Article Text

Abstract
Objective To evaluate the risk of major infections and the relationship between major infections and mortality in patients with newly diagnosed SLE.
Methods A newly diagnosed (<3 months) hospitalised Systemic Lupus Inception Cohort (hSLIC) in our centre during 1 January 2013 and 1 November 2020 was established. All patients were followed up for at least 1 year or until death. Patient baseline characteristics were collected. Major infection events were recorded during follow-up, which were defined as microbiological/clinical-based diagnosis treated with intravenous antimicrobials. The cohort was further divided into a training set and a testing set. Independent predictors of major infections were identified using multivariable logistic regression analysis. Kaplan-Meier survival analyses were conducted.
Results Among the 494 patients enrolled in the hSLIC cohort, there were 69 documented episodes of major infections during the first year of follow-up in 67 (14%) patients. The major infection events predominantly occurred within the first 4 months since enrolment (94%, 65/69) and were associated with all-cause mortality. After adjustments for glucocorticoid and immunosuppressant exposure, a prediction model based on SLE Disease Activity Index >10, peripheral lymphocyte count <0.8×109/L and serum creatinine >104 µmol/L was established to identify patients at low risk (3%–5%) or high risk (37%–39%) of major infections within the first 4 months.
Conclusions Newly onset active SLE is susceptible to major infections, which is probably due to underlying profound immune disturbance. Identifying high-risk patients using an appropriate prediction tool might lead to better tailored management and better outcome.
- systemic lupus erythematosus
- outcome assessment, health care
- therapeutics
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Major infections in SLE contribute to early death.
Short disease duration (<1 year) is an independent risk factor for infections in patients with SLE.
WHAT THIS STUDY ADDS
Major infection events were documented in 14% of patients in a newly diagnosed hospitalised SLE inception cohort during the first year of follow-up.
The majority (94%) of major infections occurred within the first 4 months and was associated with all-cause mortality.
A simple model based on SLE Disease Activity Index >10, peripheral lymphocyte count <0.8×109/L and serum creatinine >104 µmol/L were identified for predicting major infections in newly diagnosed SLE.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Underlying profound immune disturbance is probably the reason that makes newly onset active SLE susceptible to major infections.
Using appropriate prediction tool to identify high-risk patients might lead to better tailored management and better outcome.
Introduction
SLE is a chronic multisystemic autoimmune disease associated with significant morbidity and mortality. A bimodal pattern of death has been well-conceived, that is, early deaths (<1 year) are most often due to active SLE or infection; while late deaths are mainly related to atherosclerotic vascular disease.1 Indeed, short disease duration (<1 year) has been shown to be an independent risk factor associated with infections in different SLE cohorts.2–4 In patients with SLE, infections are largely considered a complication of immunosuppressive therapy; however, as high as 25.9% of severe infections are reported at the time of SLE diagnosis in the absence of immunosuppressive therapy.5 The high prevalence of severe infection in newly diagnosed SLE implies that infections are attributable to glucocorticoid and immunosuppressive therapy, and may be related to the underlying immune disturbance of SLE itself.
A recent Canadian population-based study showed that the incidence of serious infections and infection-related mortality increased by 82% and 61%, respectively, in patients with newly diagnosed SLE compared with a matched non-SLE population.6 In a Spanish inception cohort of 282 patients with newly diagnosed SLE, 19 patients (6.4%) had major infections during the first year of follow-up; high baseline SLE activity and prednisolone dose >30 mg/day during the first month were associated with a higher risk of infections.7 However, there is still no reliable method with which to precisely predict infection risk in patients with newly diagnosed SLE.
Here, by using an observational inception cohort of Chinese patients with newly diagnosed SLE (<3 months) from our centre, we aimed to profile major infection events within the first year of follow-up, and to develop a risk assessment tool for infection prediction.
Methods
Patient population and study design
Since January 2013, hospitalised patients with newly diagnosed SLE (<3 months) in the Rheumatology Department of Renji Hospital have been included in the hospitalised Systemic Lupus Inception Cohort (hSLIC). The hospitalisation was a shared decision-making by the treating physicians and the patients. The judgement of admission was based on disease activity, severity (complications included) and the need for extensive evaluation, such as invasive procedures (eg, renal biopsy).
All patients fulfilled the 1997 American College of Rheumatology (ACR) and/or 2019 European Alliance of Associations for Rheumatology/ACR SLE classification criteria.8 9 All patients who underwent at least 12 months of follow-up or until death were included in this longitudinal observational study. The cohort was further divided into a training dataset of patients enrolled between 1 January 2013 and 31 December 2019, and a testing dataset of those enrolled between 1 January 2020 and 1 November 2020.
Baseline data at the time of enrolment (at the beginning of hospitalisation) were recorded, including demographic information, clinical manifestations, laboratory tests and SLE Disease Activity Index (SLEDAI).10 Infections were graded according to Common Terminology Criteria for Adverse Events (CTCAE) (https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_ Reference_5×7.pdf). Major infection was defined as microbiological/clinical-based diagnosis treated with intravenous antimicrobial,11 which had a CTCAE grade 3 or higher. A definitive diagnosis was established if an organism was isolated from sterile sites in a patient with consistent clinical manifestations. A clinical diagnosis was established when combined clinical, laboratory and imaging findings were consistent with an invasive infection, with or without findings of colonisation.12
Statistical analysis
The independent-sample Student’s t-test, Mann-Whitney U test and χ2 test were applied as appropriate. Optimal cut-off values for continuous variables, such as SLEDAI score and age, were determined by receiver operating characteristic curve analysis (online supplemental figure S1). The independent predictors of major infection within the first 4 months were determined by multivariate logistic stepwise regression with or without adjustment for treatment exposure. Independent predictors were then combined to establish a prediction model. The performance of the prediction model was examined by Kaplan-Meier plot and receiver operating characteristic curve analysis.
Supplemental material
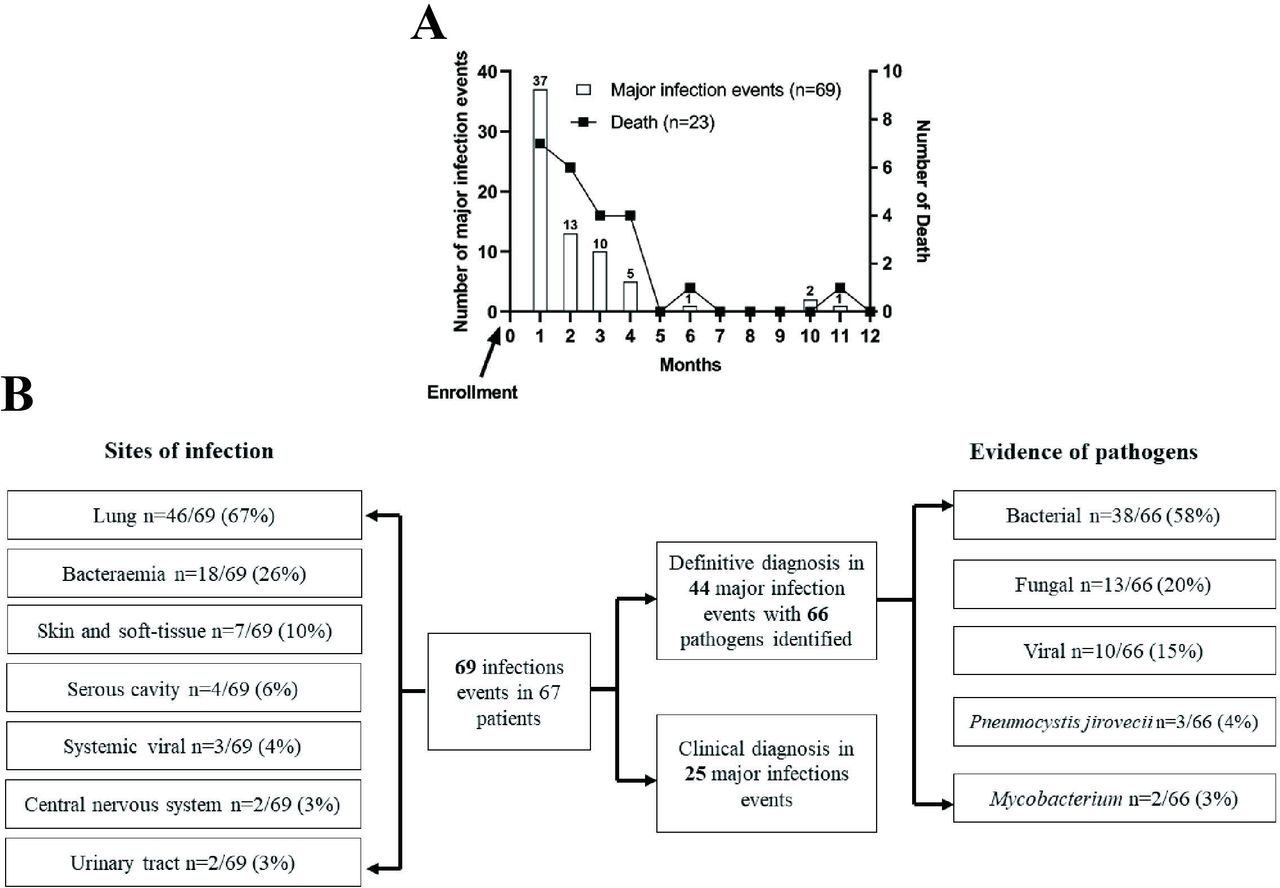
Pattern and profile of major infections in hospitalised Systemic Lupus Inception Cohort. (A) Sixty-nine documented major infection events were recorded in 67 patients during the first year of follow-up. Death events were also presented. (B) Major infection profiling.
All statistical analyses were performed using SPSS V.23 (Armonk, New York, USA) or GraphPad V.5.0 (San Diego, California, USA) software. Statistical significance was defined as p<0.05.
Results
Major infections were related to mortality in hSLIC
Between January 2013 and November 2020, a total of 553 patients with newly diagnosed SLE were hospitalised in our centre. Of those, 59 patients were excluded for not completing 1-year follow-up. A total of 494 eligible patients were included in the hSLIC study with a mean follow-up time of 2.8±2.0 years. There were 432 women (87%), with a mean age at enrolment of 36±14 years and median (IQR) duration from diagnosis to admission of 9 (1, 22) days. The cohort included 27 adolescent (aged <18 years, 5.5%) with a median age of 15 (14, 17) years. The mean SLEDAI score at enrolment was 11±6. In addition, none of our patients had HIV or primary immunodeficiencies. The clinical characteristics of the cohort are presented in table 1.
Baseline features of the hospitalised Systemic Lupus Inception Cohort
Overall, 29 patients died within the first year of follow-up, yielding a 1-year all-cause crude mortality of 5.9%. The results of the univariable comparison of baseline characteristics between survivors and deceased patients are summarised in table 1. Compared with survivors, deceased patients were older, had a higher SLEDAI score and had higher incidences of major infections, pulmonary hypertension, serositis, exposure to glucocorticoids (before study enrolment), cytopenia and renal insufficiency. Among 52/494 (11%) patients with a baseline serum creatinine >104 µmol/L, 10/52 (19%) were on dialysis; 9 patients ended up with end-stage renal disease during follow-up.
In the final multivariable logistic regression model, the independent predictors of 1-year all-cause mortality in hospitalised patients with newly diagnosed SLE were age at admission (OR=1.058, 95% CI 1.026 to 1.092) and major infections (OR=22.083, 95% CI 6.752 to 72.228) (online supplemental table S1).
Characteristics of major infections
During the first year of follow-up, 69 documented episodes of major infections were recorded in 67/494 (14%) patients. Two patients had more than one infection event, and 22/67 (33%) patients died from conditions related to the infection event. Of note, 65/69 (94%) of the infection events occurred within the first 4 months after enrolment (figure 1A).
The most common infection was pneumonia (46/69; 67%), followed by bacteraemia (18/69; 26%), skin and soft-tissue infections (7/69; 10%) and serous cavity infections (4/69; 6%); central nervous system infections (3%) and urinary tract infections (3%) were less common. Infections at multiple sites were seen in 13/69 (19%) patients, most of whom (9/13) had bacteraemia accompanied by pneumonia. The detected organisms were bacteria (58%), fungi (20%), viruses (15%), Pneumocystis jirovecii (4%) and Mycobacterium tuberculosis (3%) (figure 1B). The detailed microbiological findings are shown in online supplemental table S2.
Predictors for major infection within 4 months
Then, the cohort was further divided into a training dataset and a testing dataset based on time of enrolment. With similar baseline features in the two datasets, disease characteristics of patients with major infections within the first 4 months were compared with the rest of the patients in each dataset (table 2). Of these, 49/352 (14%) patients in the training set and 14/142 (10%) patients in the testing set had major infections within the first 4 months, respectively. Univariate and subsequent multivariable logistic regression analyses were used to identify candidate predictors in the training set. The multivariable logistic regression model included the following 10 clinically meaningful candidate predictors in the training dataset: age >40 years, SLEDAI >10, gastrointestinal involvement, nephritis, lymphocyte count <0.8×109/L, platelet count <100×109/L, serum creatinine >104 µmol/L and use of glucocorticoids, hydroxychloroquine and immunosuppressants before enrolment. Finally, three independent risk factors for major infections within 4 months were identified: SLEDAI >10 (OR=3.28, 95% CI 1.26 to 8.57), lymphocyte count <0.8×109/L (OR=4.18, 95% CI 1.90 to 9.17) and serum creatinine >104 µmol/L (OR=7.16, 95% CI 2.82 to 18.17) (table 3). As previous research shows that the administration of glucocorticoids within the first month is associated with subsequent infections in patients with newly diagnosed SLE,7 we further adjusted for methylprednisolone pulse therapy (≥500 mg/day intravenously for 3 days) and cumulative prednisone equivalent dosages within 1 month of enrolment. The aforementioned three risk factors for major infections remained significant after these adjustments, indicating the robustness of the results (online supplemental table S3).
Baseline comparison of patients with or without major infections in the first 4 months
Multivariate logistic regression of risk factors for major infections in the training set
Risk prediction model for major infection within 4 months
We generated a predictive model combining the three independent risk factors for major infections within 4 months. Risk score was defined as the number of risk factors present. The incidences of major infection events for patients in the training set with risk scores of 0, 1, 2 and 3 were 1.5%, 9.0%, 31.0% and 72.2%, respectively. We then categorised patients into two groups: low risk (risk score ≤1) and high risk (risk score ≥2) (figure 2A). The Kaplan-Meier plots display the probability of major infections within 4 months in the low-risk and high-risk groups (figure 2B). The performance of the risk model in predicting major infections was supported by a C-Index of 0.83 (95% CI 0.78 to 0.89) and 0.84 (95% CI 0.75 to 0.93) in the training and testing datasets, respectively.

{kind=link}
{kind=link}
A model for predicting major infection within 4 months in newly diagnosed SLE. (A) The risk score was defined as the number of risk factors (SLE Disease Activity Index >10, lymphocyte count <0.8×109/L and serum creatinine >104 µmol/L). Infection risk (green=low risk, red=high risk) based on the risk score in the training set and testing set. (B) Major infection-free survival curves were determined by Kaplan-Meier analysis.
Discussion
The present study found a high incidence of major infections (14%) during the first year of follow-up in hospitalised patients with newly diagnosed SLE. Of note, 94% of major infection events occurred in the first 4 months after enrolment, and major infection was related to all-cause mortality. To predict the occurrence of major infection within the first 4 months in this population, we developed a data-driven risk model composed of the SLEDAI score, blood lymphocyte count and serum creatinine measured at the beginning of hospitalisation. The result was robust across internal training and testing datasets. However, the model requires validation in independent large-scale studies.
To date, a few prediction models for infection in patients with SLE have been reported.13 For instance, a model composed of albumin, creatinine levels and daily dose of prednisolone, has been established for predicting severe infection within 6 months among hospitalised patients with active SLE.14 Another retrospective study developed an algorithm (SLE Severe Infection Score (SLESIS)) to predict the risk of severe infections in patients with SLE15; the SLESIS incorporates age, sex, Latin American ethnicity, Katz Index (Lupus Severity of Disease Index),16 previous hospitalisations for SLE, previous severe infection and daily dose of prednisolone ≥10 mg/day.15 Only one study created a model using a prospective cohort of patients with lupus with a disease duration of <5 years17; a composite clinical-immunological index including use of cyclophosphamide, absolute number of B cells, total T helper 17 lymphocytes and expression of toll-like receptor 2 in monocytes was generated to predict the development of infection in patients with SLE. Our study, on the other hand, was focused on a more homogenous hospitalised population with newly diagnosed SLE without long-term treatment exposure or chronic damage accrual. The model is simple and straightforward.
It is well known that both disease activity and immunosuppressive therapy contribute to an increased incidence of infections in SLE.2 18–20 However, in our hSLIC population, SLE disease activity index apparently outweighed glucocorticoid and immunosuppressant, which serves as a key factor predicting major infections. Our finding indicated that the predisposition to infection among newly diagnosed SLE is more likely attributed to the immune function impairment of SLE per se.21 Our study underscored the notion that major infection is a significant complication with a strong prognostic implication in the early phase (<4 months) of hospitalised patients with newly diagnosed SLE. Our risk prediction model might be helpful to sort out high-risk patients. Furthermore, the profile of major infections in our hSLIC revealed that the most common infection sites were lung, blood, skin and soft tissue. Likewise, bacterial, fungal and viral infections were the top three pathogens.22 23 Therefore, prompt recognition of infection and empirical antimicrobial treatment might be a logical strategy for high-risk patients. Appropriate vaccination (such as recombinant zoster vaccine for herpes zoster infection24) and antimicrobial prophylaxis (such as trimethoprim-sulfamethoxazole for P. jirovecii infection25) should be considered as important parts of the strategy to minimise the risk of major infections.
Our study had several limitations, of which the generalisability issue ought to be underscored. The results from our hSLIC cohort should not be extrapolated to all patients with newly diagnosed SLE, especially for those with relatively mild disease. In addition, with only 5% adolescent-onset SLE in the cohort, our conclusions should not be extrapolated to juvenile populations. It is a single-centre study without external validation. Moreover, the absence of vaccination status evaluation, particularly under the pressure of COVID-19 pandemic; and the lack of antibiotics prophylaxis protocol, which all should be placed in the future research agenda. Nevertheless, our data shed some light to better understand the pattern and risk factors of major infections in newly diagnosed severe SLE.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the ethics committee of Renji Hospital (IRB # 2012-42K). Written informed consent was obtained from all patients.
Acknowledgments
The authors thank all research nurses and patients who participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
HW and YZ are joint first authors.
Contributors SY, YC, NS and HW were involved in study concept and/or design; HW, YZ and LY were involved in acquisition of data; and WW, LZ, SG, FS and DZ contributed to analysis and/or interpretation of data. SY is the guarantor. All authors reviewed the final draft of the manuscript and approved it for submission.
Funding This study was funded by grants from the Shanghai Hospital Development Center (SHDC) (no. SHDC2020CR1015B and no. SHDC2020CR6026).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.