Article Text

Abstract
Objectives To evaluate the safety and immunogenicity of third and fourth BNT162b2 boosters in patients with SLE and rheumatoid arthritis (RA).
Methods Patients with SLE and RA aged 18–65 years who completed a series of inactivated, adenoviral vector, or heterogenous adenoviral vector/mRNA vaccines for at least 28 days were enrolled. Immunogenicity assessment was done before and day 15 after each booster vaccination. The third BNT162b2 booster was administered on day 1. Patients with suboptimal humoral response to the third booster dose (antireceptor-binding domain (RBD) IgG on day 15 <2360 BAU/mL) were given a fourth BNT162b2 booster on day 22.
Results Seventy-one patients with SLE and 29 patients with RA were enrolled. The third booster raised anti-RBD IgG by 15-fold, and patients with positive neutralising activity against the Omicron variant increased from 0% to 42%. Patients with positive cellular immune response also increased from 55% to 94%. High immunosuppressive load and initial inactivated vaccine were associated with lower anti-RBD IgG titre. Fifty-four patients had suboptimal humoral responses to the third booster and 28 received a fourth booster dose. Although anti-RBD IgG increased further by sevenfold, no significant change in neutralising activity against the Omicron variant was observed. There were two severe SLE flares that occurred shortly after the fourth booster dose.
Conclusions The third BNT162b2 booster significantly improved humoral and cellular immunogenicity in patients with SLE and RA. The benefit of a short-interval fourth booster in patients with suboptimal humoral response was unclear.
Trial registration number TCTR20211220004.
- COVID-19
- Lupus Erythematosus, Systemic
- Vaccination
Data availability statement
The data of this article are available upon reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The SARS-CoV-2 omicron variant (B.1.1.159) has multiple mutations that have resulted in greater escape from immune protection elicited by COVID-19 vaccines.
More attenuated immune response to SARS-CoV-2 vaccination has been observed in patients with autoimmune rheumatic diseases. The additional third dose of SARS-CoV-2 vaccine has been recommended in immunocompromised populations.
Some immunocompromised patients have a suboptimal humoral response to a third booster dose. Factors associated with poor immune response have not been adequately studied.
Administration of more than three doses has been shown to enhance immune response in some severely immunocompromised patients.
WHAT THIS STUDY ADDS
The third BNT162b2 booster was well tolerated, and significantly improved both humoral and cellular immunogenicity in patients with SLE and RA previously vaccinated with either inactivated, adenoviral vector, or heterogenous adenoviral vector/mRNA vaccines.
High intensity of immunosuppressive therapy and initial inactivated vaccine were associated with lower humoral immune response to the third BNT162b2 booster.
Short interval administration of a fourth BNT162b2 booster in poor humoral immune responders may not offer additional protection against the omicron variant, and flares were observed in patients with SLE.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study supported a third BNT162b2 booster dose administration in patients with SLE and RA to enhance immune protection against the Omicron variant.
Patients who receive a high dose of immunosuppressive therapy or initial inactivated vaccine could be unprotected from SARS-CoV-2 infection. Benefits and risks of additional boosters or second generation of SARS-CoV-2 vaccine should be further studied.
Introduction
The newly emerged B.1.1.159 (Omicron) variant of SARS-CoV-2 has become the dominant strain globally. Its multiple mutations have resulted in greater escape from immune protection elicited by COVID-19 vaccines.1 Recent studies in healthy populations suggested that the third booster dose of mRNA vaccine enhanced protection against the Omicron variant, although neutralising antibody titres were reduced by sevenfold compared with the ancestral variant.2–4
In patients with autoimmune rheumatic diseases, a more attenuated immune response to SARS-CoV-2 vaccination has been observed.5 According to a recent study, a third dose of mRNA 1273 vaccine significantly increased antireceptor-binding domain (RBD) titre in transplant recipients compared with placebo. However, in approximately half of the patients who received a booster, the anti-RBD titre remained low (<100 U/mL).6 Clinical factors associated with the immunogenicity in immunosuppressed populations have not been adequately studied. Several booster doses may be required to achieve adequate immune protection.7 The safety and risk of disease flare associated with repetitive vaccination in patients with autoimmune rheumatic diseases remain unknown.
We aimed to evaluate safety and immunogenicity of the third and fourth BNT162b2 booster doses in patients with SLE and rheumatoid arthritis (RA) previously vaccinated with either adenoviral vector, inactivated or heterogenous adenoviral vector/mRNA regimens. Factors associated with humoral immune response after the third booster dose were also evaluated.
Methods
Trial design
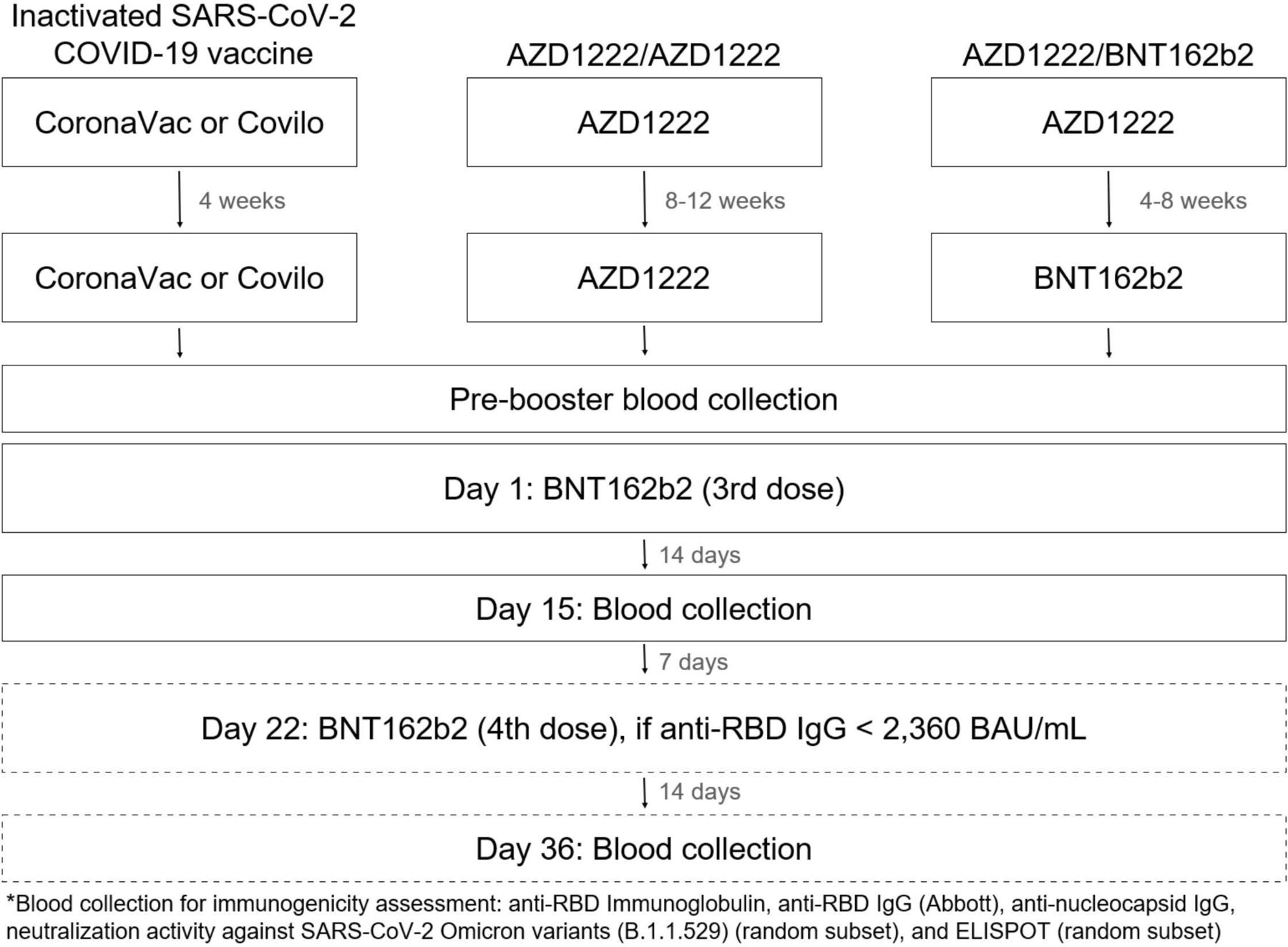
This is a prospective, single arm, open-labelled study investigating the safety and immunogenicity of third and fourth mRNA vaccine (BNT162b2, Pfizer–BioNTech) booster doses in patients with SLE and RA who have previously been vaccinated with inactivated SARS-CoV-2 COVID-19 vaccine (CoronaVac or COVILO), adenovirus-vectored vaccine (AZD1222, AstraZeneca) or heterologous regimen of AZD1222/BNT162b2.
Participants
Eligible patients were aged 18–65 years who met the classification criteria for SLE (American College of Rheumatology (ACR) 19978 or the Systemic Lupus International Collaborating Clinics criteria9 or European League Against Rheumatism (EULAR)/ACR classification10 or RA (2010 ACR and EULAR classification criteria for RA11 and had completed a series of inactivated vaccine (CoronaVac or COVILO), AZD1222 or AZD1222/BNT162b2 for at least 28 days. Intervals between the first and second doses of COVID-19 vaccines were stipulated by vaccine types: 4 weeks for inactivated vaccine, 8–12 weeks for AZD1222/AZD1222 and 4–8 weeks for AZD1222/BNT162b2. Exclusion criteria were history of SARS-CoV-2 infection, allergy to a vaccine component, pregnancy, breastfeeding and active disease at enrolment. Recruitment occurred at the rheumatology and nephrology clinic in a tertiary referral centre in Bangkok, Thailand, from 1 August 2021 to 30 November 2021. Consecutive patients meeting eligibility criteria were invited to participate in the study and provided written informed consent.
Procedures
At baseline, demographic information, current medications, disease activity and blood samples for immunogenicity analyses were collected. On day 1, 30 μg of BNT162b2 was administered intramuscularly via the deltoid region. On day 15, blood samples were collected in order to assess immune responses at their peak.12 On day 22, those with suboptimal humoral response, defined as anti-RBD IgG less than 2360 BAU/mL (16 503 AU/mL) after the third booster, were given the fourth BNT162b2 booster at 30 μg. Blood sample collection for immune responses assessment was performed again on day 36 (figure 1).

Schematic diagram of the study. BAU, binding antibody unit; RBD, receptor-binding domain.
We chose the anti-RBD IgG (Abbott Diagnostics, Abbott Park, Illinois, USA) cut-off value of 2360 BAU/mL (16 503 AU/mL) as it corresponded to vaccine efficacy of 90% for wild type.13 We aimed for high vaccine efficacy due to the spread of vaccine-resistant variants including Delta (B.1.617.2) and Omicron (B.1.1.529) variants.
Immunogenicity assessment
The humoral responses were measured by serum binding IgG levels against RBD of the SARS-CoV-2 spike protein using the SARS-CoV-2 IgG II Quant assay (Abbott Diagnostics). Values of 50 arbitrary U/mL (AU/mL) were considered positive. The numerical AU/mL is converted to binding antibody unit (BAU) per millilitre (BAU/mL) by multiplying it by 0.142. The SARS-CoV-2 cPassTM surrogate virus-neutralising test (GenScript, Piscataway, New Jersey, USA) was used to evaluate the neutralising activity against the SARS-CoV-2 Omicron variant in a subset of prebooster and postbooster samples. According to the manufacturer’s recommendations, inhibition levels greater than 30% were considered positive. The SARS-CoV-2 IgG assay (Abbott Diagnostics) was used to quantify the nucleocapsid protein of SARS-CoV-2 to evaluate for recent SARS-CoV-2 infection. Positive values were defined as 1.4. The cellular immune responses were measured by human IFN-γ-ELISpot assay (ELISpot) in a random subset of patients. Positive responses were defined as >50 spots per 10⁶ peripheral blood mononuclear cells.
Immunosuppressive treatments
Due to various immunosuppressive treatment regimens used in our cohort and more than half of patients taking two or more immunosuppressive medications, we adopted and modified the Vasudev score14 to standardise the overall immunosuppressive load. One unit of immunosuppression was assigned for each of the following doses of immunosuppressive medications: prednisone 5 mg/day, mycophenolate mofetil (MMF) 500 mg/day, azathioprine 100 mg/day, cyclosporine 100 mg/day, tacrolimus 2 mg/day, leflunomide 10 mg/day and methotrexate 15 mg/week (table 1). The average dose of immunosuppressive medication during the first 30 days was used for immunosuppressive unit scale calculation. Adjustment of immunosuppressive medications during such periods was not allowed unless clinically indicated.
Immunosuppressive load calculation scale modified from Vasudev score (9)
Safety and reactogenicity assessment
Thanou modified SELENA-SLEDAI (Safety of Estrogens in Lupus Erythematosus: National Assessment– Systemic Lupus Erythematosus Disease Activity Index) Flare Index was used to determine SLE flares. Disease activity of patients with RA was measured by Disease Activity Score 28 ESR in a subset of patients. The local and systemic reactogenicities were reviewed on day 15 and reviewed again on day 36 in those who received the second booster.
Statistical analyses
Continuous variables were expressed as mean (SD) or mean (95% CI). Antibody levels were presented as geometric mean titre (GMT) with 95% CI, or median with range when appropriate. Geometric means were computed by natural log transformation of the data points and calculating the mean and 95% CI on the transformed data. The ln-transformed mean and 95% CI were transformed back to the original scale.
Student’s t-test was used to compare the differences between two groups. Multiple groups were compared using one-way analysis of variance, followed by the Bonferroni post hoc test. Pearson or Spearman’s correlation was used to test for associations between two variables.
Univariable and multivariable linear regression was performed to determine the relationship between clinical factors and immune responses after the third booster dose. A p value of <0.05 was considered statistically significant. Statistical analysis was performed using JMP software V.13.2.1 (SAS Institute, Cary, North Carolina, USA), and dot-plot graphs were created using GraphPad Prism V.4.03 (GraphPad Software, La Jolla, California, USA).
Results
One hundred patients were enrolled with 71 having SLE and 29 having RA. All of the patients had stable disease. Ninety three per cent of patients were women. The majority of patients with SLE received MMF, and the majority of patients with RA received methotrexate (table 2).
Demographics and clinical characteristics of the study participants
Because ADZ1222 was primarily administered to the elderly in Thailand, it was given to slightly over half of the patients with RA (51.7%) who tended to be relatively older. Vaccine administration was more equally divided among patients with SLE with 38% receiving inactivated vaccines, 36.6% receiving ADZ1222/ADZ1222% and 25.4% receiving AZD1222/BNT162b2. The inactivated vaccine had the longest interval between the second and third booster doses because it was the first vaccine series available in Thailand (table 2).
Humoral immune responses following the third and fourth BNT162b2 booster doses
Anti-RBD IgG
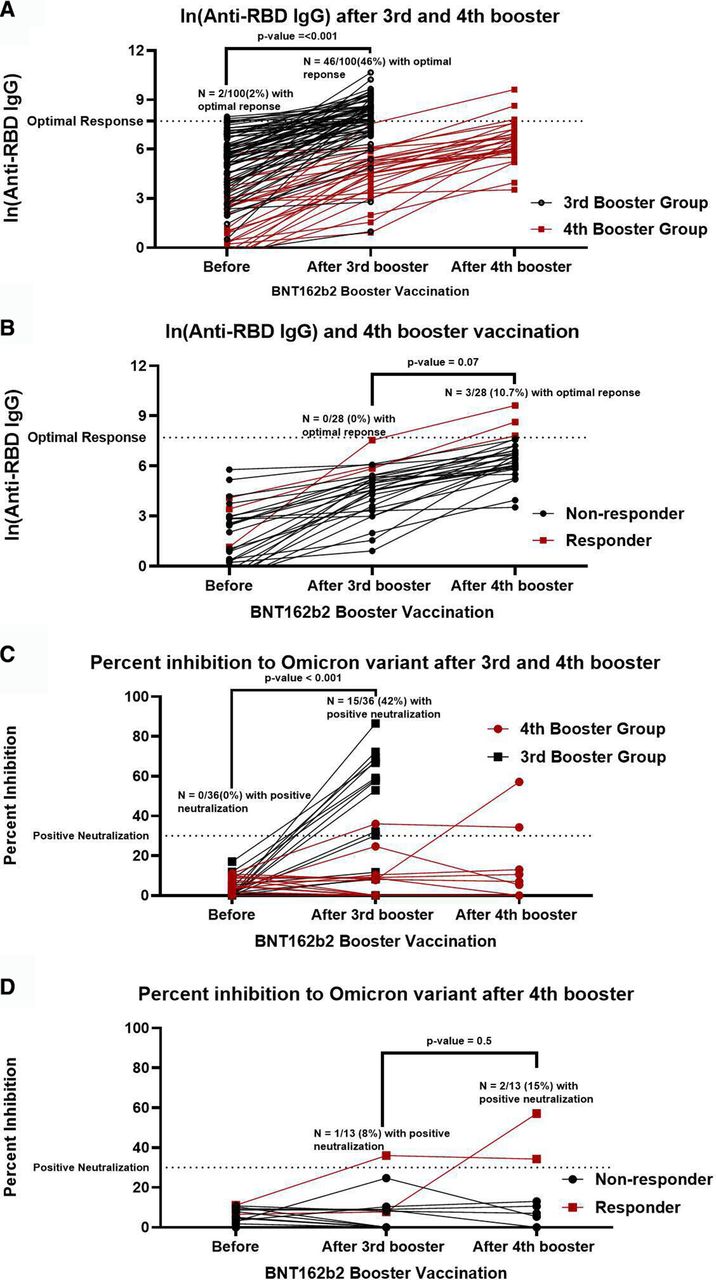
Antinucleocapsid antibodies were undetectable in all prebooster and postbooster serum samples, indicating that no COVID-19 infection occurred during the peribooster period. After the third booster, the GMT of anti-RBD IgG increased by 15-fold (from 69 (95% CI 42 to 112) BAU/mL to 1034 BAU/mL (95% CI 677 to 1577), p<0.0001) (figure 2A). Patients with anti-RBD IgG levels of more than 2360 BAU/mL increased from 2% to 46% (p<0.0001)
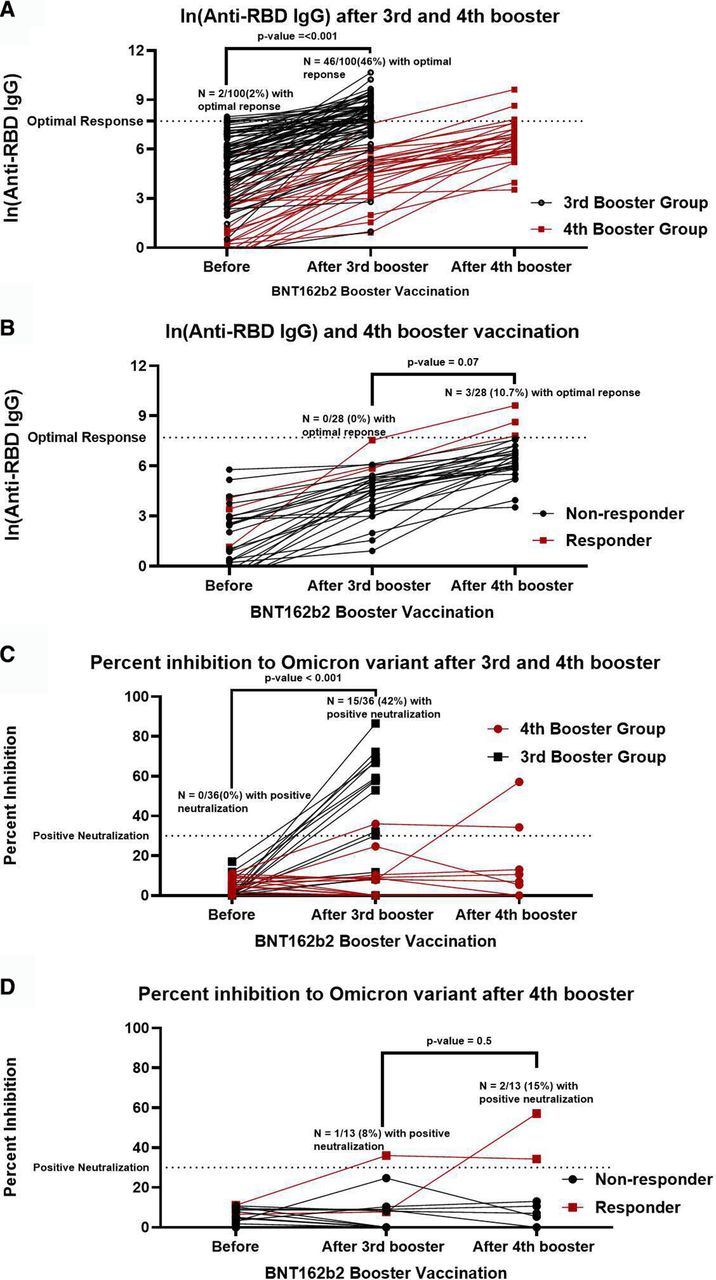
Humoral immune response before and after the third and fourth BNT162b2 booster. Optimal humoral response defined as anti-RBD IgG more than 2360 BAU/mL (16 503 AU/mL) after the third booster. BAU, binding antibody unit; RBD, receptor-binding domain.
Of 54 patients (39 with SLE and 15 with RA) with suboptimal responses to the third booster vaccine (anti-RBD IgG titre <2360 BAU/mL on day 15), 28 (23 with SLE and 5 with RA) received the fourth BNT162b2 booster on day 22. The remaining patients refused to have another booster dose. The GMT of anti-RBD Ig increased by sevenfold after the fourth booster (88 BAU/mL (range 49–155) to 644 BAU/mL (range 398–1041), p<0.0001), and three patients (11%) had anti-RBD IgG of >2360 BAU/mL (figure 2B).
Neutralising activity against omicron variant
We randomly selected 12 patients with SLE from each initial vaccine group (inactivated SARs-CoV2 vaccine, AZD1222/AZD1222 and AZD1222/BNT162b2) to assess for neutralising activity against the Omicron variant (n=36). The level of anti-RBD IgG corresponded with the neutralising activity (r2=0.42, p<0.0001).
Before receiving a third booster dose, none of the patients demonstrated positive neutralising activity against the Omicron variant. After the third booster dose, 15 patients (42%) had positive neutralising activity (>30% inhibition), and the mean percent inhibition increased from 5.1% (95% CI 3.3% to 6.8%) to 28.0% (95% CI 17.7% to 38.4%) (p<0.0001) (figure 2C).
Of 36 patients, 13 were subsequently given the fourth booster dose according to the protocol. The neutralising activity after the third and fourth booster doses was not statistically different (p=0.7). There were only 1 (7.7%) and 2 (15.4%) of the 13 patients who demonstrated positive neutralising activity against the Omicron variant after the third and fourth booster doses, respectively (figure 2D).
Factors associated with humoral immune response
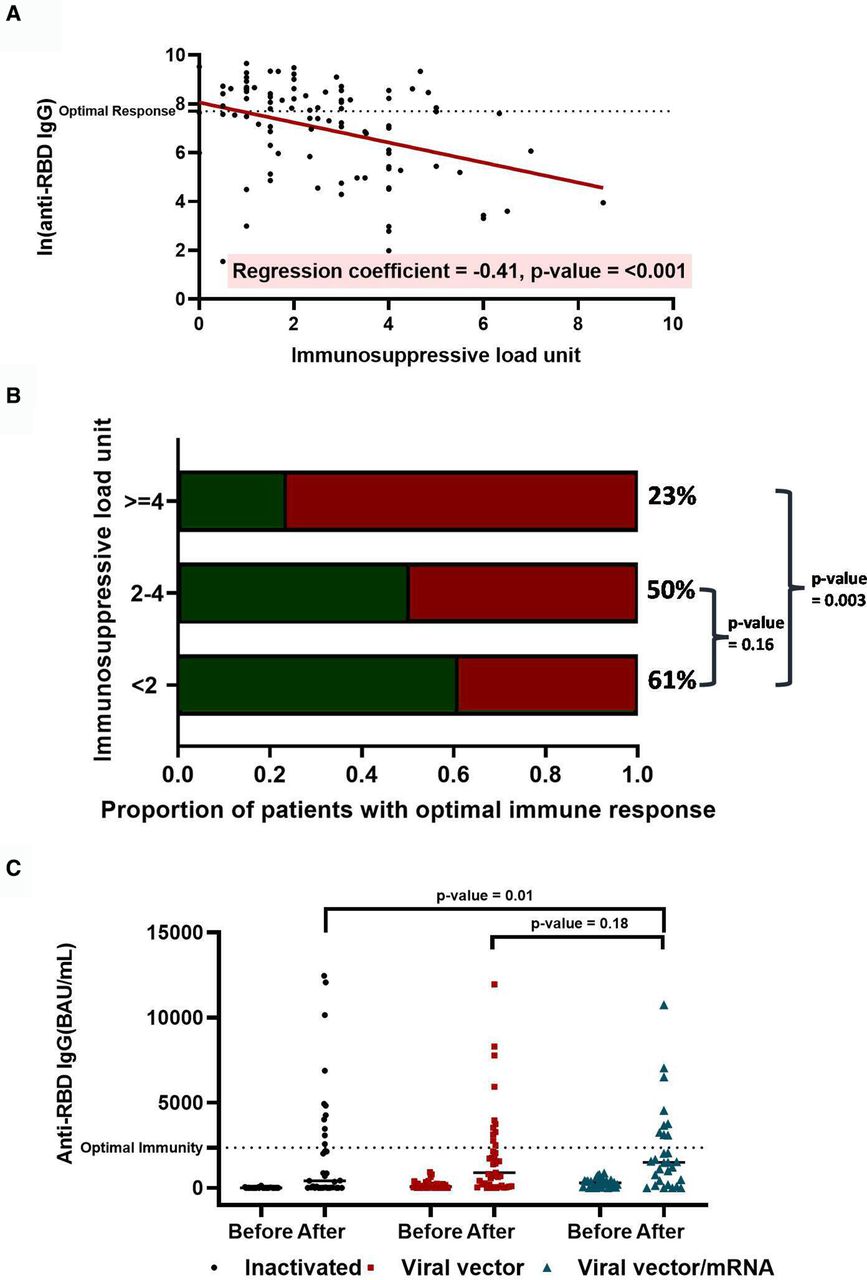
The initial inactivated vaccine and high immunosuppressive load were associated with low anti-RBD IgG titre, even adjusting for other covariates including age, sex, diagnosis and vaccine interval between the second and the third booster doses (table 3). Figure 3A–C illustrates the relationship between total immunosuppressive load and type of initial vaccine with anti-RBD IgG levels.
Association between clinical factors and ln(anti-RBD IgG) at day 15 following a third BNT162b2 booster in patients with SLE and RA
{kind=link}
{kind=link}
{kind=link}
(A) Relationship between total immunosuppressive load and anti-RBD IgG level after the third booster dose. (B) Proportion of patients with SARS-CoV-2 antispike RBD IgG antibody >2360 BAU/mL by immunosuppressive load (0 to <2, 2 to <4 and 4 or more). (C) SARS-CoV-2 antispike RBD IgG antibody before and after the third BNT162b2 booster dose by initial vaccine types. BAU, binding antibody unit; RBD, receptor-binding domain.
Cellular immune responses following the third BNT162b2 booster
The cellular immune response of 47 randomly selected patients was assessed before and 14 days after the third booster dose. Twenty-one, 15 and 11 patients received inactivated vaccines, AZD1222/AZD1222 and AZD1222/BNT162b2 as initial vaccines, respectively. Thirty-four patients (72%) had SLE and the rest had RA.
After a third booster, the proportion of individuals who had a positive ELISpot test increased from 55% to 94%. Before a third booster, those who initially received inactivated vaccines had the lowest rate of positive ELISpot test (31%), followed by AZD1222/AZD1222 (67%) and AZD1222/BNT162b2 (73%) (p=0.05), which increased to 90%, 93% and 100% after the third booster (p=0.4). There was no significant correlation between ELISpot and anti-RBD IgG level after booster (r(45)=0.22, p=0.14).
Safety, reactogenicity and disease activity of BNT162b2 booster
There was no COVID-19 breakthrough infection up to 90 days following the third booster vaccination. The BNT162b2 boosters were well tolerated, and all reactions were mild and transient. The three most common reactions were injection site pain, fatigue and fever (online supplemental figure 3). Anti-RBD IgG levels did not differ between those without adverse reactions and those who had at least one reaction (p=0.4).
Supplemental material
Two patients with SLE (8.7%) experienced disease flare after the fourth booster dose. One patient developed rapidly progressive glomerulonephritis from lupus nephritis 1 week after receiving the fourth booster vaccine. MMF also had been withheld a few months before the booster administration due to a history of multiple infections. The other developed severe thrombocytopenia 4 weeks after receiving a booster dose. The patient’s disease had been inactive for several years and she had not been receiving immunosuppressive treatment prior to this episode of flare.
Discussion
As the Omicron variant continues to spread around the world and display increased immune escape potential, aggregating data to optimise immunisation strategies in autoimmune rheumatic disease populations is crucial. This study found that a third booster dose of BNT162b2 in patients with SLE and RA was well tolerated and elicited a strong humoral immune response against the Omicron variant. However, approximately half of our patients still had a poor response to the third BNT162b2 booster, particularly those who received more intense immunosuppressive treatment or an inactivated vaccine in the initial vaccine series.
By giving a fourth BNT162b2 booster to poor immune responders, anti-RBD IgG increased to a lesser extent compared with the third booster dose (7-fold vs 15 fold), possibly due to the short interval between the third and fourth boosters.15 Despite the increase of anti-RBD IgG, no discernible increase in neutralising activity against the Omicron variant was observed. In addition, 8.7% of patients with SLE experienced severe flares shortly after the fourth booster dose, whereas other studies found mostly mild to moderate SLE flares (0% to 10.4%) after the initial vaccine series.16–19 In an animal model, repeated exposure to the same antigen was shown to induce autoimmunity.20 Given this uncertainty, the benefit of administering a short interval fourth booster dose should be balanced against the risk of disease activation.
In terms of cellular immunity, a third BNT162b2 booster elicited T-cell responses in nearly all of our patients. Positive cellular immune response rates were comparable across initial vaccine types, even among those who received inactivated vaccines, which are known to induce lower T-cell response.21 Recent studies have demonstrated that while variants of concern can evade neutralising antibodies, the cell-mediated immune response cross-reacted with the variants of concern.22–25 It also confers resilient protection against severe disease as antibody titres wane overtime.26
Prior to the booster vaccination, only 2% of patients in our cohort had antibody levels above the target of 2360 BAU/mL. This could be due to the study’s timing of antibody measurement and high target antibody level. Prebooster anti-RBD IgG was measured at day 65 (95% CI 59 to 70) after the second vaccination. As a result, antibodies may decay by half at the time of measurement.27 Due to the spread of vaccine-resistant RBD, we also aimed for a high anti-RBD IgG cut-off value, which corresponded to vaccine efficacy of 90% for wild type.13
It should be noted that there were several limitations to this study. The findings are observational and based on a small sample size, so they should be interpreted with caution. The results may not be generalisable to other autoimmune rheumatic conditions, other immunosuppressive regimens such as B-cell depletion therapy or initial mRNA vaccine series. The immunosuppressive load calculation was adapted from the prior study which was arbitrarily determined.
In conclusion, this study demonstrated that the third BNT162b2 booster was well tolerated and significantly improved humoral and cellular immunogenicity in patients with SLE and RA. The intensity of immunosuppressive therapy and the type of initial vaccine appear to affect the humoral immune response to the third booster. In poor humoral responders, a fourth BNT162b2 booster administered at a short interval may not provide additional protection against the omicron variant. Our finding that severe flares were observed in patients with SLE after the fourth booster is also cause for caution and additional research on the appropriateness of a fourth booster and the timing of such booster in our population.
Data availability statement
The data of this article are available upon reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the institutional review board of the Faculty of Medicine, Chulalongkorn University (COA No. 1425/2021). The participants gave informed consent to participate in the study before taking part.
Acknowledgments
BNT162b2 (lot number 30125BA) used in this study was supplied by the Department of Disease Control, Ministry of Public health with support of Dr Wisit Prasitsirikul, Deputy director of Bamrasnaradura Infectious Disease Institute. The authors thank Mahachakri Sirindhorn Clinical Research Center, Faculty of Medicine, Chulalongkorn University, for facility support, and Ms Jariya Pongsaisopon and Sukanlaya Yoosomsuk for coordinating the study. Thanks are also due to Dr Supranee Buranapraditkun and Dr Sasiwimol Ubolyam for enzyme-linked immunosorbent spot testing, and Ms Sutthinee Lapchai for sample preparation and coding. Study data were collected and managed using REDCap electronic data capture tools hosted at Chula Data Management Center, Faculty of Medicine, Chulalongkorn University. We thank Chula Data Management Center, Faculty of Medicine, Chulalongkorn University for the REDCap administrative support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
TA and SS are joint first authors.
TA and SS contributed equally.
Contributors TA, SS and WK contributed to the conception and design of the work; acquisition, analysis, interpretation of data; and drafting and revision of the work; accepts full responsibility for the work and/or the conduct of the study, and controlled the decision to publish. PV, NW, YP, YA and NA contributed to data acquisition and the final approval of the version to be published.
Funding This study was supported by the Rajadapisek Sompot grant (RA62/011), Health Systems Research Institute (62-034), National Science and Technology Development Agency (FDA-CO-2562-9090-TH) and Thailand Science Research and Innovation (MRG6280158).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.