Article Text

Abstract
Objective We have developed a new conceptual model to characterise the signs and symptoms of SLE: the Type 1 and 2 SLE Model. Within the original model, Type 1 SLE consists of inflammatory manifestations like arthritis, nephritis and rashes; Type 2 SLE includes symptoms of fatigue, myalgia, mood disturbance and cognitive dysfunction. Through in-depth interviews, we explored how the Type 1 and 2 SLE Model fits within the lived experience of patients with SLE, with a focus on the connection between Type 1 and Type 2 SLE symptoms.
Methods Semistructured in-depth interviews were conducted among adult participants meeting 1997 American College of Rheumatology or Systemic Lupus International Collaborating Clinics criteria for SLE. Participants were purposefully selected for age, race, sex and nephritis history. All interviews were audio-recorded and transcribed. Data were analysed through episode profile and thematic analysis.
Results Through interviews with 42 patients with SLE, two patterns of Type 2 SLE emerged: Intermittent (n=18) and Persistent (n=24). Participants with Intermittent Type 2 SLE described feeling generally well when Type 1 is inactive; these participants were younger and had more internal SLE manifestations. Participants with Persistent Type 2 described always experiencing Type 2 symptoms despite inactive Type 1, although the severity may fluctuate. Participants with Persistent Type 2 SLE experienced traditional lupus symptoms of joint pain, hair loss and rash, but less often had severe organ system involvement.
Conclusions By listening to the stories of our patients, we found two underlying patterns of Type 2 SLE: Intermittent Type 2 symptoms that resolve in synchrony with Type 1 inflammatory symptoms, and Persistent Type 2 symptoms that continue despite remission of Type 1 symptoms.
- systemic lupus erythematosus
- qualitative research
- quality of life
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The Type 1 and 2 SLE Model was developed to encompass the full range of signs and symptoms of patients with SLE experience. Type 1 SLE symptoms include those classically attributed to inflammation and autoimmunity, including arthritis, rash, serositis, nephritis, central nervous system lupus and certain laboratory findings. Type 2 SLE symptoms include fatigue, widespread pain, mood disturbance and cognitive dysfunction, which have a less clear association with inflammation.
WHAT THIS STUDY ADDS
Through in-depth interviews and qualitative analysis of patient descriptions of their experiences with SLE, we identified two unique patterns of Type 2 SLE: Intermittent and in synchrony with Type 1 inflammatory symptoms, and Persistent despite remission of Type 1 symptoms.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Intermittent and Persistent Type 2 symptoms are likely driven by different pathological processes and would benefit from different approaches to therapy.
Introduction
While current therapy for SLE is directed at the inflammation that leads to organ damage, approximately 75% of patients also experience significant fatigue, mood disturbance, widespread pain and cognitive dysfunction for which immunosuppression is largely ineffective; the aetiology of these symptoms and relationship to inflammation is uncertain.1–8 Widespread pain, fatigue and mood disturbance also occur in the general population, yet the frequency of these symptoms is significantly higher in patients with SLE.9–12 Additionally, fibromyalgia, depression and fatigue have been found to correlate with overall quality of life in patients with SLE, more so than disease activity and organ system damage,7 13 with fatigue and pain often the most debilitating symptoms that impair activities of daily living.14–16 Despite their frequency and severity, these symptoms are not measured by most indices of SLE disease activity. Furthermore, many rheumatologists do not regard these symptoms as an intrinsic part of SLE.
At the Duke University Medical Center, we developed a new conceptual model that incorporates a wider range of symptoms patients experience and places patients into two categories based on their symptom experiences: the Type 1 and 2 SLE Model.17 In its formulation, the Type 1 and 2 SLE Model has been based on the clinical experience of rheumatologists who specialise in lupus management and care. Type 1 SLE symptoms encompass the signs and symptoms that are classically attributed to inflammation. These symptoms, which are recorded in physician-reported measures of SLE disease activity, include arthritis, rash, serositis, nephritis, central nervous system lupus and certain laboratory findings.18 In contrast, Type 2 SLE symptoms include fatigue, widespread pain, mood disturbance, and cognitive dysfunction and are typically not included in physician-reported measures of SLE. While patients often identify these symptoms as a key sign of their disease, physicians frequently ascribe them instead to comorbid depression or fibromyalgia. However, the BLISS-52 and BLISS-76 trials for belimumab found that Functional Assessment of Chronic Illness Therapy – Fatigue (FACIT-F) scores at 52 weeks in the placebo group improved 2 points from baseline, while the belimumab 1 and 10 mg/kg groups improved 4–5 points from baseline (p<0.05). Additionally, in long-term follow-up of patients with SLE taking belimumab, almost half had improvement in fatigue after 6 years, suggesting some Type 2 SLE symptoms may be due to inflammation.19 20
While the course of Type 1 symptoms in SLE has been well studied, the trajectory of Type 2 symptoms and the temporal relationship between Type 1 and Type 2 symptoms are poorly understood. We therefore conducted a qualitative study to explore in depth patients’ experiences with their SLE symptoms, focusing on the pattern of Type 2 symptomatology during the course of disease, and in particular how patients experience the interaction between Types 1 and 2 SLE symptoms.
Methods
Recruitment and selection of participants
Potential participants were enrolled in the Duke Lupus Registry (DLR; Pro00008875) and seen in the Duke Lupus Clinic. The clinic schedule was reviewed weekly to identify potentially eligible participants. The research team included an epidemiologist (AME), qualitative researchers from the Duke University QualCore (AC, KM), a rheumatology fellow (MM), and attending rheumatologists from the Durham Veterans Affairs (DSP) and the Duke Lupus Clinic (JLR, MEBC, LGC-S, JD, RES and KS).
Eligibility for inclusion was determined based on information obtained in the DLR and medical record, as well as through a discussion with individuals’ rheumatologists. We first identified potential participants with an established diagnosis of SLE based on 1997 American College of Rheumatology (ACR) or Systemic Lupus International Collaborating Clinics (SLICC) criteria.18 21 We then used stratified purposeful sampling to identify patients based on individuals’ recent experience with higher versus lower Type 2 severity. Patients were initially screened based on patient-reported and physician-reported measures that were prospectively collected in the DLR from visits to the Duke Lupus Clinic over the preceding ~1 year. High type 1 symptom severity was defined as a Safety of Estrogens in Lupus Erythematosus National Assessment-SLE Disease Activity Index (SELENA-SLEDAI) score ≥6 on at least one visit during the prior year.22 We wanted to capture patients with recently high Type 1 activity, both with flares of activity and chronic activity, so not all patients received a change in therapy for their chronically active disease. High Type 2 symptom severity was defined as a Polysymptomatic Distress (PSD) score ≥12 on at least one visit during the prior year.23 24 Those who had a history of both high Type 1 and high Type 2 symptoms were defined as the Mixed SLE group. We reviewed an average of 4 SELENA-SLEDAI and PSD scores per participant over an average period of 53 weeks for this initial classification. Our clinic regularly uses the PSD during routine clinical care over other patient-reported outcome measures, such as Medical Outcomes Survey Short Form 36 (SF-36), FACIT-F and PROMIS measures, as we find it to be the most clinically useful, quickly interpretable and encompassing measure of Type 2 SLE symptoms.
Once we had stratified potential participants based on their prior year of scores within DLR, we purposefully selected participants within each stratum to encompass a wide range of lived experiences with SLE with respect to race, age, disease duration, disease history and manifestation, including a history of lupus nephritis.25 This was accomplished by having the treating rheumatologist review the patient’s SLE history to ensure they represented patients within their activity group based on physician assessment scores, medications, demographics and hospitalisation. This review also allowed us to overcome limitations of the SLEDAI; for example, a patient with an extensive rash who had a low SLEDAI score of 2 would have been reclassified through chart review as having high Type 1 symptoms. Potential participants were approached about the study during routine clinic visits by their rheumatologist, and interviews were conducted with participants following oral consent.
After conducting interviews with participants with Type 1, Type 2 and Mixed SLE, a theme began to emerge of different patterns of Type 2 SLE symptoms. As is standard practice with rigorous qualitative research, if a theme emerges, a study team can research it further. Therefore, we sought to additionally document the perspective of individuals with both low Type 1 and low Type 2 symptoms in the previous year, defined as the Minimal SLE group. We identified and approached potential participants who had low Type 1 and Type 2 SLE activity. All of these participants had clinical SLEDAI scores of 0, and a PSD score <3 at all visits during the previous 12 months; one individual had low C3/C4 and anti-dsDNA+ in the previous year but no other signs of SLE activity.
Data collection
Semistructured, in-depth interviews were conducted from September 2019 to March 2020 (Type 1, Type 2 and Mixed) and March to April 2021 (Minimal) by two trained interviewers on the telephone (n=40) or in person (n=2). Each interview lasted, on average, 45 minutes. All participants provided oral informed consent before participating, agreed to be audio-recorded with an encrypted recorder and were informed they could stop the interview at any point. All participants completed the full interview. Recordings were subsequently transcribed verbatim.
Interviews were conducted using an open-ended, semistructured interview guide created by the authors. At the start of each interview, participants provided demographic information (age, gender, race, ethnicity, education, employment status, health insurance, marital status and time since SLE diagnosis). During interviews, participants were asked to describe (1) their good and bad days living with SLE, (2) their experiences with a list of symptoms commonly reported by people living with SLE (eg, brain fog, fatigue, hair loss, joint pain, kidney disease, rash or skin issues) and (3) experiences with disease flares (including symptoms experienced, length of flares, triggers, symptoms experienced outside of flares and symptoms that appear to coexist). Participants described experiences throughout their disease course, from onset of first SLE symptoms to present day. The interview concluded with participants describing how they perceive their experiences with SLE fit within the Type 1 and 2 SLE Model.
We aimed to conduct 12 interviews each within the Type 1, Type 2 and Mixed SLE groups, based on research demonstrating thematic saturation is typically reached around 12 interviews.26 After reaching the anticipated sample size during data collection, we assessed informational redundancy, based on interviewer feedback that participants were sharing similar information, to determine whether additional interviews were needed.27 For the Minimal SLE group, because we expected participants to have very similar experiences, we assessed saturation after fewer interviews and found information redundancy after five patients were interviewed.
Analysis
The analytical approach was a combination of episode profile analysis28 and applied thematic analysis.29
First, three SLE researchers (AME, JLR, MEBC) read six transcripts independently and summarised the pattern of Types 1 and 2 SLE symptoms described by each participant, particularly the connection between or independence of Types 1 and 2 SLE symptoms. The researchers then discussed their independent summaries for each participant and reached consensus on the Types 1 and 2 SLE symptom relationship. These steps were repeated for all remaining transcripts in groups of 3–6 until all participants had been discussed. A consensus was reached for all participants; researchers continued discussing their summaries and how each researcher described Types 1 and 2 SLE symptoms interacting for each patient until all three SLE researchers agreed with the final determination. The researchers then identified broader patterns about the relationship between Types 1 and 2 SLE symptoms.
We then used applied thematic analysis to further explore the nuances between the patterns of Type 1 and Type 2 SLE symptoms, focusing on a subset of the interview data: how participants described good days and bad days with SLE. First, three coders (AME, KM, MM) applied structural codes to transcript text to group similar responses together (for example, ‘good day with lupus’, ‘bad day with lupus’). Thematic coding followed, focusing on identifying and then coding the emerging concepts within each structural code (for example, ‘symptoms on a good day’, ‘ability to function on a good day’, ‘frequency of good days’, ‘symptoms on a bad day’, ‘ability to function on a bad day’, ‘frequency of bad days’).29 Analysts conducted seven intercoder reliability assessments over several time points throughout data analysis to ensure their coding of the data stayed consistent. Discrepancies in coding were discussed and resolved, and the codebook and coded transcripts were revised as necessary.
Thematic code frequencies across transcripts were examined to identify the most frequent and salient themes, and other data reduction techniques were used to explore the nuances and to identify subthemes. Descriptions of these themes and subthemes, together with illustrative quotes, were described in analytical summary reports. Additionally, the participants were descriptively compared using demographic data collected from participants and clinical data collected in the DLR, including European Alliance of Associations for Rheumatology (EULAR)/ACR 2019 SLE criteria.30
Patient and public involvement
Patients or members of the public were not involved in the design, conduct or reporting of the research.
Results
We conducted 42 interviews. The median time between the last clinic visit and interview was 4 weeks. Based on our study definition for SLE activity in the past year, we recruited 12 participants with primarily Type 1 SLE symptoms (higher SLEDAI and lower PSD scores over the prior year), 12 participants with primarily Type 2 SLE symptoms (lower SLEDAI and higher PSD scores over the prior year), 13 with both Type 1 and Type 2 symptoms (Mixed SLE), and 5 participants with no recent type 1 or type 2 SLE symptoms (Minimal SLE). Most participants were female (93%) and approximately half were non-Hispanic black, with mean age of 45 years and disease duration of 14.5 years (table 1). Approximately one-third of participants had a history of lupus nephritis (n=15).
Participant characteristics
Patterns of Type 2 symptomatology
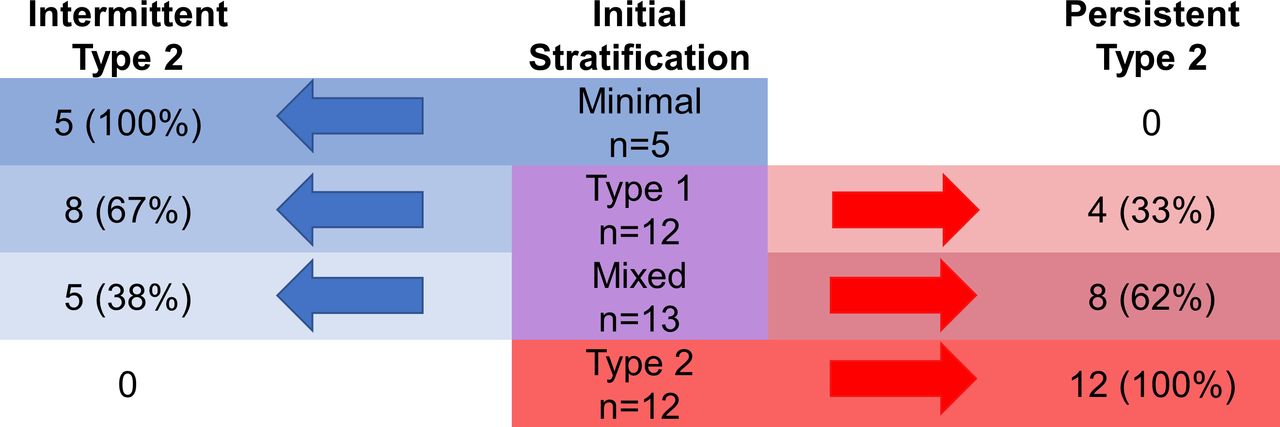
Despite starting with four groups of patients, the patient lived experience revealed two patterns of Type 2 SLE (figure 1). A group of participants described experiencing Type 2 symptoms in tandem with Type 1 symptoms (box 1). As indicated by interviews with participants in this group, Type 2 symptoms can improve and remit when Type 1 disease is inactive; with quiescence of Type 1 SLE, these participants feel generally well. For many of these individuals, when Type 1 is inactive, so is Type 2. We have labelled this group Intermittent Type 2 SLE (n=18). In contrast, another group of participants described Type 2 symptoms as pervasive regardless of Type 1 symptoms. For these individuals, Type 2 symptoms were described as always present, although the severity may fluctuate. One participant referred to this situation as ‘day-to-day lupus’. We have labelled this group Persistent Type 2 SLE (n=24).

{kind=link}
Participants were enrolled through stratified purposeful selection based on the prior 12 months of SELENA-SLEDAI (Type 1 symptoms) and PSD (Type 2 symptoms) scores. At the conclusion of study analysis, we found that all participants with minimal symptoms at the time of the interview described a history of Intermittent Type 2 symptoms corresponding to periods of Type 1 SLE activity. All of the participants within the initial Type 2 group described Persistent Type 2 symptoms regardless of SLE activity. Participants in the Type 1 and Mixed groups, however, divided into the Intermittent and Persistent groups. PSD, Polysymptomatic Distress; SELENA-SLEDAI, Safety of Estrogens in Lupus Erythematosus National Assessment-SLE Disease Activity Index.
Illustrative quotes in participants with Intermittent and Persistent Type 2 symptoms
Connection between Types 1 and 2 SLE symptoms
Intermittent Type 2
‘It’s all hand in hand. You can’t really have Type 1 and not experience something from Type 2. If anything, Type 2 helps me know that this is what is affecting my Type 1.’ (31-year-old woman)
‘Type 1 actually triggers Type 2. Type 1 is where I’m not able to do anything and that’s going to cause my anxiety and it’s going to cause my depression, it’s going to–through anxiety and depression, I’m going to get more fatigued if I’m not already fatigued from Type 1. It’s going to cause my muscle pains and things like that.’ (48-year-old woman)
PersistentTtype 2
‘So, [Type] 1 is active Lupus and [Type] 2 is basically day-to-day lupus.’ (49-year-old woman)
‘[Type] 1 usually for me, besides the hair loss, are coming and going symptoms, and then [Type] 2 are pretty much present, like the fatigue and the depression and things like that.’ (57-year-old woman)
Good days with SLE
Intermittent Type 2
‘A good day is symptom free. I feel like lupus is something that’s not in my consciousness at all.’ (46-year-old man)
‘A really good day is pretty much not having lupus, or before lupus because you aren’t suffering from any symptoms or there’s nothing going on that reminds you of the fact that you have it. At least for me it means that none of my joints hurt, I don’t have any crazy scratches anywhere, and it’s kind of almost like it didn’t happen.’ (32-year-old woman)
Persistent Type 2
‘A good day for me would be waking up with no pain which I rarely ever do. Getting out and doing what I can and being a mom, waking up every morning focused on being a mom.’ (48-year-old woman)
‘A good day is [being] able to get through the day without having to take a nap. I’m always in pain, but maybe it’s more tolerable on those days. That would be a good day.’ (31-year-old woman)
Bad days with SLE
Intermittent Type 2
‘A bad day would be full flare–face swollen, joints swollen, in pain, the rash would be painful to touch, and anything that touches my body would hurt. Those days, I would not get out of bed.’ (24-year-old woman)
‘Joint pain. Constant joint pain. And then not being in the mood to do anything. Tired.’ (27-year-old woman)
Persistent Type 2
‘My body shuts down. A bad day with lupus makes my heart race. It makes everything that could be wrong with me come out… I get cold chills. I’m very exhausted. I have no energy, no strength. I don’t eat. I just wanna lay in bed all day and sleep.’ (59-year-old woman)
‘A bad day is not being able to wake up, [I’m] in pain. If I do manage to drag myself out of bed, try to get in the shower, and push myself, I have to come back and lay down. I never knew that taking a shower could be such an exhausting experience. I can’t handle heat, so I hurt all over, my muscles and joints and everything hurt. I get in the shower, hoping the warm shower will ease up the pain, and then it seems like the heat from being in the shower saps you. What teeny-tiny little bit of energy you had to get in there is now gone… just feeling like you can’t get up and go and do anything. A level of exhaustion I never imagined could be possible.’ (51-year-old woman)
Differences in participant demographics by symptom pattern
Compared with participants with Persistent Type 2 SLE, participants with Intermittent Type 2 SLE were younger (average age of 39 vs 50 years), more were often black (67% vs 42%), and fewer were uninsured or covered by Medicare or Medicaid (33% vs 58%). The groups were similar with respect to other demographics (table 1). Both groups had an average of four clinic visits in the registry.
Participant descriptions of good days and bad days with SLE
One-third of individuals in the Intermittent group said that on a good day, they did not experience symptoms; a few stated that SLE was not even in their consciousness on these days and several described the absence of any joint pain on good days. Others still felt generally well, even if not completely asymptomatic. In contrast, all participants in the Persistent group described symptoms on even their good days. For these participants, a good day was described as fatigue and joint pain that was less severe but nevertheless still present and interfered with their day-to-day functioning. Participants in both groups described feeling more functional on good days, but more participants in the Persistent group discussed their ability to complete activities of daily living on good days, including getting out of the house and socialising, as well as completing household tasks, caring for their family or working.
Participants with both symptom patterns gave similar descriptions of bad days with SLE, with many reporting pain and stiffness, primarily in the joints. Half reported fatigue on bad days, with several also describing joint swelling, brain fog, depression, anxiety and an influenza-like feeling. A few study participants in the Persistent group described feeling incapacitated on bad days. Although both groups described similar symptoms, there were differences in their impact on individuals. Approximately three-quarters of those in the Persistent group described being less functional, with over half reporting staying in bed. In contrast, around one-third of participants in the Intermittent group reported being less functional on bad days, with some describing limited mobility or inability to complete day-to-day activities.
Self-reported symptoms during disease course
A majority of participants in both groups had brain fog and depression at some point since their initial SLE diagnosis, and all but two participants reported experiencing fatigue (table 2). More participants in the Persistent group described experiencing anxiety, muscle pain, fibromyalgia and widespread pain than did participants in the Intermittent group.
Participant-reported symptoms at some time during lupus disease course
The relationship of symptom pattern to classification criteria
All participants met either ACR 1997 or SLICC criteria (table 3). All participants in the Intermittent group and all but five participants in the Persistent group also met 2019 EULAR/ACR criteria. All but two participants were ANA positive; one had a low titre ANA (1:40) and the other was ANA negative but positive for anti-dsDNA antibody. Almost all participants met mucocutaneous (93%) and musculoskeletal (81%) criteria.
2019 EULAR/ACR criteria
Most participants in the Persistent group (63%) met only musculoskeletal, mucocutaneous or constitutional criteria, with or without leucopenia, compared with 22% of participants in the Intermittent group. Almost half of participants with Intermittent Type 2 met renal criteria, with 44% having biopsy-proven lupus nephritis and another 11% having a history of proteinuria. Only five participants with Persistent Type 2 met renal criteria. Of note, these participants described milder Type 2 symptoms than participants with Persistent Type 2 without a history of renal disease. Additionally, more participants with Intermittent type 2 had a history of anti-dsDNA antibody, anti-Smith antibody and low C3/C4.
Discussion
The findings in this study provide new insights into the nature of symptoms experienced by people living with SLE during the disease course. Through in-depth interviews with participants who met classification criteria for SLE, we found that almost all had experienced Type 2 SLE symptoms at some point in their disease. Type 2 SLE symptoms presented in two distinct patterns: Intermittent Type 2 SLE symptoms that can vary in tandem with Type 1 SLE symptoms and Persistent Type 2 SLE symptoms that are present even when Type 1 SLE symptoms are inactive. The two groups defined by the pattern of Type 2 symptoms differed in the persistence and severity of Type 2 symptoms as well as the occurrence of other SLE disease manifestations. Importantly, while all participants described their bad days in similar ways, the two groups indicated very different symptoms and functional abilities on good days.
Patient narratives about their experiences are important to defining disease symptomatology and have helped us in refining our conceptual model of Types 1 and 2 SLE and understanding the relationship between the two symptom categories. Similar to results of other studies, we found that almost all patients with SLE experience fatigue.31 32 Other Type 2 SLE symptoms of muscle pain, anxiety, brain fog and depression were also described by a majority of participants, even among those who were initially classified as Type 1 SLE. Many of the patients in the Intermittent group reported prior episodes of Type 2 symptoms that resolved when their flares of Type 1 SLE receded. While we recruited participants whose symptoms primarily fit into four categories (Minimal, Type 1, Type 2 and Mixed), our analysis demonstrated that this categorisation was inadequate to describe the symptom patterns. First, participants described their experience of Types 1 and 2 SLE symptoms on a spectrum as opposed to binary categories. Second, distinct patterns of correlation and independence of Types 1 and 2 SLE symptoms emerged that led to our conclusion that patients with SLE fit into two patterns of Type 2 SLE: Intermittent and Persistent.
These findings are particularly helpful in our understanding of the Mixed SLE group. Participants in the Persistent Type 2 group described always having Type 2 symptoms that were occasionally accompanied by Type 1 symptoms. In contrast, participants in the Intermittent Type 2 group described having Type 1 and Type 2 symptoms at the same time, with Type 2 symptoms improving as Type 1 symptoms resolved. Both groups would meet criteria for Mixed SLE at cross-sectional time points: Persistent Type 2 symptoms accompanied by occasionally active Type 1 symptoms and Intermittent Type 2 symptoms with coexistent Type 1 activity.
The Intermittent and Persistent groups had distinct disease manifestations over time, suggesting potentially different underlying aetiologies for Type 2 symptoms. While all participants met either SLICC or 1997 ACR criteria for SLE, five participants in the Persistent group did not meet 2019 EULAR/ACR criteria. Participants in the Intermittent group experienced more severe manifestations of SLE over their disease course, encompassing two-thirds of those with a history of lupus nephritis. Participants with Persistent Type 2 SLE and a history of lupus nephritis generally described milder Type 2 symptoms than other participants with Persistent Type 2. This finding of milder Type 2 symptoms in patients with lupus nephritis is supported by results from the Accelerating Medicines Partnership lupus nephritis cohort, which found most patients with isolated renal disease had PROMIS-29 domain scores for anxiety, depression and fatigue similar to the general population.33 Within our cohort, we have found that patients with active lupus nephritis report higher levels of fatigue, sleep impairment and cognitive dysfunction than patients with inactive lupus nephritis, suggesting that these patients may have an intermittent pattern of Type 2 SLE.34
The majority of participants in the Persistent group only met musculoskeletal, mucocutaneous or constitutional criteria, without severe organ system involvement. Additionally, fewer participants in the Persistent group had a history of positive tests for anti-dsDNA antibody and anti-Smith antibodies, and low C3/C4. The 2019 EULAR/ACR criteria have been shown to have superior sensitivity compared with the 1997 ACR criteria and superior specificity compared with the SLICC criteria30; this improvement is consistent across disease duration, sex and race/ethnicity.35 Prior studies of the 2019 EULAR/ACR criteria found that 5%–15% of patients with an established diagnosis of SLE do not meet classification criteria; patients not meeting criteria were primarily those with milder disease.36 37 These findings support the idea that patients with Persistent type 2 SLE may have a more limited form of lupus without major systemic involvement.
Our data suggest that Intermittent and Persistent Type 2 symptoms may be driven by different pathological processes. Most participants in the Intermittent group described symptoms that wax and wane with Type 1 SLE symptoms. It is possible that, in these participants, Type 2 symptoms result from immune mechanisms and would respond to immunosuppression. This possibility may explain the finding that half of patients with SLE in the BLISS-76 long-term extension trial for belimumab experienced improvement in fatigue with treatment.19 20 Future studies will explore this hypothesis further. In contrast, Type 2 SLE symptoms in the persistent group were described as always present. Fluctuations in the severity of these symptoms appear to be independent of Type 1 SLE symptoms and are likely related to other factors, which would not respond to immunosuppression. For this group of patients, different therapies are likely needed, including pharmaceutical and non-pharmaceutical approaches, such as a focus on diet, sleep, exercise or mindfulness.
This first qualitative study of the Type 1 and 2 SLE Model has limitations. We aimed to gather information on a range of patients with SLE who live in the Southeastern USA and receive care at an academic medical centre; we did not include patients from other regions of the USA, other types of medical facilities and non-English-speaking patients. These patients may have other SLE experiences. Furthermore, we asked participants to describe their entire disease experience and, with average disease duration of 15 years, it is possible recall bias may have affected the responses of some participants. Additionally, participants discussed SLE symptoms such as rash, joint pain and kidney disease which they attributed to their SLE, though some of these symptoms were not related to SLE. The PSD, while a measure that encompasses many Type 2 SLE symptoms, does not provide equal weight to all symptoms. As such, a patient who only has extreme fatigue would have a lower score than a patient who has multiple Type 2 symptoms, although the impact on their quality of life may be similar. Finally, as with all research, we interviewed individuals who agreed to participate, and this group of participants may be self-selected to have more interest in discussing our research questions.
In conclusion, our study found that, while Type 2 SLE symptoms occur almost invariably during the course of SLE, these symptoms exist as two distinct patterns: intermittent and in synchrony with Type 1 inflammatory symptoms, or persistent despite remission of Type 1 symptoms. Future studies need to focus on identifying biological, immunological and psychosocial differences between patients with Intermittent and Persistent Type 2 SLE.
This study emphasises the importance of engaging patients in qualitative research through which they can provide a personal account of their experiences living with chronic diseases. A key strength of this paper is the use of the qualitative approach of episode profile analysis. Through this process, we were able to consider and understand the experiences of each patient and then group similar experiences together. This new approach allowed us to find homogeneity within a heterogeneous disease. Only by listening to the stories of our patients were we able to find the two underlying patterns of Type 2 SLE.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Duke Health IRB (Pro00102300, Pro00103335).
Acknowledgments
We thank the participants for their involvement in the study.
References
Footnotes
Twitter @MithuRheum
Contributors All authors contributed to the interpretation of the data, drafting of the article and/or revising the manuscript critically for important intellectual content. All authors approved the final version to be published. AME, JLR, AC, DSP and MEBC contributed to the conception or design of the work. JLR, LGC-S, JD, RES, KS and MEBC contributed to the acquisition of clinical data. AME, JLR, AC, KM, MM and MEBC contributed to the acquisition and analysis of qualitative data. AME is responsible for the overall content of the study as guarantor.
Funding This work was supported by grants from the NIH NCATS (1KL2TR002554) and Pfizer (ASPIRE Award). AME and KS are supported by a grant from the NIH NCATS (1KL2TR002554). KS is supported by a grant from the Duke Center for REsearch to AdvanCe Healthcare Equity (REACH Equity) Career Development Award (NIH 5U54MD012530-02). LGC-S is supported by grants from the Rheumatology Research Foundation and the Arthritis Foundation.
Competing interests AME reports grant support from Exagen to her institution outside the submitted work. JLR reports grant support from Exagen to her institution outside the submitted work; consulting fees from Eli Lilly, Immunovant and Exagen. AC reports grant support from UCB to her institution outside the submitted work. DSP reports consulting fees from Immunovant and participation on a Data Safety Monitoring Board or Advisory Board for Bristol Myers Squibb. LGC-S reports grant support from GlaxoSmithKline to her institution outside the submitted work; honorarium from Pennsylvania State University and the American College of Rheumatology. JD reports grant support from Pfizer outside the submitted work. MEBC reports grant support from Exagen, UCB and GlaxoSmithKline to her institution outside the submitted work; consulting fees from UCB, AstraZeneca and GlaxoSmithKline outside the submitted work. KM, MM and RES have no relevant competing interests to declare.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.