Article Text

Abstract
Background Vitamin D status varies with geographic location and no studies of vitamin D in systemic lupus erythematosus (SLE) have been reported in the Southern Hemisphere.
Objectives To assess the prevalence of vitamin D deficiency in an Australian SLE cohort, and its relationship with disease activity.
Methods Data were collected prospectively on 119 consecutive patients with SLE in the Monash Lupus Clinic in Melbourne, Australia, between January 2007 and January 2013. Patients had simultaneous serum 25-hydroxyvitamin D concentration and disease activity (SLEDAI-2K) recorded. Statistical methods were used to determine the correlation of serum vitamin D level and disease activity both at baseline and at a subsequent time point. Adjustments were made for the use of glucocorticoids, immunosuppressants and vitamin D supplementation.
Results Vitamin D deficiency (<40 nmol/L) was detected in 27.7% of patients at baseline. Multiple regression analysis showed a significant inverse correlation of SLEDAI-2K with baseline vitamin D level and with vitamin D supplementation. Over a 12-month period of observation, among the 119 patients, there were 464 serial vitamin D measurements with corresponding SLEDAI-2K, representing 266 time intervals. The median change in vitamin D level was an increase of 25 nmol/L and this corresponded with a decline in SLEDAI-2K of 2 units. In regression analysis, there was a significant association between low vitamin D at a prior time point and a rise in SLEDAI-2K at the subsequent time point (univariable OR 3.3, 95% CI 1.5 to 7.7, p=0.005) or having a high disease activity (SLEDAI-2k>10) at the subsequent time point (univariable OR 3.1, 95% CI 1.4 to 6.8, p=0.004).
Conclusions In Australian patients with SLE, low vitamin D was associated with a higher disease activity and an increase in serum vitamin D was associated with reduced disease activity over time. The therapeutic effect of vitamin D in SLE should be further assessed in interventional studies.
- Systemic Lupus Erythematosus
- Disease Activity
- Autoimmune Diseases
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
-
This is the first published study looking at the association of low vitamin D with SLE disease activity in the Southern hemisphere.
-
In an Australian SLE cohort, low vitamin D was associated with a higher disease activity.
-
An increase in serum vitamin D level was associated with reduced SLE activity over time.
Introduction
Vitamin D is a steroid hormone that has a well-established role in calcium metabolism and bone homeostasis.1 Vitamin D has two physiological forms, vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol). The primary source of vitamin D3 is synthesis by UVB radiation exposed skin. Thereafter, vitamin D undergoes hepatic metabolism to 25-hydroxyvitamin D (25(OH)D), the form conventionally measured in serum in clinical assays of vitamin D status. In the kidney, 25(OH)D is further metabolised to 1,25-dihydroxyvitamin D, which works by binding to the vitamin D receptor (VDR) located in the nuclei of target cells.
Following the discovery that VDRs are expressed by immune cells, including antigen-presenting cells, natural killer cells, and B and T lymphocytes, the concept that vitamin D has roles in the regulation of the immune response has emerged.2 Vitamin D deficiency has been associated with several autoimmune diseases including multiple sclerosis,3 rheumatoid arthritis,4 type1 diabetes mellitus,5 and systemic lupus erythematosus (SLE).3–9
SLE is a chronic multisystem inflammatory autoimmune disease that is characterised by immunological abnormalities resulting in the production of autoantibodies. The steps leading to autoimmune-mediated inflammation are believed to be stimulated by the uptake of nucleic acid-containing immune complexes by plasmacytoid dendritic cells, and the resulting activation of Type I interferon expression. This inflammatory milieu promotes defective function of regulatory T cells (Tregs) and hyperactivity of helper T cells (Th cells), and the survival and activation of autoreactive B cells that produce autoantibodies.10 There is increasing evidence to suggest that vitamin D impacts negatively on many of these events. This includes vitamin D-induced downregulation of the Th1 immune response and of the proliferation of activated B cells,11 while upregulating Tregs.12 A recent study showed that vitamin D3 inhibits dendritic cell maturation and expression of IFN-α induced genes in SLE patients.13
Patients with SLE are prone to vitamin D deficiency, because of factors such as avoidance of sunshine due to photosensitivity,14 the use of sun-screen,15 chronic renal insufficiency16 and the use of medications such as glucocorticoids17 and antimalarials18 that may enhance the clearance of vitamin D. Accordingly, several recent studies have emerged identifying a possible association of low vitamin D and disease activity in SLE.19 ,20 The frequency of vitamin D deficiency varies greatly between communities in different latitudes.7 ,9 ,16 ,21 ,22 Currently, it is not yet known whether observations made in a certain location are applicable globally. Moreover, knowledge about the impact on SLE of vitamin D supplementation, often given to SLE patients as part of a preventive approach to osteoporosis or in an attempt to treat vitamin D deficiency, is lacking.
The objectives of our study were (1) to determine the prevalence of vitamin D deficiency in an Australian SLE cohort, representing the first such study from the Southern Hemisphere; (2) to determine the relationship between disease activity and vitamin D deficiency in this cohort; and (3) to determine whether vitamin D supplementation is associated with increases in vitamin D and whether this in turn is associated with reduced disease activity.
Patients and methods
Study population
Between January 2007 and January 2013, data including demographic and disease characteristics were collected prospectively at each visit in patients with SLE who attended the Monash Medical Centre Lupus Clinic. In this clinic, the longitudinal collection of disease activity data recorded using the SLEDAI-2K23 takes place at every visit.
The study was approved by the Human Research Ethics committee of Monash Health, and all patients provided written informed consent. For this study, we recruited all patients who fulfilled the revised American College of Rheumatology (ACR) criteria for the classification of SLE24 and had at least one serum vitamin D concentration measured in conjunction with a clinical visit at which SLE data were collected. Other variables measured at baseline were demographic variables including self-reported ethnicity. When serial serum vitamin D was measured, a number of laboratory variables were concurrently measured, including erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), anti-double-stranded DNA (dsDNA) antibodies, renal function (serum creatinine and estimated glomerular filtration rate (eGFR)), and complement levels (C3 and C4). Glucocorticoid, immunosuppressive drug and vitamin D supplementation use were also noted both at initial and subsequent occasions when serum vitamin D was measured. Lumbar spine and femoral neck bone density data measured using dual energy x-ray absorptiometry were recorded where this had been measured within 12 months of the baseline vitamin D assessment.25 ,26
Measurement of 25(OH)D3 level and definition of insufficiency
Vitamin D levels in the majority of samples were analysed at Monash Health clinical pathology service using the DiaSorin assay. For a minority of patients, vitamin D levels were measured at external pathology laboratories. Levels are expressed in nmol/L, and vitamin D level less than 40 nmol/L was considered as vitamin D deficiency.
Statistical analysis
Baseline vitamin D analysis
The date of the first vitamin D measurement was designated the date of study entry, also referred to as ‘baseline’. The relationships between baseline vitamin D level and ESR, CRP, lumbar spine T-scores and femoral neck T-scores on bone densitometry at baseline were evaluated using Pearson's correlation coefficient and depicted in the form of scatter plots. Multiple linear regression was used to assess the relationship between baseline vitamin D level and SLEDAI-2K, vitamin D supplementation and glucocorticoid use at baseline.
Change in vitamin D over 1 year
Changes in vitamin D and SLEDAI-2K over the first year of follow-up were reported as mean (SD) and median, and the correlation between these was assessed using Pearson's correlation coefficient and simple linear regression.
Analyses using serial vitamin D measurements
The mean and median number of vitamin D measurements per patient, the time between measurements and the duration of follow-up were reported. Univariate (χ2) and logistic regression analysis were used to determine the relationship between low vitamin D at a prior time point and a rise in SLEDAI-2K at the subsequent time point of at least one unit. Similar analyses were undertaken to assess the relationship between low vitamin D at a prior time point and a SLEDAI-2K of 10 or greater at the subsequent time point.
Logistic regression analysis was used to determine the relationship between low vitamin D at a prior time point and SLEDAI-2K at the subsequent time point, while adjusting for the use of glucocorticoids, immunosuppressives and vitamin D supplementation during the interval, and accounting for the expected correlation in repeated measurements of vitamin D in each patient using generalised estimating equations.
Results
Baseline vitamin D analysis
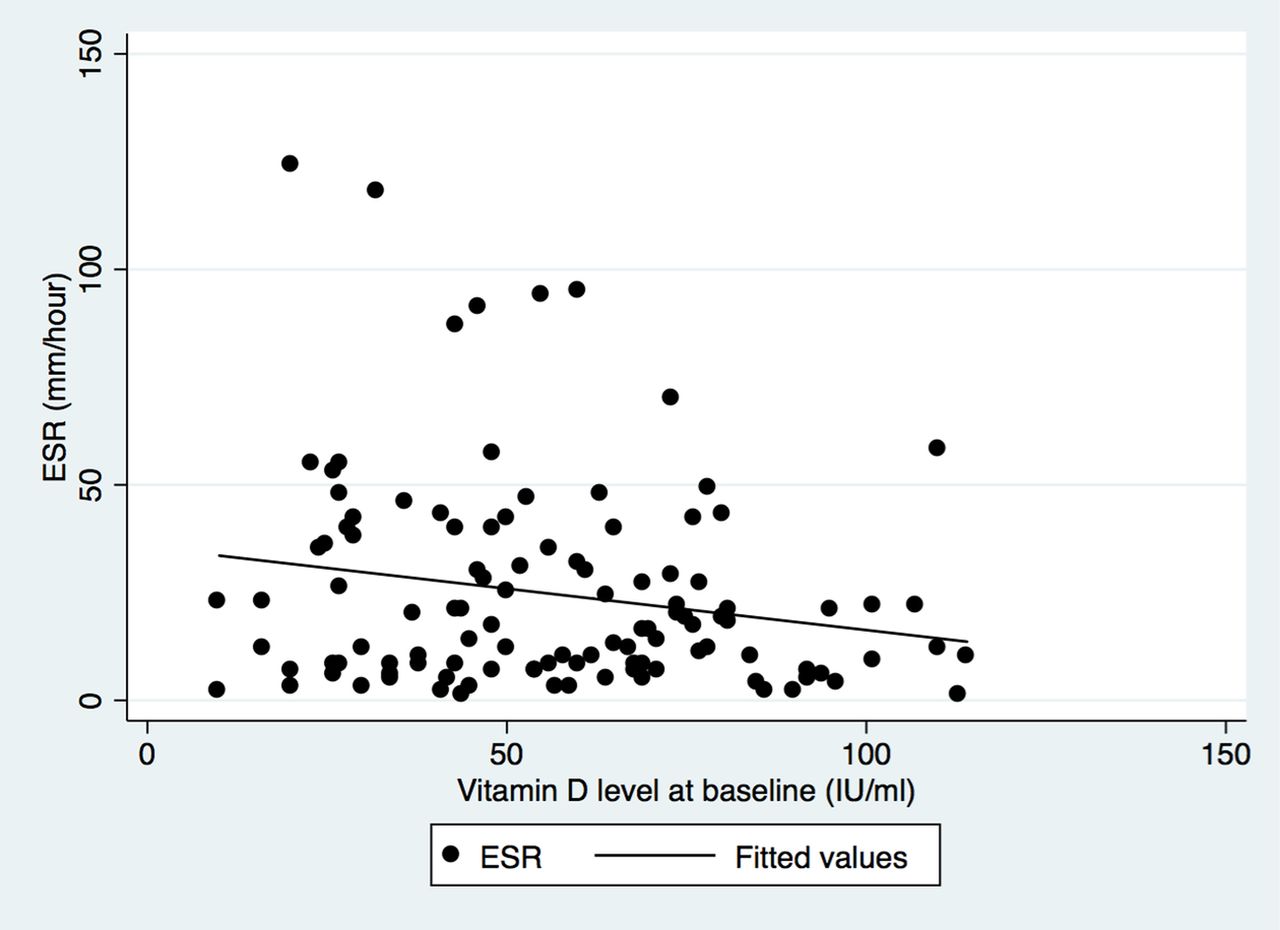
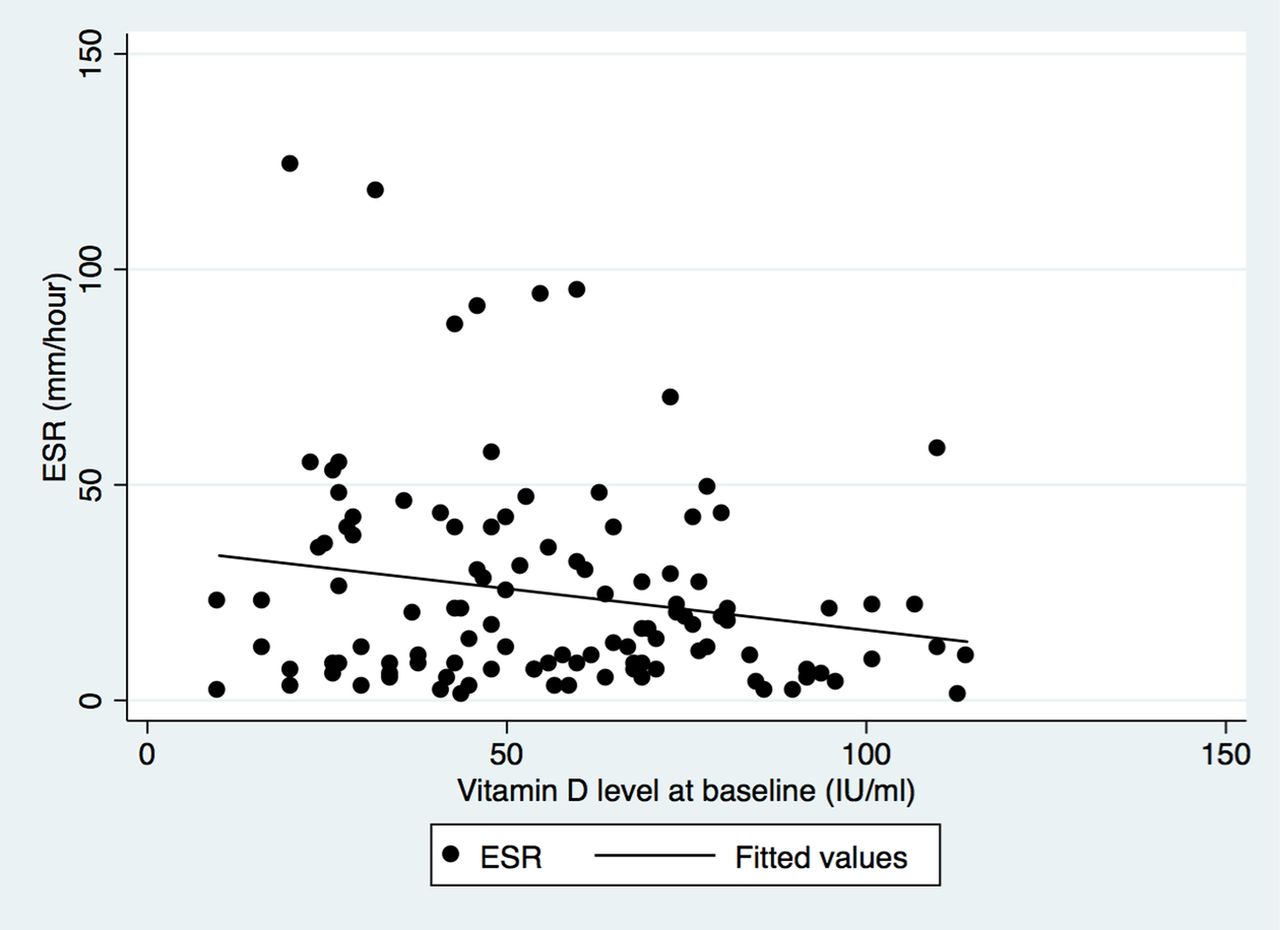
Patient characteristics are presented in table 1. Thirty three (27.7%) patients were vitamin D deficient (<40 nmol/L) at study entry, while 53 (44.5%) were on vitamin D supplementation. There was a significant, albeit weak inverse correlation between vitamin D level and ESR at baseline (r=−0.2, p=0.04), depicted in figure 1. However, there was no significant correlation between vitamin D level at baseline and CRP, or with femoral neck and lumbar spine bone density (T scores) at baseline.
Patient characteristics (n=119)
{kind=link}
Dot plot and line of best fit, depicting the relationship between vitamin D level and erythrocyte sedimentation rate (ESR) at baseline.
In multiple linear regression analysis (table 2), baseline vitamin D level was significantly and inversely correlated with SLEDAI-2K, and with vitamin D supplementation, but not with glucocorticoid use. In a different model that excluded SLEDAI-2K due to its collinearity with ESR, vitamin D level at baseline was also significantly correlated with ESR (β=−0.3, p=0.01, 95% CI −0.4 to −0.06), even after adjustment for vitamin D supplementation and glucocorticoid use. There was no significant relationship between immunosuppressant use and serum vitamin D level at baseline. As all patients were on hydroxychloroquine, its relationship to serum vitamin D could not be determined.
Multiple regression analysis of correlates of baseline vitamin D
Change in vitamin D over time
Over 12 months of follow-up from the baseline assessment, the median change in vitamin D level was an increase of 25 nmol/L, while there was a median decline in SLEDAI-2K of 2 units. There was no significant correlation between change in SLEDAI-2K and change in vitamin D level over 12 months, when assessed using Pearson's correlation coefficient (r=−0.2, p=0.2), or in linear regression (β=−0.2, 95% CI −3.0 to 0.7, p=0.2).
Among the 119 patients, there were a total of 464 serial vitamin D measurements with corresponding SLEDAI-2K recorded at the same time, representing 266 time intervals over a mean (SD) follow-up of 0.95 (0.79) years. Characteristics of the serial vitamin D data set are presented in table 3. Forty three of the 119 patients (36.1%) had low vitamin D (<40 nmol/L) during follow-up, and 26 of 119 patients (21.8%) had high disease activity (SLEDAI-2K >10). In regression analysis, there was a significant association between low vitamin D at a prior time point and a rise of at least 1 unit in SLEDAI-2K at the subsequent time point, with a univariable OR of 3.3, 95% CI 1.5 to 7.7, p=0.005. Similarly, there was a significant association between low vitamin D at a prior time point and a SLEDAI-2K greater than 10 points at the subsequent time point, with a univariable OR of 3.1, 95% CI 1.4 to 6.8, p=0.004. However, after adjustments for covariates, namely vitamin D supplementation, glucocorticoid and immunosuppressive use during the intervening time interval, these associations were no longer significant, suggesting that vitamin D supplementation and treatment of SLE may modify the relationship between serum vitamin D and subsequent disease activity.
Serial vitamin D data (464 measurements among 119 patients)
Discussion
This is a longitudinal study of a large group of Australian patients with SLE. We found that there is a high prevalence of vitamin D deficiency in our cohort, with over a quarter of the patients having vitamin D level less than 40 nmol/L. This is in keeping with reports from other parts of the world, including Asia16 ,27 and Europe,14 ,21 even though vitamin D varies with geographic location and season. Although we did not demonstrate any significant association between vitamin D deficiency and ethnicity in our cohort, it is important to note that our cohort has a high proportion of Asian patients.
This is the first longitudinal study of vitamin D and SLE in the Southern Hemisphere. We describe an inverse association between serum vitamin D level and SLE disease activity. We also demonstrate a significant inverse correlation between vitamin D level and ESR at baseline and in multiple linear regression9 analysis after adjustment for vitamin D supplementation and glucocorticoid use. Our findings are consistent with several other observational studies that have shown that vitamin D level inversely correlates with disease activity.7–9 ,16 ,21 ,22 ,27–29 In the longitudinal follow-up, univariable analysis showed significant associations of vitamin D with subsequent increases in SLEDAI-2K or high disease activity (SLEDAI-2K >10), each with ORs greater than 3. The predictive effect of low vitamin D on subsequent disease activity did not remain significant after adjustment for vitamin D supplementation, glucocorticoid use and immunosuppressive use, suggesting that in future studies of vitamin D effects in SLE, these variables should be controlled for.
In multiple regression analysis, we found a significant inverse correlation of SLEDAI-2K with baseline vitamin D concentration and with vitamin D supplementation. Importantly, there was a significant association between low vitamin D (<40 nmol/L) at a prior time point and a rise in SLEDAI-2K (1 or more units) at a subsequent time point (univariable OR 3.3, 95% CI 1.5 to 7.7, p=0.005) or having high disease activity (SLEDAI-2K>10) at a subsequent time point (univariable OR 3.1, 95% CI 1.4 to 6.8, p=0.004). These findings are in contrast to a recent study by Schoindre et al,21 which showed that lower vitamin D was not predictive of disease flare up.
A large proportion of our patients were receiving vitamin D supplementation. Although our study was not designed to determine the indication for the prescription of vitamin D supplementation, it is likely that physicians were influenced by the high prevalence of glucocorticoid use, and associated osteoporosis risk in these SLE patients.25 ,26 The role of vitamin D in the therapy of SLE per se is unclear. Recent interventional trials have provided insight into potential benefits. Abou-Raya et al30 randomised 267 SLE patients in a 2:1 ratio to receive either oral cholecalciferol 2000 IU/day or placebo. After 12 months, there was a significant reduction in the levels of proinflammatory cytokines (IL-1, IL-6, IL-18, TNF-α), and improvement in anti-dsDNA, C4, haemostatic markers (fibrinogen, vonWillebrand factor) and disease activity scores in the treatment group compared with the placebo group. Petri et al31 investigated the effects of vitamin D in 1006 patients over 128 weeks. On a first visit, 25(OH)D levels <40 ng/mL were found in 76% of patients, of whom 85% were African American. These patients received supplementation with 50 000 units of vitamin D2 (ergocalciferol) weekly, and a modest but a significant reduction in the risk of high disease activity was observed in association with increases in 25(OH)D in the subset of patients with low levels of vitamin D at baseline.
We did not find any correlation between vitamin D level and glucocorticoid use. This finding is consistent with a recent study by Schoidre et al.21 It is thought that glucocorticoids may interfere with vitamin D absorption and higher doses of supplementation may be required to attain therapeutic levels.
We did not find any significant relationship between vitamin D and medication use. Ruiz-Irastorza et al14 found that treatment with hydroxychloroquine independently predicted a higher serum vitamin D level. In contrast, Schoindre et al21 did not find any correlation between blood hydroxychloroquine concentrations and vitamin D level. We were not able to determine any relationship between hydroxychloroquine and vitamin D level as all of our patients were taking hydroxychloroquine.
In conclusion, this study demonstrates that vitamin D deficiency is prevalent in SLE patients in the Southern Hemisphere and that low vitamin D is associated with a higher SLE disease activity and ESR. A trend towards a predictive effect of low vitamin D on subsequent disease activity was observed, but did not remain significant after adjustment for vitamin D supplementation, glucocorticoid use and immunosuppressive use. Future studies should include randomised trials which focus on the clinical effect of vitamin D supplementation in SLE and should control for variables that could affect the analysis of benefit.
Acknowledgments
We wish to thank Susan Morton for assistance with data collection.
References
Footnotes
-
Contributors KSY contributed to study design, data collection, interpretation of results and preparation of manuscript; MNo contributed to data collection, interpretation of results and preparation of manuscript; AB-YH contributed to data collection, interpretation of results and preparation of manuscript; EFM contributed to study design, data collection and interpretation of results and preparation of manuscript; MNi contributed to study design, data analysis, interpretation of results and preparation of manuscript.
-
Funding MNi is a recipient of a David Bickart Clinician Research Fellowship from the University of Melbourne Faculty of Medicine, Dentistry and Health Sciences and holds an a National Health and Medical Research Council (NHMRC) of Australia Clinical Early Career Research Fellowship (APP1071735).
-
Competing interests None.
-
Ethics approval Human Research Ethics committee of Monash Health.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.