Article Text

Abstract
Objective Assess the safety and efficacy of belimumab in older adults with SLE.
Methods This post hoc integrated analysis (GSK Study 116559) included safety data from six randomised, placebo-controlled belimumab trials (BLISS-76, BLISS-52, BLISS-SC, North East Asia study, LBSL02, EMBRACE; n=4170). The BASE study provided additional safety data (n=4003). Efficacy data were from five of the trials. Older adults (≥65 years) were compared with the overall populations of patients with SLE. Patients who had received ≥1 treatment dose were included.
Results Sixty-three older adults (1.5%) were included in the pooled safety analysis population and 156 (3.9%) in the BASE study. At baseline, older adults had lower disease activity but more organ damage than the overall populations. In the pooled safety analysis population, five (18.5%) placebo-treated and ten (27.8%) belimumab-treated older adults experienced ≥1 serious adverse event (SAE), as did 230 (17.0%) placebo-treated and 421 (15.0%) belimumab-treated patients overall. In the BASE study, nine (11.0%) placebo-treated and six (8.1%) belimumab-treated older adults experienced ≥1 SAE, as did 222 (11.1%) placebo-treated and 220 (11.0%) belimumab-treated patients overall. No clinically relevant differences in deaths and adverse events of special interest were observed between older adults and the overall populations. Older adults’ SLE Responder Index response rates favoured belimumab versus placebo, consistent with the overall population.
Conclusion The safety and efficacy of belimumab in older adults were generally consistent with the overall populations, suggesting belimumab is a treatment option for older patients with SLE. Due to small numbers of older adults, findings should be interpreted with caution.
- Autoimmune Diseases
- Lupus Erythematosus, Systemic
- Inflammation
Data availability statement
GSK is committed to publicly disclosing the results of GSK-sponsored clinical research that evaluates GSK medicines, and as such was involved in the decision to submit. Anonymized individual patient data and study documents can be requested for further research from www.clinicalstudydatarequest.com.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Data on the efficacy and safety of belimumab, an anti-B-lymphocyte stimulator recombinant human immunoglobulin G1λ monoclonal antibody, in older adults (aged ≥65 years) with SLE are limited.
WHAT THIS STUDY ADDS
This integrated analysis of data from randomised, placebo-controlled trials of belimumab plus standard therapy demonstrated that the safety and efficacy of belimumab in older adults with SLE were generally consistent with the overall study populations.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The findings, although limited by the small numbers of older adults within the clinical trials, suggest that belimumab is a treatment option for this subpopulation of patients with SLE.
Introduction
Older adults with SLE have high unmet needs due to comorbidities and increased risk of treatment toxicities, as well as greater damage accrual and higher mortality rates versus early-onset SLE.1–3 Although disease activity of patients with true late-onset SLE may differ from older patients who developed SLE earlier in life, these risks will remain.
Belimumab has demonstrated efficacy and safety in patients with SLE.4–7 Due to low numbers of older adults within clinical trials and the low SLE incidence in this age group, data on the use of belimumab in this population are limited.8 9 The objectives of this analysis were to assess the safety and efficacy of belimumab in older adults with SLE.
Methods
Study design
This post hoc analysis (GSK Study 116559) evaluated the safety of belimumab in older adults with SLE (aged ≥65 years at baseline) compared with the overall population using pooled data from six randomised, placebo-controlled trials (BLISS-76 (NCT00410384),4 BLISS-52 (NCT00424476),5 BLISS-SC (NCT01484496),6 North East Asia (NEA) study (NCT01345253),7 LBSL02 (NCT00071487)10 and EMBRACE (NCT01632241)11) (online supplemental figure 1). Additional safety data were obtained from a large, randomised, controlled study in adults with SLE (BASE (NCT01705977)), in which the primary focus was safety.12 Data from BASE were presented side-by-side with the pooled data (pooled safety analysis population) due to differing study size, population and data collection.
Supplemental material
In the efficacy analyses, older adult data were pooled from BLISS-76, BLISS-52, NEA study, BLISS-SC and EMBRACE, and were presented side-by-side with the overall population data from BLISS-76 and BLISS-52 pooled, NEA study, BLISS-SC and EMBRACE. LBSL02 was excluded from the efficacy analysis due to differing medication rules, efficacy endpoints and gating techniques for the biomarker assays.
Population
Full inclusion and exclusion criteria and the ethical conduct of each trial have been published (summarised in the online supplemental methods).4–7 10–12
Treatment
Patients received belimumab or placebo in addition to standard therapy (online supplemental figure 1).4–7 10–12 Randomisation ratio (belimumab (all doses):placebo) was 2:1 for all studies in the pooled safety analysis, except LBSL02 (3:1). For BASE, the randomisation ratio was 1:1.
Endpoints
Safety outcomes in the pooled safety analysis population included incidence of adverse events (AEs), serious adverse events (SAEs), adverse events of special interest (AESI) and deaths. In BASE, safety outcomes included incidence of SAEs, AESI and deaths.
The efficacy outcome in this pooled analysis was the SLE Responder Index (SRI) response rate at week 52. This was the primary efficacy endpoint for BLISS-76, BLISS-52, NEA study and BLISS-SC.4–7 For EMBRACE, the primary efficacy endpoint was the SRI response rate at week 52 with modified Systemic Lupus Erythematosus Disease Activity Index (SLEDAI)−2K scoring for proteinuria; SRI with Safety of Estrogens in Lupus Erythematosus National Assessment version of the SLEDAI (SELENA-SLEDAI) scoring was a key secondary efficacy endpoint.11 SRI with SELENA-SLEDAI scoring findings did not differ from SRI-SLEDAI-2K analysis; therefore, SRI with SELENA-SLEDAI scores are presented here for comparison.
Statistical analysis
For safety analyses, the primary population was older adults who were randomised and received ≥1 dose of study drug (older adult intent-to-treat (ITT) population). The overall ITT population was all randomised patients (planned treatment group) who received ≥1 dose of study drug. For BASE, the ITT population was used for population summaries, and the ‘as-treated’ population was used for safety analyses (one patient (placebo) received non-planned study treatment for >50% of doses). All safety analyses were descriptive.
For efficacy analysis, the modified ITT older adult and overall populations were the ITT population, excluding patients from three sites in EMBRACE and one site in the NEA study due to potential Good Clinical Practice non-compliance.
ORs and 95% CIs were calculated from a logistic regression model for comparison of SRI response rate between belimumab and placebo.
Patient and public involvement
Patients and/or public were not involved in the study design or dissemination of this pooled analysis.
Results
Patients
Overall, 63 of 4170 patients in the pooled safety analysis population and 156 of 4003 patients in BASE were older adults. Most older adults completed their studies (pooled safety analysis: 20 (74.1%) placebo, 29 (80.6%) belimumab), similar to the overall population (1038 (76.6%) placebo, 2280 (81.0%) belimumab). Most common reasons for discontinuation in older adults were AEs (pooled safety analysis: 1 (3.7%) placebo, 3 (8.3%) belimumab; overall: 97 (7.2%) placebo, 169 (6.0%) belimumab) and patient request (pooled safety analysis: 4 (14.8%) placebo, 2 (5.6%) belimumab; overall: 71 (5.2%) placebo, 108 (3.8%) belimumab).
Demographics and disease characteristics
Most older adults (~80%) were aged ≥50 years at SLE diagnosis (late onset). In the pooled safety analysis population and BASE, older adults had lower disease activity but more organ damage compared with the overall population (table 1). Most older adults were using glucocorticoids and/or antimalarials at baseline.
Background demographics and disease characteristics
Safety
When comparing older adults and the overall population, there were no clinically relevant differences in the incidence of AEs or SAEs in the pooled safety analysis population or the incidence of SAEs in BASE (table 2).
Treatment-emergent AEs, SAEs and severe AEs in older adults and the overall populations
In the pooled safety analysis population, the most commonly reported SAEs in belimumab-treated older adults were nervous system disorders and vascular disorders. Overall, two of four nervous system disorder SAEs reported in belimumab-treated older adults were considered severe (neuritis and transient ischaemic attack), one of which (neuritis) led to treatment discontinuation. All four nervous system disorder SAEs were considered unrelated to the study drug and resolved. Two of three vascular disorder SAEs reported in belimumab-treated older adults were considered severe (both arteriosclerosis); none led to discontinuation and all were considered unrelated to the study drug. In placebo-treated older adults, the most commonly reported SAE was psychiatric disorders. Review of individual cases identified no clinical concern in terms of trends or clustering of events.
The most commonly reported SAEs in older adults in BASE (placebo and belimumab) were infections and infestations, cardiac disorders and gastrointestinal disorders. When examined by the preferred term, pneumonia was reported in two (2.4%) placebo-treated older adults in BASE; all others in older adults were singular events.
In both the pooled safety analysis and BASE, there were no clinically relevant differences in number of deaths in older adults compared with the overall population (online supplemental table 1).
There were no imbalances in rates of AESI (postinfusion/injection systemic reactions (PISRs), serious infections of special interest, malignancies, depression (including mood disorders/anxiety) and suicide/self-injury), either between older adults and overall, or between belimumab and placebo in older adults (online supplemental table 1).
In the pooled safety analysis population, PISRs were reported in 2 (5.6%) belimumab-treated older adults and 286 (10.2%) belimumab-treated patients overall. There was one infection of special interest (herpes zoster) in older adults (placebo); no older adults experienced malignancies. Depression was reported in 3 (8.3%) belimumab-treated older adults and 205 (7.3%) belimumab-treated patients overall. One older adult case of depression was serious (placebo); no older adults in either treatment group had suicide/self-injury events.
In BASE older adults, there were no serious PISRs or malignancies. Two (2.7%) belimumab-treated older adults had serious infections of special interest (sepsis), and one (1.4%) experienced a serious suicide/self-injury event (suicide attempt). Overall, 17 (0.8%) and 11 (0.5%) belimumab-treated patients had serious infections of special interest and serious suicide/self-injury events, respectively. Serious infections of special interest reported by these 17 patients comprised 8 opportunistic infections, 2 cases of active tuberculosis, 1 herpes zoster infection and 10 cases of sepsis.
Efficacy
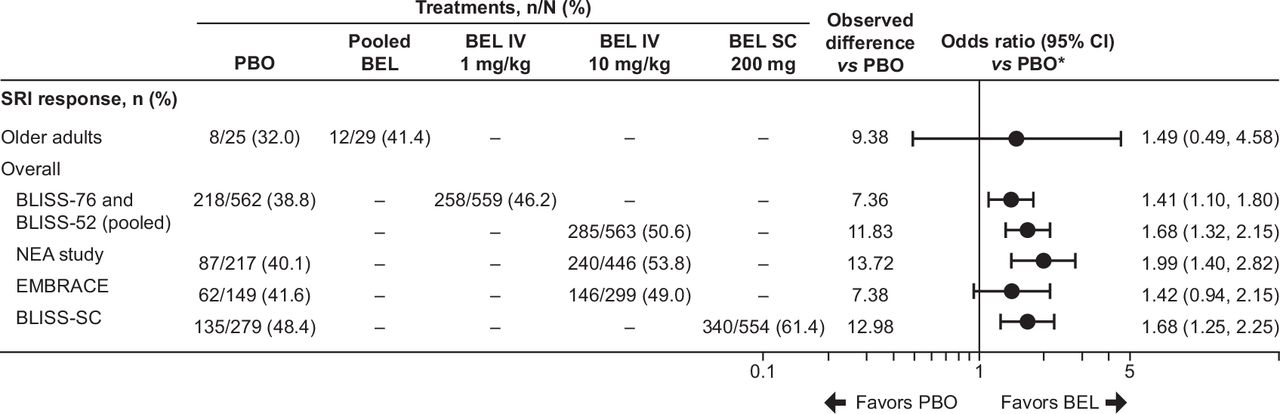
The SRI response rate at week 52 in older adults favoured belimumab versus placebo, consistent with overall (figure 1). When evaluating the three components of SRI response, the observed difference in ≥4-point reduction in SELENA-SLEDAI score between belimumab and placebo in older adults was generally comparable to overall (online supplemental table 2). The observed difference in no worsening in Physicians Global Assessment and no new 1A/2B British Isles Lupus Assessment Group domain scores between belimumab and placebo was slightly lower in older adults compared with overall.

{kind=link}
SRI response rate at week 52 for older adults and the overall populations. *In the pooled efficacy analysis (older adults), covariates were treatment and baseline SELENA-SLEDAI score (≤9 vs ≥10). For BLISS-76 and BLISS-52, covariates included treatment, baseline SELENA-SLEDAI score (≤9 vs ≥10), baseline proteinuria level (<2 vs ≥2 g/24 hours equivalent) and race (black African ancestry vs other). For BLISS-SC, covariates were treatment, baseline SELENA-SLEDAI score (≤9 vs ≥10), baseline complement levels (low C3 and/or C4 vs no low C3/C4) and race (black African ancestry vs other). For the NEA study, independent variables were treatment, country, baseline SELENA-SLEDAI score (≤9 vs ≥10) and complement levels (low C3 and/or C4 vs no low C3/C4). For EMBRACE, covariates were treatment, baseline SELENA-SLEDAI score (≤9 vs ≥10), baseline complement levels (≥1 low C3 and/or C4 vs no low C3/C4) and region (USA/Canada vs rest of world). BEL, belimumab; NEA, North East Asia; PBO, placebo; SELENA-SLEDAI, Safety of Estrogens in Lupus Erythematosus National Assessment version of the Systemic Lupus Erythematosus Disease Activity Index; SRI, Systemic Lupus Erythematosus Responder Index.
Discussion
This analysis included 8173 patients with SLE, with 219 older adults. Baseline characteristics and demographics of the overall populations were generally consistent with previous SLE studies and representative of real-world populations.13 The higher baseline Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index score in older adults is consistent with cumulative and irreversible organ damage accompanying the disease course, and published data show age is associated with damage accrual.14 The lower baseline disease activity in older adults versus overall is consistent with previous studies in patients with late-onset SLE1 2 and may be partially explained by the greater likelihood of menopause and lower oestrogen levels in older female patients.9 Oestrogens have established immunomodulatory effects and may exacerbate SLE disease activity.9
Safety analysis showed no clinically relevant differences in the incidence of AEs (pooled safety analysis population), SAEs, AESI or death between older adults and overall populations. There were no imbalances in AESI between belimumab and placebo in older adults. When SAEs were examined by preferred terms, no clustering of events occurred. Pneumonia was reported in two (2.4%) placebo-treated BASE older adults; all others were singular events.
SRI response rate in older adults favoured belimumab over placebo, consistent with overall populations.
The small numbers of older adults (pooled safety analysis: n=63/4170 (1.5%), BASE: n=156/4003 (3.9%)) mean that findings should be interpreted with caution. The safety and efficacy of belimumab in older adults were generally consistent with overall populations and suggest a favourable benefit–risk profile. However, efficacy analyses beyond SRI were not reported, owing to no observations and/or small sample size. An additional limitation is that effects of comorbidity on benefit–risk are not addressed.
Given the small number of older adults with SLE and complexities associated with their comorbidities, controlled clinical trials in this patient population are not feasible. These analyses suggest belimumab is a treatment option for older adults with SLE and provide useful information to inform clinical practice.
Data availability statement
GSK is committed to publicly disclosing the results of GSK-sponsored clinical research that evaluates GSK medicines, and as such was involved in the decision to submit. Anonymized individual patient data and study documents can be requested for further research from www.clinicalstudydatarequest.com.
Ethics statements
Patient consent for publication
Ethics approval
Studies were conducted according to the ethical principles of the Declaration of Helsinki, International Council for Harmonisation on GCP and applicable country-specific regulations. Studies were approved by a central or local institutional review board or ethics committee. All patients provided written informed consent.4–7 10–12
Acknowledgments
Medical writing and submission support were provided by Helen Taylor, PhD, Fishawack Indicia Ltd, UK, part of Fishawack Health, and was funded by GSK. All authors approved the submission of this article via a third party and approved all statements and declarations. A summary of these data was presented as a poster at the European Alliance of Associations for Rheumatology 2021 congress.15
References
Footnotes
Contributors GE, AH, BJ and DAR contributed to the conception or design of the study. DD’C acquired the data. All authors contributed to the analysis and interpretation of the data.
Funding This study was funded by GSK (GSK Study 116559).
Competing interests DD’C worked as a consultant for GSK, UCB and Eli Lilly and was a paid speaker for GSK and Vifor Pharma. GE, YG, AH, BJ and DAR are employees of GSK and own stocks and shares in the company. PM was an employee of GSK at the time of the study and held stocks and shares in the company.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.