Article Text

Abstract
Background Most clinical trials of new treatments for systemic lupus erythematosus (SLE) have shown weak discrimination between investigational agents and placebo when added to standard of care (SOC). The design of future SLE trials may be improved by considering strategies for reducing placebo response rates and better understanding the within-patient variability in disease activity during follow- up. We evaluated longitudinal patterns of response in SLE patients who received placebo plus SOC in two completed 52-week clinical trials. Baseline characteristics that discriminated persistent responders from non-responders were also examined, with the goal of identifying characteristics that may define patient populations with unmet medical need who should be targeted for enrollment in future trials
Materials and methods Data was obtained from the Collective Data Analysis Initiative (CDAI) of the Lupus Foundation of America and included 147 patients from the placebo plus SOC arms of two randomised Phase II/III trials in moderately-to-severely active lupus patients without acute nephritis. BILAG-based response was evaluated at weeks 12, 24, 36, 48, and 52. Both cross-sectional and longitudinal analyses of response rates were performed. Baseline clinical variables that discriminated persistent responders and non-responders were identified using logistic regression.
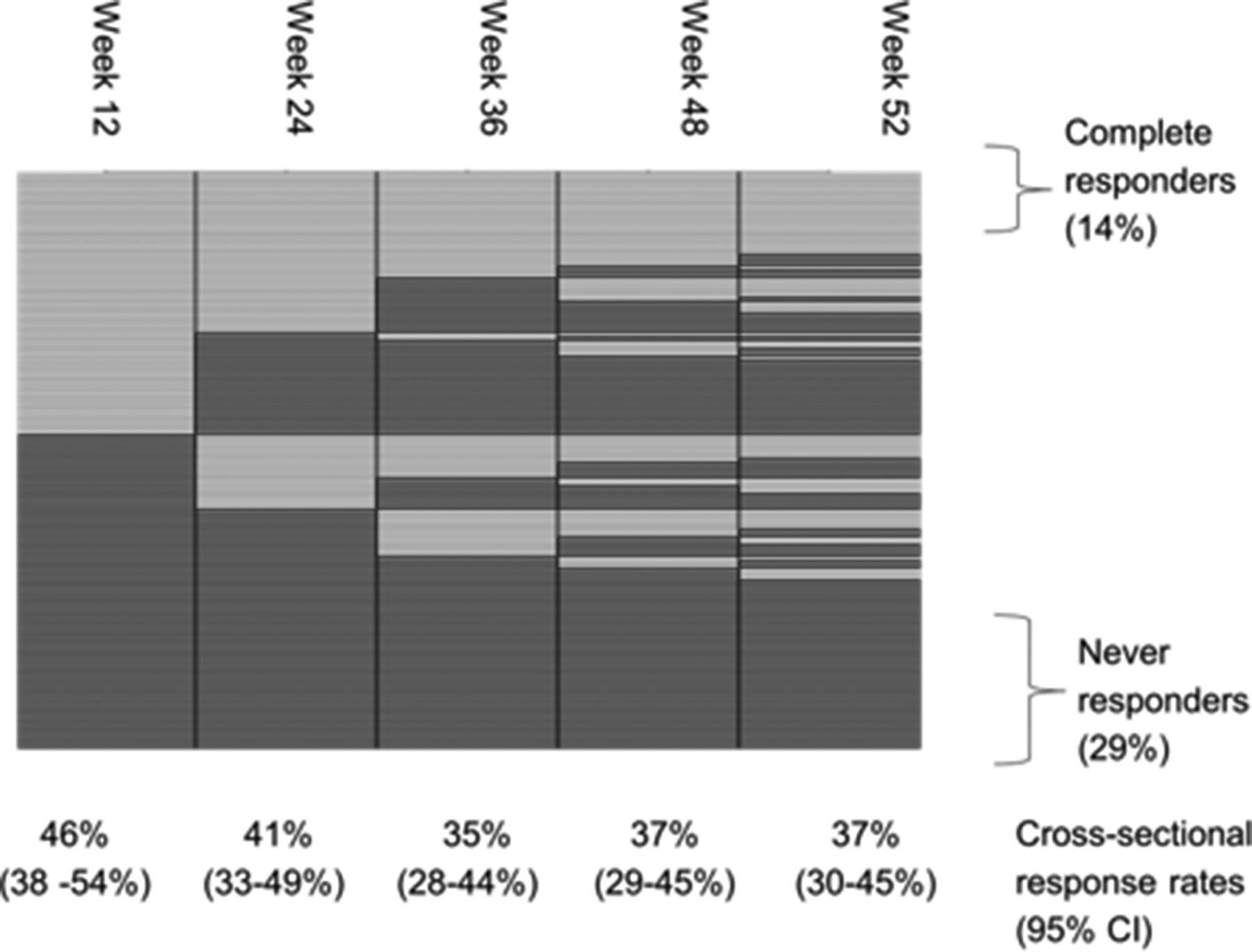
Results Cross-sectional response rates for patients treated with placebo plus SOC decreased from 46% to 37% between 12–52 weeks (Figure 1). The rate of complete and sustained response, i.e., response at all visits between 12–52 weeks, was only 14.3% (95% CI: 8.6%–19.9%). Agreement between response status at 12 weeks and 36–52 weeks was low (kappa = 0.15–0.25); furthermore only 31% of initial 12 week responders maintained response at all subsequent visits. Baseline factors contributing to persistent response to SOC included fewer active organ systems, high C3 levels, and type of background therapy.
Conclusions An endpoint based on a sustained rather than landmark response may reduce high placebo response rates in SLE trials that continue aggressive SOC. Further exploration to assess the power of this endpoint to improve discrimination between active and placebo arms is indicated. The observed lack of stability in response to SOC over time highlights a potential weakness with shorter studies that use an endpoint of improvement. Our data also confirm earlier reports that the likelihood of response in the placebo group depends on the severity of disease and the aggressiveness of background treatments.

{kind=link}
Temporal patterns in response status (Light = Response; Dark = No Response)
Acknowledgements Lupus Foundation of America Collective Data Analysis Initiative Group.