Article Text

Abstract
Objectives Studies regarding the epidemiology of systemic lupus erythematosus (SLE) are lacking in Argentina. Our purpose was to estimate the incidence and prevalence of SLE in a university hospital-based health management organisation in Buenos Aires (HIMCP).
Methods For incidence calculation, the population at risk included all adult members of the HIMCP, with continuous affiliation for at least 1 year from January 1998 to January 2009. Each person was followed until he/she voluntarily left the HIMCP, death or finalisation of the study. Multiple methods for case finding were used to ensure complete ascertainment: (a) patients with problem SLE, undifferentiated autoimmune disease or mixed connective tissue disease in the Computer-based Patient Record System, (b) patients with positive antinuclear antibody test, anti-Sm antibodies and/or anti-dsDNA antibodies in the laboratory database and (c) patients who consumed hydroxichloroquine, chloroquine, azathioprine, cyclophosphamide, mycophenolate, cyclosporine or rituximab, from the administrative HIMCP drugs database. Medical records of all patients found were reviewed, and only patients fulfilling ACR criteria for SLE were included. Global and gender incidence rate (IR) was calculated. Prevalence was estimated on 1 January 2009, and the denominator population was the number of active members >18 years at that date (n=127 959).
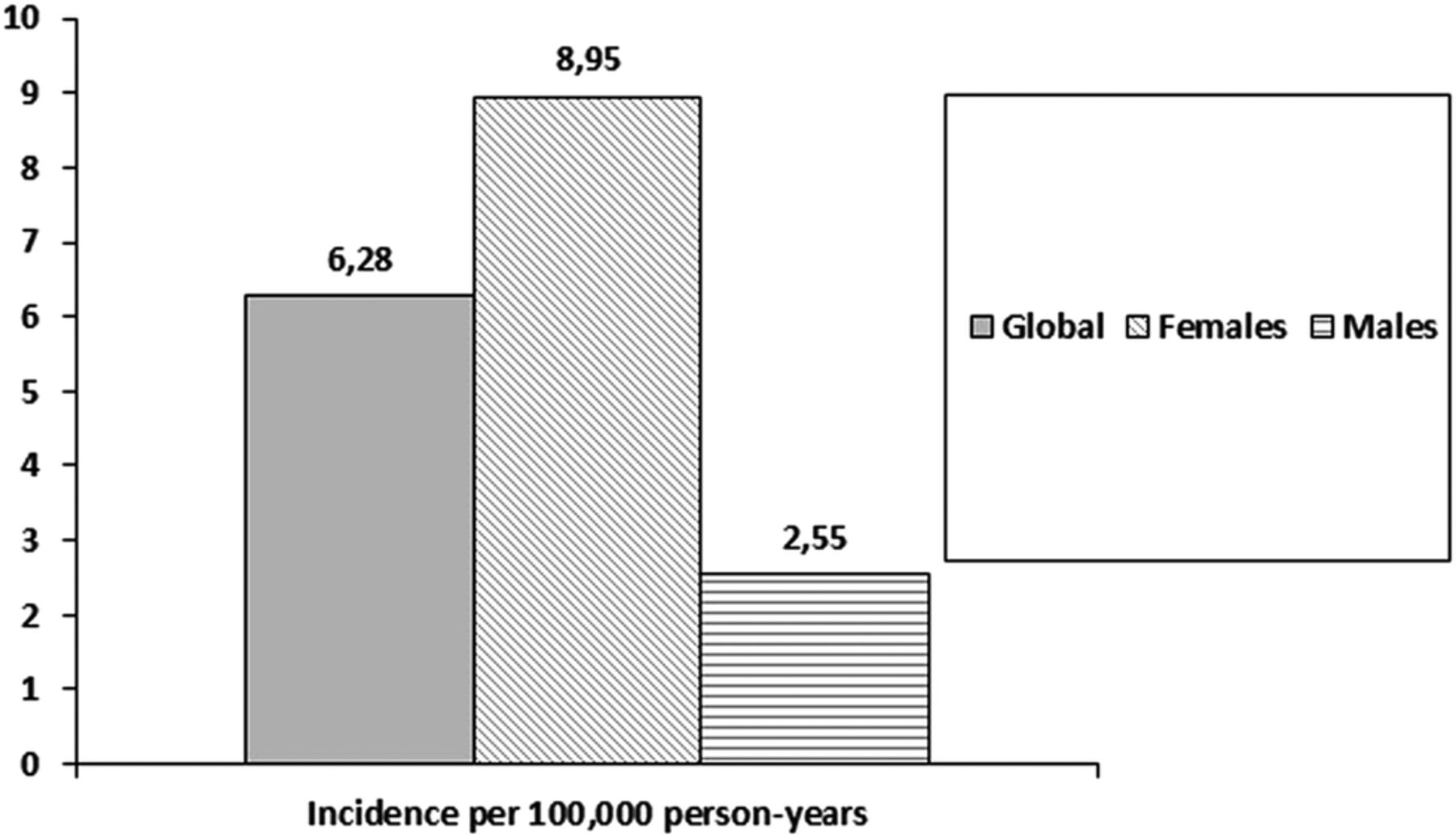
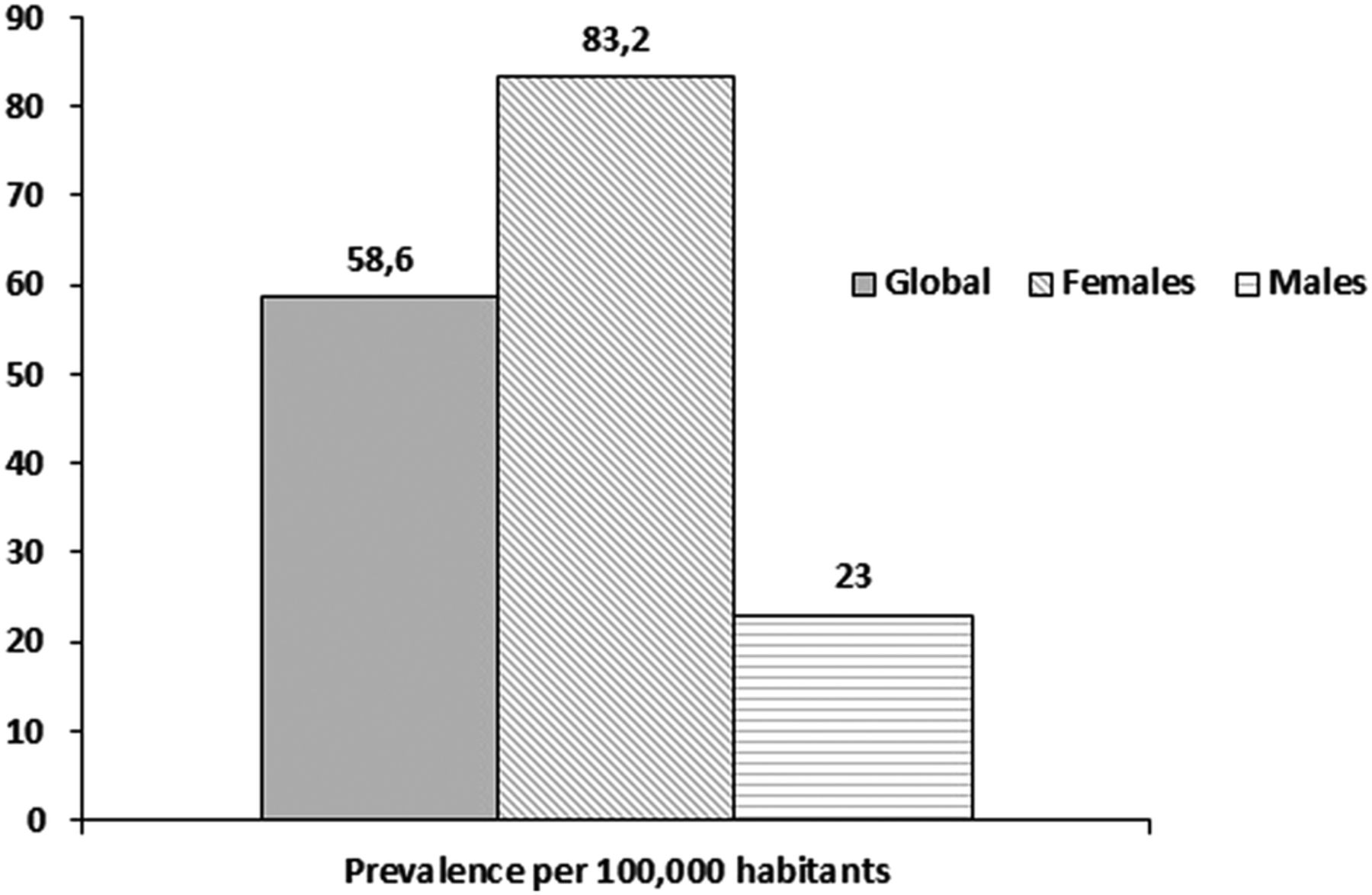
Results In the study period, 68 patients developed SLE. The observed IR (per 100 000 person-years, (CI 95%)) was 6.3 (4.9 to 7.7) for total population; 8.9 (CI 6.6 to 11.2) for women and 2.6 (1.2 to 3.9) for men. On 1 January 2009, 75 prevalent cases were identified. Prevalence rates (cases per 100 000 habitants, (CI 95%)) were 58.6 (46.1 to 73.5) for total population; 83.2 (63.9 to 106.4) for women and 23 (CI 11.9 to 40.1) for men.
Conclusions SLE incidence and prevalence rates in Argentina are in agreement with those of other studies from different parts of the world.
- Epidemiology
- Systemic Lupus Erythematosus
- Autoimmune Diseases
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
-
Incidence and prevalence rates of lupus in Buenos Aires, Argentina were similar to those reported in other studies in Latin America and USA.
-
Females incidence rate peak was on the 20s and prevalence rate peak on the 40s and 50s.
-
Male incidence and prevalence rates were lower and similar among all age groups.
Introduction
The prevalence and incidence of systemic lupus erythematosus (SLE) reported in published studies have remarkable disparities across countries.1
Study methodologies differ and interpretation of results has limitations.2 These limitations include lack of standardised criteria for case detection, passive methods of case ascertainment that miss mild cases (ie, review of inpatient medical records), studies conducted in small geographic areas that make generalisation difficult, studies using self-report or self-report physician diagnosis that report a much higher prevalence (including patients who may not meet strict criteria), and so on.2
The majority of SLE epidemiology studies have been performed in the USA and Europe and most of them have been performed using Caucasian cohorts.1 Several studies have shown that SLE more frequently affects non-Caucasian individuals; prevalence of SLE in the USA is higher in African-Americans, Hispanics and Asians than in Caucasians.1 Additional studies are needed to clarify potential aetiologies, such as genetic factors with regional variation in gene pools and environmental factors including infections, latitude, sun exposure, toxins and diet, which could explain differences in the epidemiology of SLE around the world.
In this sense, scarce data are available on lupus epidemiology in Latin America and in particular in Argentina. Our objective was to estimate the incidence and prevalence of SLE in a university hospital-based health management organisation in Buenos Aires (HIMCP), Argentina.
Methods
Setting
The population studied was the membership of the Hospital Italiano Medical Care Program, a prepaid health maintenance organisation in Buenos Aires, Argentina. Hospital Italiano Medical Care program provides comprehensive medical and health services through two main hospitals and 24 peripheral outpatient centres to around 140 000 members primarily located in the urban areas around the city of Buenos Aires, Argentina. The city covers an area of 202 km2 and has a subtropical climate. It is located on the western bank of the ‘Rio de la Plata’ and has a population of 2 890 151 inhabitants (2010 census).3 In all, 92% of the population is white and of European descent, and the remaining is a mixture of natives and other ethnicities3 (see online supplementary tables S1-S2).
Argentina has a segmented health system consisting of three large sectors: public, private and social security (the last two covering a population of nearly 18.3 million people, distributed among close to 300 entities of varying scope and size). Beneficiaries of the private system can freely choose their health maintenance organisation.
In this context, the Hospital Italiano Medical Care Program is a private health system insurance selected by many city inhabitants because of a perceived excellence of the services provided as well as the affordability of the insurance. Approximately 5%–7% of the population in these geographic areas is affiliated to the Hospital Italiano Medical Care Program. Despite the previously mentioned limitations, the characteristics of these population are fairly representative of the metropolitan population of the city of Buenos Aires, covering a number of demographic and socioeconomic categories3 ,4 (see online supplementary tables S1–S3).
Population
For incidence calculation, the population at risk was that of all adult members (aged >18 years) of the HIMCP, with continuous affiliation for at least 1 year from January 1998 to January 2009. Each person was followed up until he/she was diagnosed with SLE, voluntarily left the Hospital Italiano Medical Care Program, death, or finalisation of the study (final dates) contributing time at risk since January 1998 or enrolment date (whichever occurred later) to the final date.
Case ascertainment
Multiple methods for case finding were used to ensure complete ascertainment: (a) patients with problem SLE, undifferentiated autoimmune disease or mixed connective tissue disease in the Hospital Italiano Medical Care Program problem oriented Computer-based Patient Record System, (b) patients with positive Antinuclear antibody test titer >1/160 and/or positive anti-Sm antibodies and/ or anti-dsDNA antibodies in the Hospital laboratory database and (c) patients who consumed hydroxichloroquine, chloroquine, azathioprine, cyclophosphamide, mycophenolate mofetil, cyclosporine and/or rituximab, from the administrative Hospital Italiano Medical Care Program drugs database. Medical records of all patients found were reviewed, and only patients fulfilling American College of Rheumatology (ACR) criteria for SLE5 were included.
Statistical analysis
Global and gender incidence rate was calculated with 95% CIs. For incidence calculation, the date of diagnosis was considered as that when the diagnosis first appeared in the clinical records and cases had to have been enrolled with the Hospital Italiano Medical Care Program for at least 1 year before this date. Prevalence was estimated in January 2009, and the denominator population was the number of adult Hospital Italiano Medical Care Program active members on that date (n=127 959). Age- and sex-specific incidence and prevalence rate with their 95% CIs were also calculated.
Results
Incidence
In the study period, 186 086 persons contributed a total of 1 082 817.6 person-years. A total of 68 patients developed SLE between 1998 and 1 January 2009. The overall incidence rate was 6.3 (CI 95%: 4.9 to 7.7) cases per 100 000 person-years. All patients were from Caucasian ethnicity.
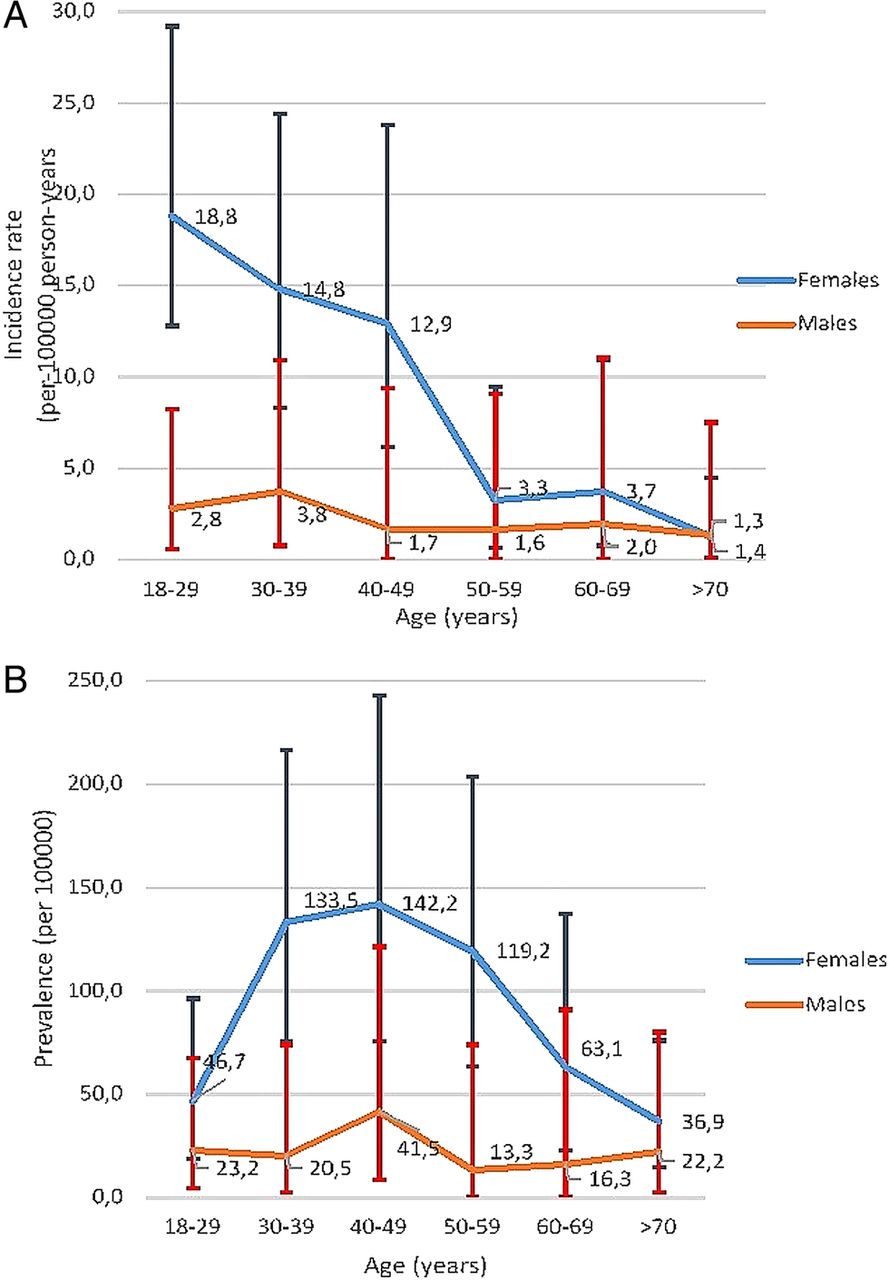
Overall, 57 of the new onset SLE were women (83.8%), with an incidence rate of 8.9 (CI 95%: 6.6 to 11.2) cases per 100 000 person-years. Incidence rate for men was 2.6 (CI 1.2 to 3.9) cases per 100 000 person-years (figure 1). Age-specific incidence rates (figure 2A) in female patients peaked in the 20s, while the rates for male patients appeared more constant across age groups. In older age groups, incidence rates among women and men were much closer than in younger patients (figure 2A).

Incidence of systemic lupus erythematosus by gender.

Age-specific average annual incidence (A) and prevalence (B) rates (per 100 000 persons) of systemic lupus erythematosus, categorised by sex. Values are the point estimate and bars show the 95% confidence intervals.
Prevalence
On 1 January 2009, 75 prevalent cases were identified. Denominator population was the number of active members over 18 years old at that date (n=127 959). Prevalence rate was 58.6 (CI 95% 46.1 to 73.5) cases per 100 000 inhabitants (women 83.2 (CI 95%: 63.9 to 106.4) and men 23 (CI 95% 11.9 to 40.1) per 100 000 members) (figure 3). Age-specific prevalent rates are shown in table 2B. Among women, SLE was more prevalent in the 40s and 50s. The peak prevalence among men was in the 40s.

{kind=link}
{kind=link}
{kind=link}
Incidence of systemic lupus erythematosus by gender.
Comparison with data published from other parts of the world is shown in table 1.
Data on SLE incidence and prevalence around the world
Discussion
The variability in incidence and prevalence estimates of SLE around the world can be attributed to true disparities across the countries or may result from the methodological differences among the studies. Data in table 1 provide a summary of studies performed around the world showing some differences among different countries.
The influences of ethnic, social and demographic variables on the clinical characteristics of SLE patients have already been shown by many studies.42–53 In series from both the USA and Europe, more severe disease was noticed in non-Caucasian populations (Hispanics, African descendants and Asians) than in Caucasians.43 ,47 ,48 ,52 ,54–58
Latin America is a large subcontinent rich in the variety of racial admixtures between and within countries. In addition, socioeconomic, educational and demographic variations are prominent. In consequence, the apparent homogeneity of Latin Americans is a myth, and within the subcontinent lies great diversity.59
Little information on SLE is available from Latin America.59–75
Several studies from the USA have included Latin American patients, usually referring to them as ‘Hispanics’,55 ,56 ,76–80 a term that is mainly derived from their language rather than their ethnic background. Despite this, the so-called Hispanics in the USA have been shown to have more severe disease and poorer outcomes than white Americans,76 ,80 probably because they usually share low socioeconomic status (SES) and Amerindian background, both associated with more sever lupus.
By January 2001, the Grupo Latinoamericano de Estudio del Lupus (GLADEL) cohort included 1214 patients from 34 centres from nine Latin American countries. There were 537 mestizos (44%), 507 white patients (42%) and 152 African-Latin Americans (ALA) (13%). There were small numbers of pure Amerindian and oriental individuals. White patients predominated in Argentina and Cuba and in a lesser degree in Brazil. Mestizos predominated in Guatemala, Mexico and Peru. ALA patients were more prevalent in Venezuela, Brazil and Colombia.59
In the GLADEL cohort, both ALA and mestizos had more severe disease than white patients, as evidenced by a higher frequency of renal disease, pericarditis, polyadenopathy and discoid lesions in ALA. Mestizos and ALA had lower SES, fewer years of formal education and less accessibility to medical care than white patients, and these socioeconomic factors may have a bearing on the more severe disease found in non-whites.59
No data have been published before on incidence and prevalence of SLE in Argentina. Our study has some limitations. It was performed in a health maintenance organisation and therefore contains some selection bias. However, as shown in online supplementary tables S1 and S2, comparison of this health maintenance organisation population with that of the city of Buenos Aires shows that it is fairly representative of that population, although there are some differences, mainly in the SES. These differences might affect the prevalence as patients with poorest SES have less survival. However, we think that with caution, results obtained in this study could be extrapolated to the whole city of Buenos Aires. Buenos Aires population may not be representative of the complete Argentinian population since it has mainly a European origin, showing a lesser proportion of mestizos than the rest of the country. For example, Argentinian SLE patients included in GLADEL (also a non-randomised Argentinian sample) were 17.1% mestizos, while in our study only 2.3% were mestizos. Due to the low number of persons from other ethnicities, we were unable to compare the epidemiology of the disease according to ethnic origin; in fact, all patients were classified as white in our study. As the study was undertaken in a healthcare organisation where ‘ill’ patients are not incorporated, we may have a bias when considering prevalent cases because patients with existing disease would not have been allowed to enter the health maintenance organisation. This fact did not appear to have a great effect as our prevalence is similar to other studies, and this limitation would not affect incidence rates.
Despite these limitations, this study provides the first estimation of the incidence and prevalence of SLE in Argentina using the same methodology we used in previous studies with other rheumatic diseases.81–83
More efforts are needed to achieve a better characterisation of the Argentinian lupus population in order to understand the burden of SLE in the country. A more profound knowledge of the local lupus epidemiology may allow establishing country-specific healthcare policies.
Conclusions
Incidence and prevalence of SLE in this study population from Argentina were within the range of estimates previously reported in other countries.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All authors contributed to the conception and design of the study, acquisition and/or interpretation of data, drafting the article or revising it critically for important intellectual content and approved the final version of the manuscript.
-
Funding This study was funded by Rheumatology Section, Medical Services, Hospital Italiano de Buenos Aires.
-
Competing interests None.
-
Ethical approval We received confirmation from our Ethical Committee that ethics approval was not required for this retrospective study.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.