Article Text

Statistics from Altmetric.com
Introduction
Lupus nephritis (LN) occurs in up to 60%1 of all patients with systemic lupus erythematosus (SLE) and is associated with increased mortality rates.2 Current guidelines on the treatment for LN recommend corticosteroids in combination with cyclophosphamide or mofetil mycophenolate (MMF) as induction treatment and azathioprine or MMF as maintenance treatment.3 ,4 Nevertheless, there is a persistent need for new therapeutic options since the cumulative renal flare rate is 50% within 10 years upon the first-choice conventional treatments.5 For these refractory patients, guidelines are less specific in their recommendations: Rituximab is most often recommended to be considered despite the negative results in randomised trials.6 ,7 Interestingly, no consensus was reached on the role of calcineurin inhibitors (CNIs)3 ,4 despite two recently published, large randomised controlled trials (RCTs) showing a positive signal on the efficacy of a tacrolimus (TAC)-based treatment in LN.8 ,9 Moreover, an attractive aspect of TAC is that it also can be given during pregnancy,10 ,11 which is a frequent dilemma in young women with SLE. Also, TAC is a readily available agent and commonly used in kidney transplantation. Taken together, systematically analysing the potential role of TAC as treatment for LN is necessary.
TAC is a macrolide CNI frequently used in solid organ transplantation to prevent rejection.12 Calcineurin inhibition by TAC prevents dephosphorylation of the nuclear factor of activated T cells and thereby reduces activity of genes coding interelukin 2 and related cytokines,13 leading to inhibition of T cell activation. Besides its immunosuppressive effect TAC, as well as its calcineurin-inhibiting predecessor ciclosporine, are both known for their antiproteinuric effects in treating a variety of renal pathologies.14 In an SLE mouse model,15 treatment with TAC in animals with spontaneous LN shows inhibition of the progression of glomerular hypercellularity, crescent formation, proteinuria development and suppression of serum anti-dsDNA antibody elevation. Thus, from an immunological point of view, TAC might have potential as treatment for LN.
The present study aimed to guide clinical judgement on the use of TAC in patients with LN. Therefore, we systematically reviewed all the published clinical studies that investigated a TAC regimen in LN and performed a meta-analysis on the efficacy of TAC regimens and assessed available safety parameters.
Methods
Literature search strategy and data analysis
Pubmed, Embase, Web of Science and Cochrane databases were searched for all human studies on treatment of LN with TAC. The following search terms were used: (((‘Tacrolimus’[Mesh] OR ‘tacrolimus’[tw] OR tacrolimus*[tw] OR ‘Prograf’[tw] OR ‘Prograft’[tw] OR ‘FR-900506’[tw] OR ‘FR 900506’[tw] OR ‘FR900506’[tw] OR ‘FK-506’[tw] OR ‘FK 506’[tw] OR ‘FK506’[tw] OR ‘WM0H WNM’[all fields]) AND (‘Nephritis’[Mesh] OR ‘nephritis’[tw] OR nephrit*[tw] OR ‘Glomerulonephritis’[tw] OR ‘Anti-Glomerular Basement Membrane Disease’[tw] OR ‘Glomerulosclerosis’[tw] OR ‘Balkan Nephropathy’[tw] OR ‘Pyelonephritis’[tw] OR ‘Pyelitis’[tw] OR ‘Pyelocystitis’[tw]) AND (‘Lupus Erythematosus, Systemic’[Mesh] OR ‘Systemic Lupus Erythematosus’[tw] OR ‘SLE’[tw] OR ‘lupus’[tw])) OR ((‘Tacrolimus’[Mesh] OR ‘tacrolimus’[tw] OR tacrolimus*[tw] OR ‘Prograf’[tw] OR ‘Prograft’[tw] OR ‘FR-900506’[tw] OR ‘FR 900506’[tw] OR ‘FR900506’[tw] OR ‘FK-506’[tw] OR ‘FK 506’[tw] OR ‘FK506’[tw] OR ‘WM0H WNM’[all fields]) AND (‘Lupus Nephritis’[Mesh] OR ‘Lupus Nephritis’[tw] OR ‘Lupus Glomerulonephritis’[tw]))) AND (‘Clinical Trial’[publication type] OR random*[tw] OR ‘trial’[tw] OR ‘RCT’[tw] OR placebo*[tw] OR ‘double blind’[tw]). According to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria,16 titles and abstracts of search results were evaluated for suitability based on the following criteria: (1) published as a clinical trial in human subjects; (2) included patients had an established diagnosis of SLE in accordance with the American College of Rheumatology revised criteria; (3) the presence of LN and persistent clinical findings such as elevated serum creatine, proteinuria >0.5 g or active urine sediment; (4) for controlled studies: well defined renal complete, partial and non-response criteria. The studies were judged and selected independently by two investigators (TK and YKOT). Consensus was achieved on studies that were selected by only one of two investigators.
All studies were labelled according to their design, that is: ‘case series’ when 10 or less patients were reported, ‘uncontrolled cohort’ when more than 10 patients were studied, ‘case-control study’ (CCS) or ‘randomised controlled trial’ (RCT). Study characteristics were summarised by descriptive statistics and ordered on the basis of type and goal of TAC treatment leading to four categories: (1) studies applying a TAC regimen as induction treatment for new LN or flare of LN; (2) studies applying a TAC regimen as maintenance treatment for patients with LN who had received any given induction treatment; (3) studies applying a TAC regimen applied as induction treatment and followed by (lower dosages of) TAC as maintenance treatment; (4) studies switching conventional treatment to a TAC regimen during the maintenance phase. The quality of randomised controlled trials was assessed with the Delphi list.17
From all controlled studies relevant variables were extracted, that is, baseline characteristics, trial design characteristics, TAC regimen characteristics, renal responses, dropouts and adverse events. With respect to renal response criteria, the definitions for complete, partial and no response were adapted from the individual studies.
Statistical analysis
Descriptive statistics were used to summarise baseline, trial and TAC regimen characteristics. Data from five RCTs were used in a meta-analysis, to compare renal response and adverse events between TAC-based regimens and control therapy. The meta-analysis was performed with Stata, V.10 (Statacorp, Texas, USA). The relative risk (RR) and 95% CI for each outcome was calculated for each study using the Mantel-Haenszel fixed- effects model. Heterogeneity was determined by the χ2 and I2 tests. An outcome of p<0.05 was considered a significant difference.
Results
Summary of the literature search
Our search strategy resulted in 239 articles of which 23 relevant clinical studies were selected based upon the predefined quality criteria (figure 1). As depicted in table 1, we found that the majority of clinical studies consisted of uncontrolled case series (26%) and uncontrolled cohort studies (39%). Controlled studies encompassed 2 (9%) CCS and 6 (26%) RCTs. From all selected studies, 87% were exclusively performed in Asian LN populations, leaving 3 (13%) uncontrolled studies in non-Asian patients. The most frequently studied TAC regimen combined TAC with steroids (65%), also termed ‘duo therapy’. Six (26%) studies combined TAC with steroids plus MMF, also termed ‘triple therapy’. A majority of 13 (57%) studies investigated TAC as induction treatment, 5 (22%) as maintenance treatment, 3 (13%) used TAC as induction and subsequent maintenance treatment and 2 (9%) studies investigated a switch of conventional maintenance to a TAC maintenance regimen.
Summary of study characteristics

Flow chart of the literature search. LN, lupus nephritis; RCT, randomised controlled trial.
Table 2 summarises the controlled studies grouped by treatment goal and on the basis of their treatment regimen. This overview illustrates the heterogeneity of the published studies.
Number of studies stratified by treatment intention
To better understand the studied TAC regimens in the controlled studies, the quality score (only applicable in RCT), study designs and TAC dosing were summarised in table 3. Overall, the quality of studies was poor to average (median score 4, range 3–5) as measured by the standardised Delphi scoring for RCTs. Importantly, one shared characteristic was that all studies investigating induction treatment with TAC regimens defined their renal response end point at 6 months. The definition of renal response, however, was different for each study (see online supplementary table S2). With respect to dosing, we could not find any coherence between any of the studies nor within studies investigating duo therapy or triple therapy TAC regimens. Seven (88%) studies measured TAC trough levels to guide their dosing, however target trough levels varied per study (table 3).
supplementary tables
Overview of the studies fulfilling the predefined selection criteria for analysis of tacrolimus-based regimens in patients with lupus nephritis
Patient characteristics
Overall, 693 patients were included in the meta-analysis on renal response and most frequently reported adverse events. Patient characteristics were summarised in table 4. In short, 90% of the subjects were female. The mean age was 32 years and 100% were of Asian ethnicity. Histopathologically, 84% had an LN class III/IV±V and 16% LN class V.
Baseline characteristics of patients with LN from the selected RCTs that are used in the meta-analysis for renal response and adverse events
Of note, for non-Asian subjects we did not find any controlled trials. Two case series24 ,25 and one uncontrolled cohort study26 with a total of 32 patients using TAC regimens have been published and none met the selection criteria.
Meta-analysis of renal responses upon induction treatment with TAC-based regimens
The results of the meta-analysis are shown in figure 2. Five RCTs investigated TAC regimens in the induction treatment phase and were used for data extraction. Again, all studies reported renal response rate as a primary end point at 6 months. Three RCTs used intravenous cyclophosphamide in the control arm,9 ,18 ,20 one study mycophenolate8 and one study19 contained two control arms using either mycophenolate or cyclophosphamide. TAC-based induction treatment led to a significantly higher total renal response (RR 1.23, 95% CI 1.12 to 1.34, p<0.05) with significantly higher complete renal response (RR 1.48, 95% CI 1.23 to 1.77, p<0.05) and equivalent partial renal response (RR 0.98, 95% CI 0.79 to 1.21, p=not significant (NS)). The RR for total, complete and partial response was also assessed for studies using duo therapy and triple therapy separately. In RCTs using duo therapy, TAC-based induction treatment led to equivalent total renal response (RR 1.06, 95% CI 0.94 to 1.19, p=NS) with equivalent complete renal responders (RR 1.15, 95% CI 0.92 to 1.44, p=NS) as well as partial responders (RR 0.91, 95% CI 0.62 to 1.34, p=NS). For RCTs using triple therapy, TAC-based induction treatment led to a significantly higher total renal response (RR 1.37, 95% CI 1.21 to 1.56, p<0.05), with more complete responders (RR 1.94, 95% CI 1.45 to 2.61, p<0.05), and equivalent partial responders (RR 1.01, 95% CI 0.78 to 1.31, p=NS).

Forest plots of the relative risks (RRs) and 95% CIs of the total (complete plus partial), complete and partial renal response rates in the selected randomised controlled trials (RCTs) upon induction tacrolimus-based treatment versus conventional treatment. A fixed-effects meta-analysis was performed. The meta-analysis was performed for studies using duo therapy (adapted from Mok et al [8], Chen et al [18], Li et al [19]) and for studies using triple therapy (adapted from Liu et al [9], Bao et al [20]) separately as well. The vertical solid line represents an RR of 1 and the dotted line illustrates the overall RR. The p value of the test for heterogeneity is shown for subtotal and overall analyses.
Renal responses upon maintenance treatment with TAC and steroids
Only one study21 met our quality criteria to evaluate the effect of maintenance treatment with a TAC regimen. This study reported an equivalent response of 100% vs 95% to TAC versus control treatment after 6 months: 56% achieved a complete remission (19 out of 34) and 44% achieved a partial remission (15 out of 34). No flares were observed during this period. In the control group, where patients received azathioprine, 64% achieved complete remission (23 out of 36) and 31% a partial remission (11 out of 36). Two flares were observed in the control arm.
Meta-analysis of adverse events upon induction treatment with TAC and steroids
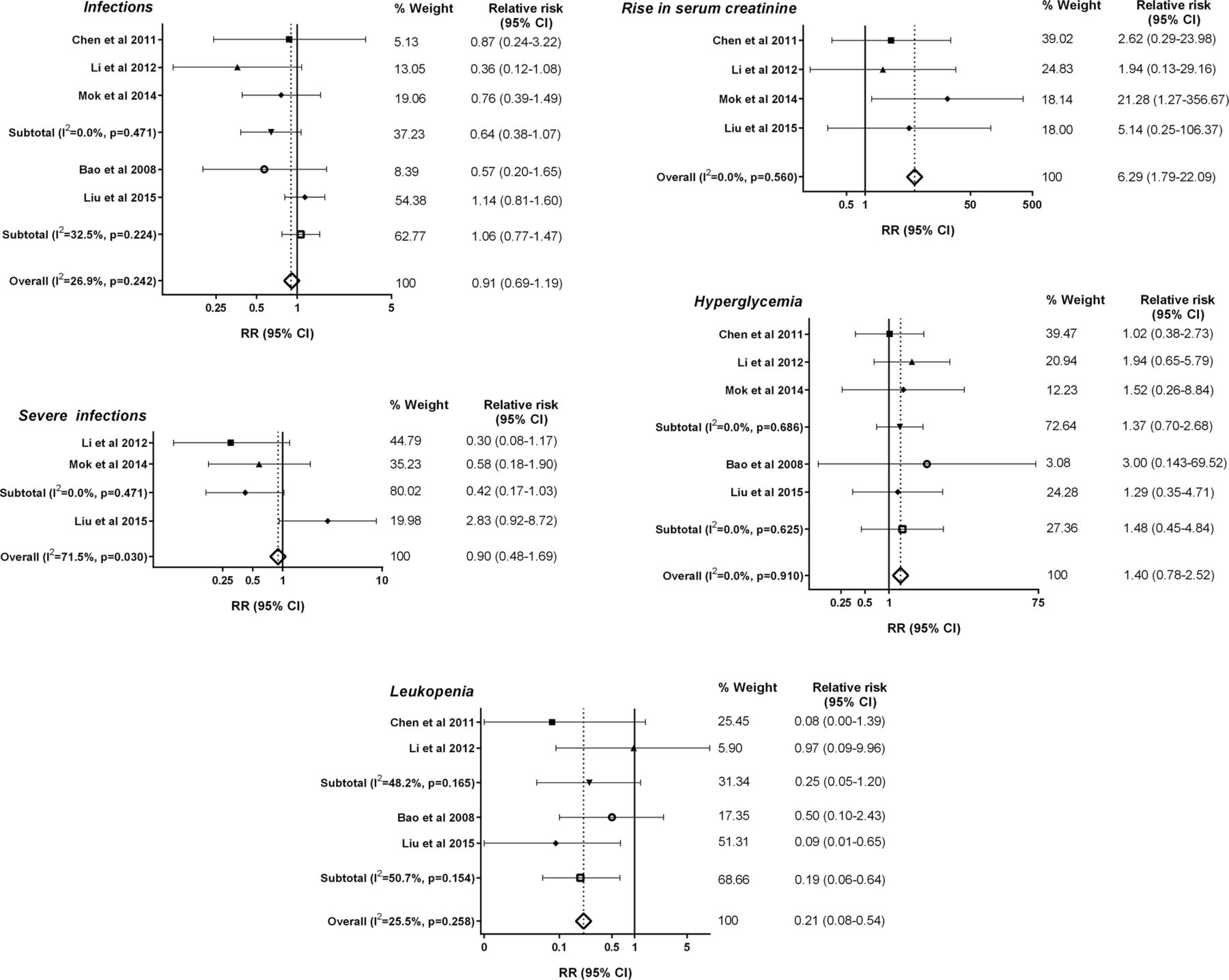
From the five RCTs investigating TAC regimens in the induction phase, the most frequently reported adverse events were included for meta-analysis (figure 3). Leucopoenia was significantly less reported in the TAC-based treatment group (RR 0.21, 95% CI 0.08 to 0.54, p<0.05). A rise of serum creatine was higher in the TAC-based treatment group (RR 6.29, 95% CI 1.79 to 22.09, p<0.05). Infectious complications were comparable between the TAC-based treatment group and control group (RR 0.91, 95% CI 0.69 to 1.19, p=NS). Although severe infections (RR 0.90, 95% CI 0.48 to 1.69, p=NS) and hyperglycaemia (RR 1.40, 95% CI 0.78 to 2.52, p=NS) were more often reported in the TAC-based treatment group, these results did not reach statistical significance. Relative risks for the most reported adverse events were also compared between duo therapy and triple therapy separately. Overall, results between studies using duo therapy or triple therapy did not differ. Importantly, the TAC-based treatment in the RCTs using duo therapy showed a lower, non-significant rate for severe infection (RR 0.42, 95% CI 0.17 to 1.03, p=NS), whereas a trend to a higher rate of severe infections was seen with triple therapy (RR 2.83, 95% CI 0.92 to 8.72, p=NS).
{kind=link}
{kind=link}
{kind=link}
Forest plots of the relative risks (RRs) and 95% CIs for the five most commonly reported adverse events in the selected randomised controlled trials (RCTs) on tacrolimus-based treatment versus conventional treatment. Overall infections, severe infections, hyperglycaemia, leucopoenia and rise in serum creatine were used in a meta-analysis, using a fixed-effects model. For infections, hyperglycaemia and leucopoenia, a meta-analysis was performed for studies using duo therapy (adapted from Mok et al [8], Chen et al [18], Li et al [19]) and for studies using triple therapy (adapted from Liu et al [9], Bao et al [20]) separately as well. The vertical solid line represents an RR of 1 and the dotted line illustrates the overall RR. The p value of the test for heterogeneity is shown for subtotal and overall analyses.
Discussion
The present study was performed to better guide clinical judgement on the use of TAC in patients with LN. Selecting only the highest quality studies for meta-analysing the clinical efficacy of TAC-based regimen, we demonstrated that the currently available studies are predominantly non-randomised, uncontrolled studies. Our systematic meta-analysis of randomised trials comparing TAC-based regimens with conventional treatment demonstrated superior efficacy in Asian patients with LN, mainly determined by studies evaluating triple therapy.9 ,20 Safety profiles of TAC-based regimens were comparable to conventional treatment. These results cannot be extrapolated to the general LN population. Therefore, taken all together, current evidence supports the use of TAC-based regimens in a selected group of patients with LN of Asian ethnicity with a preference for using triple therapy (TAC, MMF and steroids) as induction treatment. The latter said, long-term safety of TAC-based regimens is not established.
The goal of this study was to translate published study results on TAC in LN to current clinical practice. Based on our study and previous meta-analyses27 ,28 there is level 1A evidence29 to support the clinical efficacy of TAC in the subgroup of Asian patients with LN. However, our study illustrated that a ‘grade A’ recommendation for TAC is hampered by the heterogeneity of TAC-based regimens studied in this subgroup of patients with LN. In this view it is important to note that the positive result of our meta-analysis was predominantly determined by the study of Liu et al9 that investigated a TAC-based regimen using ‘triple’ therapy combining steroids, mycophenolate and TAC. Altogether, it is self-evident that a randomised, multiethnic study is mandatory to further expand our knowledge and evidence of TAC treatment in LN.
To further guide clinicians in the use of TAC, it is reasonable to extrapolate the level 1A evidence (see online supplementary table S1) described above to the subgroup of refractory patients with LN. Generally, refractory LN is defined as a failure on two conventional treatments (being either mycophenolate or cyclophosphamide).3 ,4 ,30 Several treatment suggestions are made in LN treatment guidelines for refractory LN such as rituximab, CNIs, intravenous immunoglobulins, plasmapheresis and tumor necrosis factor (TNF) blockade.31 Thus, with respect to TAC, a grade B positive recommendation can be formulated. Our data at the least suggest that the use of TAC is not inferior to conventional treatment. Moreover, we and others27 ,28 ,32 showed that the safety profile of TAC is very good in LN. Therefore, we would recommend TAC to be considered as a treatment option in patients with refractory LN.
TAC is a safe drug during pregnancy and its continuation is commonly recommended in the setting of pregnant patients who have received solid organ transplantation.10 ,33–35 From this perspective, the level 1A evidence on the efficacy of TAC in Asian patients with LN should also be considered for extrapolation to this special subgroup of patients with LN. Although TAC is non-teratogenic, there is an increased risk of gestational diabetes and hypertension.36 Currently, there are no controlled studies available investigating TAC for LN in pregnant patients. In a case series on nine patients with LN,33 TAC was successfully used to maintain remission in three patients and to treat a lupus flare in six patients. All pregnancies resulted in live births with birth weights according to gestational age and no congenital abnormalities. At present, azathioprine is considered the first choice of treatment in pregnant patients with LN.37 However, in those patients with LN who are azathioprine-resistant or azathioprine-intolerant, TAC can be considered as a treatment option.
CNIs were studied in LN before. Early exploratory studies on the efficacy of ciclosporine in LN resulted in comparable efficacy to conventional treatments, at the cost of unacceptably higher adverse events rates.38 However, a small RCT in 40 patients (Cyclofa-Lune trial)39 demonstrated that after approximately 8 years of follow-up, ciclosporine was non-inferior to high-dose cyclophosphamide as induction treatment for proliferative LN. A second RCT40 in class V membranous LN, showed faster remission with ciclosporine compared with cyclophosphamide with comparable remission rates. Long-term follow-up of 5 years showed increased relapse rates in the ciclosporine treated arm. Only one study that investigated ciclosporine as maintenance therapy observed equal efficacy to azathioprine in preventing disease flares.41 On a histopathological level, ciclosporine was unable to reduce chronic activity in lupus kidney biopsies, supporting the hypothesis that the antiproteinuric effects of ciclosporine were predominantly attributable to haemodynamic rather than immunological changes.42 We know from the vast literature on transplantation that ciclosporine and TAC are different with respect to immunological efficacy as well as safety profile. Ciclosporine binds cyclophilin while TAC binds FK506, resulting in different immunosuppressive effects.43 Furthermore, both ciclosporine and TAC have small therapeutic widths, causing small variations in dosing to potentially imply large differences in efficacy and toxicity. Therefore, irrespective of the available data on ciclosporine, further investigations into the efficacy of TAC on clinical as well as histopathological end points are clearly warranted.
There are important limitations to consider in the present meta-analysis. First, the quality of the controlled studies was low as defined by the Delphi score, mainly because of the incomplete blinding procedures in all studies. Second, as mentioned before, from five RCTs the largest RCT performed by Liu et al9 determined 49% of the overall total response. Third, TAC regimens were heterogeneous across all studies: target trough levels varied or were not used and also concomitant steroid dosing differed (see online supplementary table S2). This notion hampers a general recommendation on the optimal dosing of TAC. Fourth, no long-term results could be investigated in this meta-analysis. Only one study8 reported long-term results (ie, 5 years of follow-up) after induction treatment with TAC and prednisone during 6 months followed by azathioprine and prednisone as maintenance treatment. Of note, a higher rate of renal relapses was observed in the TAC-based treatment arm, which did not reach statistical significance (p=0.13). Lastly, it needs to be emphasised that all included studies were performed in Asian patients. The importance of ethnicity has been demonstrated by the ethnicity-based subgroup analysis of the Aspreva Lupus Management Study (ALMS) trial.44 Superiority of mycophenolate over cyclophosphamide was predominantly determined by its efficacy in African-American and Hispanic patients. In addition, genome-wide association studies revealed different genetic susceptibility loci for SLE between ethnicity groups.45 Also, the CYP3A5 polymorphism determines the metabolism of TAC, and a lower bioavailability of TAC in African-American kidney transplant recipients46 ,47 is well described. Altogether emphasising that the extrapolation of these data to other ethnic groups is not self-evident. Of note, we found only three non-controlled case series treating non-Asian subjects with TAC-based regimens.24–26 Despite these limitations, this comprehensive analysis of all published studies illustrated that TAC-based therapy in selected patients with LN can be efficacious without major safety concerns. Therefore, these data emphasise the importance to further investigate the efficacy of TAC for patients with active LN.
Indeed, the international Lupus Trial Nephritis Network has recently initiated the design of a trial with a TAC-based regimen. In this respect a few considerations could be deducted from our current study. Based on the efficacy results in our meta-analysis, it would be plausible to investigate triple therapy randomising a multiethnic patient population with LN. Regarding safety of such an RCT, a possible higher risk for severe infections in the triple therapy arm needs to be monitored closely. The general dosing in a TAC regimen is roughly estimated at 3–4 mg twice daily during the induction phase, based on the summary of studies. Monitoring of trough levels is not mandatory although it can help to exclude low exposition in patients. Most importantly, the definition of the primary renal end point needs much attention: due to the haemodynamic effects of TAC on reducing proteinuria, as discussed above, the classic LN renal end point which is mainly based on proteinuria improvement is intrinsically biased. Briefly, patients with LN with TAC have a quick reduction of proteinuria within the first weeks of treatment (most probably due to haemodynamic effects) and therefore empirically a higher chance of achieving a partial or even complete response. Also in the current meta-analysis, we could not exclude whether a haemodynamic effect is (partly) responsible for the positive effects of TAC regimens. While a haemodynamic effect is undoubtedly present, it seems unlikely that this effect could fully explain the beneficial effect of TAC-based therapies. Thus, it seems wise to consider a less biased renal end point such as a repeat renal biopsy. Although timing of this renal biopsy needs careful consideration, it would confirm treatment efficacy in a more objective manner plus help to identify whether, if any, there is a risk for CNI toxicity on the renal tissue level. Of note, it is important to take into account that all included studies in this study used proteinuria as an important remission criterion (see online supplementary table S2). Taking these considerations into account, a multicentre, international RCT defining the role of TAC in LN treatment should be feasible and eagerly embraced by the scientific community.
In conclusion, we recommend the use of a TAC-based regimen in the selected group of Asian patients with LN. In addition, we recommend considering a TAC-based regimen in the subgroups of patients with refractory LN and (pre)pregnant patients with LN. Although long-term efficacy and safety results are lacking, it seems reasonable to conclude that when patients with LN are to be treated with TAC, this strategy seems not to be inferior to conventional treatment and has a good safety profile. In the future, the place of TAC in the therapeutic armamentarium for LN can only be established when a multicentre, international RCT is performed as now proposed by the international Lupus Nephritis Trial Network.
Acknowledgments
The authors thank J Schoones for his advice and support with the literature search. The authors also thank Professor Dr O M Dekkers for independently reviewing statistical analysis.
References
Footnotes
↵Dr Craen died on January 17th, 2016.
Contributors TK, TJR, YKOT contributed to the ideas for the article. YKOT performed the literature search. TK, AJMC, ST and YKOT contributed to data acquisition and analysis. TK, OWB, ST, TWJH, TJR and YKOT contributed to the writing of the manuscript. YKOT is the guarantor.
Funding The work of TK and YKOT was supported by the Dutch Kidney Foundation (KJPB12.028) and a Clinical Fellowship by the Dutch Organisation for Scientific Research.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.