk of renal flares4 6 and eventually kidney failure,2 3 6 occurring in up to 30% of patients.13 14 Moreover, a systematic, multicentric trial aiming at investigating the prognostic effect of repeating kidney biopsy in LN is underway (REBIOLUP).12 The blossoming of data regarding renal rebiopsy testifies the eagerness of clinical scientists to improve LN management; on the other hand, it underlines the uncertainty concerning the interpretation of renal findings as long-term predictors.
Indications for rebiopsy are not unanimously accepted outside recommendations for LN flares,15 16 overlooking a relevant portion of patients with suboptimal response.
In this study, we investigated the clinical and histological findings at second diagnostic kidney biopsy in a large cohort of patients with persistently active or flaring LN on initial treatment and their prognostic value on the development of ESKD. We also compared the predictors of ESKD at the first and second kidney biopsy.
Patients and Methods
We analysed a subgroup of patients selected from a multicentric cohort of 381 patients with LN11 across four Italian Rheumatology and Nephrology referral centres who received standard of care for LN, consisting in prednisone in combination with synthetic immunosuppressants, including mycophenolate mofetil, azathioprine, calcineurin inhibitors or cyclophosphamide and addition of angiotensin-converting enzyme inhibitors.15 We included in the present work adult (≥18 years old) patients with a biopsy-proven LN who underwent a second diagnostic kidney biopsy due to development of a renal flare or lack of complete response despite standard initial treatment,11 limiting the time period for inclusion from January 1990 onwards, due to data availability and homogeneity in the treatment schedule.
Exclusion criteria were the presence of other renal diseases and the pre-existent need for kidney replacement therapy. Patients displaying incomplete clinical records were as well excluded. A retrospective analysis of prospectively collected clinical and histological data was performed.
The set outcome was the development of ESKD and the primary aim was to evaluate predictors of ESKD at second kidney biopsy. The secondary aim was the comparison between predictors at second versus first kidney biopsy.
Patient assessment
LN was classified according to the 2003 International Society of Nephrology/Renal Pathology Society (ISN/RPS) criteria;17 chronicity index (CI) and activity index (AI) were assessed according to Austin et al.18
Demographics, clinical and laboratory features at first and second kidney biopsy and at last observation were recorded in a shared database. End of follow-up was defined as development of ESKD, or last observation or death in patients who did not develop ESKD.
Renal variables
Normal renal function: serum creatinine ≤1 mg/dL and estimated glomerular filtration rate (eGFR) >60 mL/min/1.73 m2 by CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration).
ESKD: start of kidney replacement therapy.19
Proteinuria: measured by benzethonium chloride on the urine collected over 24 hours expressed as g/24 hours.
Arterial hypertension: mean of three consecutive measurements of systolic blood pressure >140 mm Hg and/or diastolic blood pressure >90 mm Hg in sitting position.
The reasons for rebiopsy were classified as follows:
Nephritic flare: increase in serum creatinine of at least 30% over the last value associated with nephritic urinary sediment, with or without increased proteinuria.20
Proteinuric flare: increase in proteinuria without modification of serum creatinine of at least 2 g/24 hours if the previous proteinuria was <3.5 g/24 hours, or a doubling if previous proteinuria was ≥3.5 g/24 hours.20
Lack of complete response: proteinuria ≥0.7 g/day for more than 1 year from the start of induction treatment and normal or near-normal eGFR.11 15
Patient and public involvement
This research was carried out without patient involvement. Patients were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Statistical analysis
Descriptive statistics are reported as mean and SD for continuous variables, and as counts and percentages for dichotomous variables. The difference of continuous variables between groups was tested with non-parametric Mann-Whitney test for independent samples. χ² test was used to test associations of qualitative or dichotomised variables among groups of patients.
Inferential analysis was performed using the Cox proportional hazard model. Both univariable and multivariable analysis were performed. Kaplan-Meier estimate was used to draw survival curves and Mantel-Cox log-rank test was used to test their difference.
In the multivariate analysis, we tested variables with potential clinical significance.21
Patients lost to follow-up were censored at last observation. The SPSS statistical package 26 (Chicago, Illinois, USA) was used.
Results
Study cohort
Ninety-two patients with LN were included in the study, 84 (91.3%) of Caucasian ethnicity, with a mean age 35.1±10.56 years at second kidney biopsy.
Reasons for repeating kidney biopsy were nephritic flare (Group 1, n=28, 30.4%), proteinuric flare (Group 2, n=46, 50%) or lack of complete response LN (Group 3, n=18, 19.5%). Demographic, histological, therapeutic intervention and clinical features of patients from different groups are reported in table 1.
Demographic, histological and clinical features at second renal biopsy and at disease outcome in patients from different groups (expressed as mean (SD) unless differently specified)
In total, 25 (27.2%) developed ESKD after a mean time of 9.04±9.48 years from the second biopsy. The prevalence of patients developing ESKD varied significantly, being predominant within Group 1, that is, nephritic flare group (60.7% (17/28) Group 1 vs 13% (6/46) Group 2 vs 11% (2/18) Group 3, p<0.001)).
Six out of 25 patients (24%) who had developed ESKD died along the study, vs 5/67 (7.4%) patients who had not developed ESKD (p=0.06).
Demographic, histological and clinical features of patients according to development of ESKD are reported in table 2.
Demographic, histological and clinical features at second renal biopsy according to renal outcome (reported as mean (SD) if not otherwise specified)
Predictors of ESKD at second kidney biopsy and comparison with first biopsy
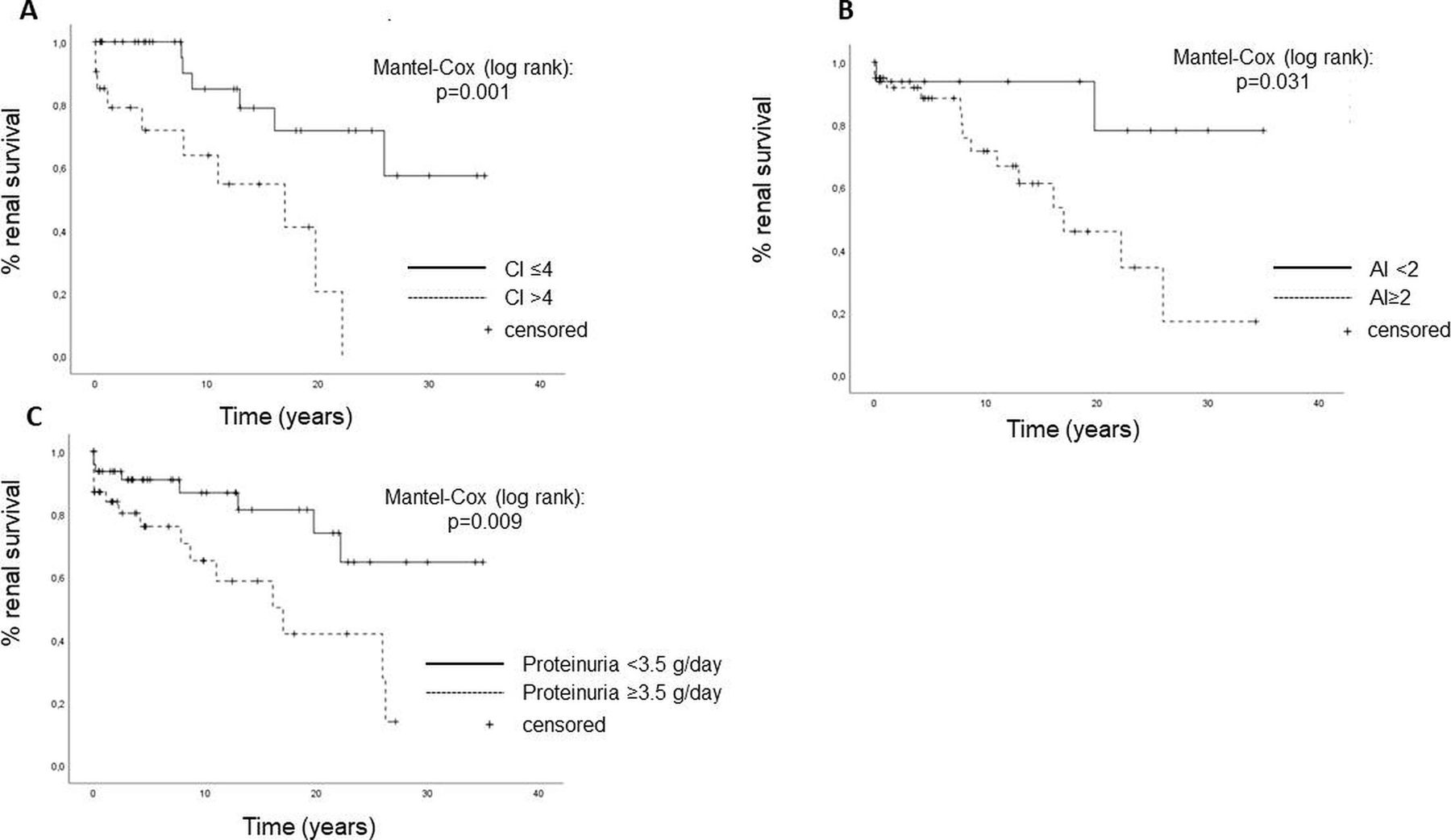
At univariate analysis, several clinical and histological factors present at second biopsy were associated with ESKD (table 3). Cox multivariable analysis highlighted CI (HR (95%CI): 1.41 (1.09 to 1.82), p=0.008), AI 1.20 (1.03 to 1.41), p=0.022), and proteinuria at second biopsy (1.22 (1.04 to 1.42), p=0.013) to be independent predictors of ESKD (table 3). Values of CI >4, AI≥2 and proteinuria ≥3.5 g/day identified patients at higher risk for ESKD at Mantel-Cox analysis (figure 1 and online supplemental table S1).
Supplemental material

{kind=link}
Risk graphs divided by histological parameters and proteinuria show critical values. (A) Patients with CI>4 or (B) AI≥2 at second biopsy are at significantly higher risk of ESKD during their clinical course. (C) Patients with proteinuria ≥3.5 g/day at second biopsy are at significantly higher risk of ESKD during their clinical course. Survival calculated with Mantel-Cox long-rank test. AI, activity index; CI, chronicity index; ESKD, end stage kidney disease.
Predictors of ESKD at second kidney biopsy
Importantly, histological indexes and proteinuria at first kidney biopsy did not predict subsequent ESKD (AI: 95% CI 0.88 to 1.1, p=0.8; CI: 95% CI 0.08 to 1.4, p=0.6; proteinuria 95% CI 0.9 to 1.1, p=0.8), whereas arterial hypertension did (HR 7.20 (2.11 to 24.52), p=0.002). Independent predictors at first and second biopsy are summarised in online supplemental table S1).
In order to check for overfitness and to test the influence of other clinically meaningful independent variables at second kidney biopsy, we tested different Cox regression models (online supplemental table S2) which confirmed the above stated predictors for ESKD in the whole patient cohort.
Supplemental material
Itemised data for AI and CI scores at second biopsy were available for a subgroup of patients (n=29, including 11 patients developing ESKD). Within this subgroup, glomerular activity and especially presence of subendothelial deposits was associated with increased ESKD risk while tubular chronic lesions showed a trend towards increased ESKD risk, at univariable Cox regression analysis (table 4).
Subgroup analysis (Cox regression univariable models) testing itemised AI and CI scores as predictors of ESKD
Histological class switch from first to second kidney biopsy
At first kidney biopsy, 3 (3.2%) patients displayed class I or II, 15 (16.3%) class III, 49 (53.3%) class IV, 14 (15.2%) class V, 11 mixed (5 III+V and 6 IV+V). At second kidney biopsy, histological record was available for 89/92 patients and showed a total amount of class switch of 50.5% (45/89, (online supplemental table S3).
Supplemental material
Class IV remained stable in 29/49 (59%) cases, while patients with initial class I and II progressed to a proliferative class. No independent predictors of class switch were found.
Modification of CI and AI between first and repeated biopsy
The overall mean CI significantly increased (mean±SD, 1.43±1.61 vs 4.11±2.42, p<0.001) while the AI decreased (7.04±3.89 vs 4.83±3.43, p=0.002) from the first to the second biopsy. The greatest CI increase occurred in Group 1, being as well apparent in Group 3 (lack of response) (online supplemental figure S1A), which may at least partially account for the increased proteinuria in this group. Proportions of patients displaying AI≥2 across groups are shown in online supplemental figure S1B (Group 1, 87.5%; Group 2 65.5%; Group 3 61.8%; p<0.001).
Supplemental material
Discussion
This study, performed on a large real-life cohort of patients with LN with persistently active or flaring LN on initial treatment, has shown that the histological findings at second diagnostic biopsy were the best predictors of ESKD. Importantly, AI and CI at second biopsy outperformed the same parameters evaluated at the first biopsy in terms of prediction of ESKD.
The concept of findings at second biopsy being more predictive for renal survival has been acknowledged in the last decade,6 12 13 16 22 23 with most data concerning prediction of renal relapses rather than terminal renal disease.5 6 In fact, despite the experience linking renal damage to worsened renal outcome,4 6 the true prognostic value of histological lesions in the long run is hard to assess both in clinical trials and real-life cohorts,11 14 likely due to an extensive follow-up required to tell apart hard endpoints such as ESKD.
We have pinpointed high activity at second biopsy as an independent predictor of ESKD. Notably, an AI ≥2 at second biopsy conferred a significant higher risk of ESKD, thereby suggesting that even a moderate histological activity contributes to kidney failure and not only to susceptibility to subsequent flaring. Our observations are consistent with recently published data on increased AI being associated with higher probability of renal function deterioration defined as ≥120% increase of baseline serum creatinine;6 here, we further show this association to hold true for ESKD intended as actual kidney replacement therapy, therefore stressing the need for a profound control of histological activity within an optimised therapeutic decision making. Interestingly, a subgroup analysis highlighted glomerular activity and particularly the presence of subendothelial deposits as major drivers of AI hazardousness.
In line with previous studies,1–6 we have as well shown that high chronicity at second kidney biopsy heralds future ESKD, with values of CI >4 conferring the highest risk. Among itemised domains, tubular chronic lesions showed a trend towards increased ESKD risk in the subgroup analysis, thereby confirming tubular-interstitial lesions as major contributors to renal damage.
It is worth noting that neither active nor chronic lesions at the first biopsy in our cohort could predict ESKD, which differs from earlier cohorts yet adds up to more recent data.6 Hence, it may be reasoned that the lack of prognostic value of histology at first biopsy may be due to a timely diagnosis of SLE and LN, entailing an earlier performance of the diagnostic biopsy in the last few decades,12 24 and to a more aggressive treatment in severe forms,24 which possibly dampens their long-term impact.
Besides, proteinuria at second kidney biopsy resulted as an independent predictor of ESKD and was not correlated to either serum creatinine or histological parameters. Particularly, nephrotic proteinuria ≥3.5 g/day conferred a higher risk in our cohort. In keeping with observations concerning AI and CI, proteinuria at diagnostic biopsy did not predict ESKD. This may be explained by the initial proteinuria reflecting ongoing inflammation, while acting as a persistent damaging stimulus over time,25 independent of the underlying histology. While the association between low proteinuria and favourable outcome has been confirmed,7 the long-term predictive value of increased proteinuria is still debated, as this parameter was not found to predict adverse long-term prognosis in other cohorts.6 Differences in duration of follow-up and patient groups may account for different observations and should raise awareness on the interpretation of clinical findings.
The rate of class switch between first and second biopsy was around 50%, in keeping with other cohorts,26–28 while proliferative classes remained mostly stable. Because an increased AI at second biopsy signified an increased risk in ESKD, this highlights the importance of performing a second kidney biopsy in patients with suboptimal/no response or flaring LN as a tool for long-term risk stratification, regardless of LN class be changed or not.
This study has both strengths and limitations. Among the latter, most are connected to its real-life nature, encompassing the retrospective analysis of prospectively available data and the heterogeneity of the underlying reasons for a repeated kidney biopsy. Additionally, a detailed characterisation of the glomerular and tubule-interstitial compartment in the whole cohort was lacking. On the other hand, this is among the largest studies on the topic of second kidney biopsy in LN in the real-world, providing handy tools for patient stratification which may help to consolidate second biopsy as an advised clinical act.
Conclusion
In summary, we have shown that both high activity and chronicity at second, but not at first, diagnostic kidney biopsy predict ESKD in patients with LN and lack of response or flaring after standard therapy. Besides, proteinuria is confirmed as an independent damaging factor for the kidney which may benefit from additional normalising approaches. Altogether, our data identify easy-to-interpret parameters at second kidney biopsy which may significantly impact on patient prognosis and highlight the need of multicentric studies assessing the indispensability and cost-effectiveness of repeating kidney biopsy in LN, at least in specialised centres, to improve prognostic stratification and prevent long-term deterioration of renal function.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committee of Fondazione Ca’ Granda IRCCS Ospedale Maggiore Policlinico di Milano, Italy (protocol number 505_2019bis). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
GM and LI are joint senior authors.
GM and LI contributed equally.
Contributors Study conception and design: AD, GM, MG, LI. Data collection: all authors. Data analysis: MG, GM, MZ. Data interpretation: MG, GM, AD, LI. Critical reading for important intellectual content: all authors. AD is held responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.