Article Text

Abstract
Objective To evaluate hypogammaglobulinaemia and risk of serious infectious adverse events in active lupus nephritis.
Methods The Abatacept and Cyclophosphamide Combination Efficacy and Safety Study (ACCESS) compared abatacept with placebo in participants with lupus nephritis undergoing treatment with Euro-Lupus Nephritis low-dose cyclophosphamide. Serum IgG levels were assessed prior to initiation of treatment and throughout the trial. Hypogammaglobulinaemia was defined as IgG <450 mg/dL.
Results Hypogammaglobulinaemia was observed in 16/102 (15.7%) participants prior to initiation of induction therapy for active lupus nephritis. Participants with nephrotic range proteinuria were more likely to have hypogammaglobulinaemia, and serum IgG levels were inversely correlated with urine protein to creatinine ratio (r=−0.42, p<0.0001). Following initiation of treatment for active lupus nephritis, additional participants developed hypogammaglobulinaemia by weeks 2–4. Serum IgG levels then increased, and all but one participant had serum IgG ≥450 mg/dL at 24 weeks. Hypogammaglobulinaemia was not associated with an increased risk of serious infectious adverse events.
Conclusions In active lupus nephritis in ACCESS, hypogammaglobulinaemia was common and inversely correlated with proteinuria. Serum IgG levels were lowest in the weeks immediately following initiation of induction therapy, and subsequently improved by 24 weeks. Hypogammaglobulinaemia was not associated with serious infectious adverse events.
- Cyclophosphamide
- Infections
- Lupus Nephritis
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
Reduced serum IgG has been reported in lupus nephritis (LN)1 2; however, levels are not routinely measured, and the prevalence of hypogammaglobulinaemia in active LN is not known. Persistent trough levels of IgG below 400 mg/dL in common variable immunodeficiency and X linked agammaglobulinaemia have been associated with increased risk of infection, pneumonia in particular,3 but there is little evidence that hypogammaglobulinaemia in active LN confers a similar risk. However, a phase II/III trial with atacicept in LN was halted after enrolment of six participants, when severe infections occurred in two participants with hypogammaglobulinaemia.4 Therefore, evaluation of serum IgG levels during treatment for active LN was undertaken in the Abatacept and Cyclophosphamide Combination Efficacy and Safety Study (ACCESS)5 to evaluate the relationship of serum IgG levels to serious infectious adverse events (SIAEs).
Patients and methods
Study treatment
Details of ACCESS have been previously described.5 Briefly, ACCESS was a multicentre randomised controlled trial of abatacept compared with placebo in 134 participants with LN who underwent treatment with the Euro-Lupus Nephritis (ELN) low-dose cyclophosphamide regimen6 followed by azathioprine maintenance therapy. Participants also received prednisone. ACCESS, registered as NCT00774852, received institutional review or ethics board approval at each site, and was conducted in accordance with the International Conference on Harmonisation Guidelines for Good Clinical Practice and the Declaration of Helsinki.
Assessments
Quantitative serum IgG assessments were instituted after the initiation of ACCESS, and were assessed at the screening visit and at weeks 0, 2, 4, 12, 24 and 52. Hypogammaglobulinaemia was defined as serum IgG <450 mg/dL since serum IgG was expected to decline in the setting of LN treatment, and the risk for infection in immunodeficiency syndromes is associated with serum IgG <400 mg/dL.3 Nephrotic range proteinuria was defined as urinary protein ≥3.5 g in a 24-hour urine collection. Adverse events (AEs) were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events v3.0 (NCI CTCAE v3.0).
Statistical methods
Comparisons of categorical variables were performed using a Χ2 test or a Fisher exact test depending on the cell sizes. Comparisons of continuous variables were performed using a Wilcoxon rank-sum test. Pearson’s correlation coefficient was calculated to determine associations between IgG level and urine protein to creatinine ratio (UPCR). All statistical tests were two-sided.
Results
Hypogammaglobulinaemia in active LN correlated with proteinuria
In ACCESS, 134 participants were treated for active LN with the ELN cyclophosphamide induction regimen and prednisone, in combination with abatacept or placebo. Serum IgG levels were examined beginning at the screening visit in 102 participants. Hypogammaglobulinaemia was observed in 16/102 (15.7%) participants prior to induction therapy. Four participants had serum IgG <300 mg/dL, and the lowest level of IgG observed prior to induction therapy was 170 mg/dL. Table 1 shows the characteristics of 16 participants with IgG <450 mg/dL prior to induction therapy, compared with 86 participants with IgG ≥450 mg/dL prior to induction therapy.
Characteristics of participants with hypogammaglobulinaemia prior to induction therapy for lupus nephritis
Gender, age, race and ethnicity did not significantly differ between the two groups, nor did the proportion of participants with total lymphocyte counts <1000/µL. Mycophenolate mofetil and corticosteroid usage in the 30 days prior to enrolment was not significantly different. Participants did not receive cyclophosphamide or rituximab in the year prior to enrolment, or belimumab in the 6 months prior to enrolment.
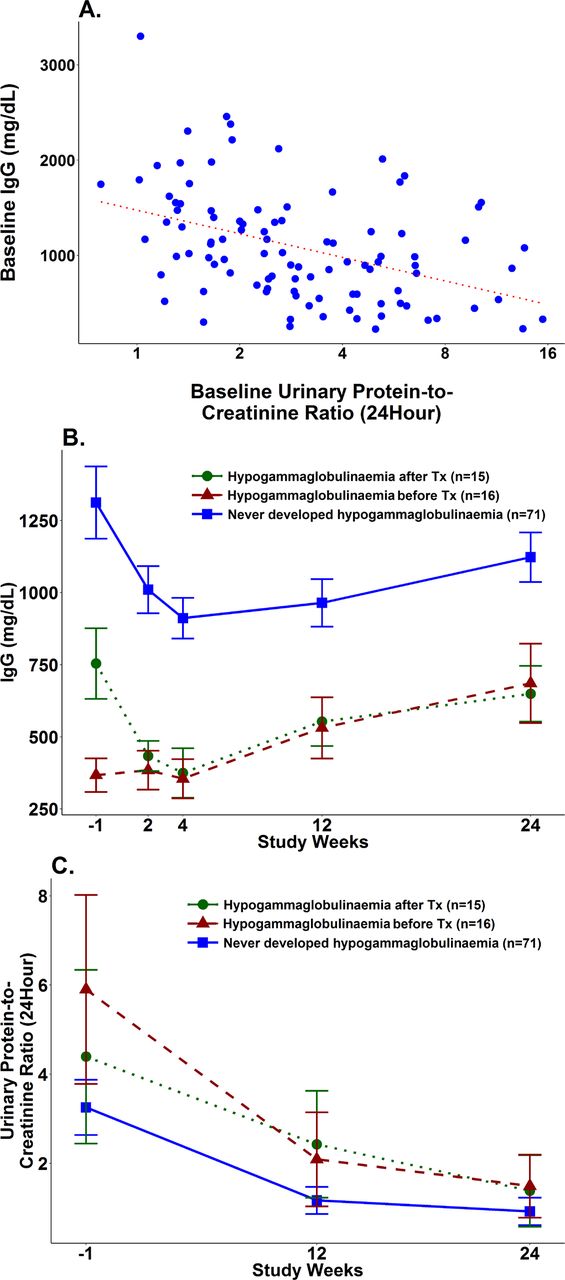
In contrast, participants with low serum IgG level prior to induction therapy were significantly more likely to have nephrotic range proteinuria compared with participants without low serum IgG (p<0.01, table 1). Hypogammaglobulinaemia was observed in 13/44 (30%) participants with nephrotic range proteinuria ≥3.5 g prior to induction therapy, compared with 3/58 (5%) without nephrotic range proteinuria. Hypogammaglobulinaemia prior to induction therapy was observed most frequently in the setting of high levels of proteinuria, occurring in 5/12 (42%) participants with proteinuria >8.0 g and in 3/4 (75%) participants with proteinuria >14 g in a 24-hour collection. Pearson’s correlation analysis showed an inverse correlation between IgG level and UPCR in a 24-hour collection (r=−0.42, p<0.0001, figure 1A). Low serum IgG prior to induction therapy was also associated with LN duration ≥12 months (p=0.04, table 1).
{kind=link}
(A) Correlation between serum IgG and UPCR in a 24-hour collection. (B) Serum IgG levels before, during and after Tx. (C) UPCR in a 24-hour collection before, during and after Tx. Tx, induction therapy; UPCR, urine protein to creatinine ratio.
Serum IgG levels initially decreased following treatment for active LN, then increased by 24 weeks
Low serum IgG levels prior to induction therapy remained low during the initial few weeks of treatment. Furthermore, serum IgG levels decreased following induction therapy in participants without hypogammaglobulinaemia prior to treatment (figure 1B). Fifteen additional participants developed hypogammaglobulinaemia following initiation of induction therapy, including five who developed IgG <300 mg/dL. Thus, hypogammaglobulinaemia was observed in a total of 31/102 (30.4%) participants, either prior to treatment or in the weeks immediately following treatment initiation, while 71/102 (69.6%) never developed hypogammaglobulinaemia. Similar proportions of participants with hypogammaglobulinaemia were observed in the abatacept group and the placebo group (data not shown).
Serum IgG levels tended to be lowest at week 2 or week 4, and then increased by week 12, whether hypogammaglobulinaemia was present prior to treatment, developed after treatment or never occurred (figure 1B). At study week 24, hypogammaglobulinaemia resolved to IgG ≥450 mg/dL in nearly all participants remaining in the study, corresponding to overall improvement in UPCR in all groups (figure 1C). Only one participant had residual low serum IgG of 380 mg/dL at week 24 and also had a poor renal response to therapy. At study week 52, all participants remaining in the study had serum IgG ≥450 mg/dL (data not shown).
Hypogammaglobulinaemia was not associated with SIAEs
Eleven SIAEs occurred in nine participants during the 24 weeks of treatment (table 2).
Serious infectious adverse events during the first 24 weeks of the ACCESS trial
Infectious AEs were considered serious if they were grade 3 or higher (according to the NCI CTCAE v3.0), or if the event resulted in or extended hospitalisation. SIAEs occurred in 3/31 participants who developed hypogammaglobulinaemia during the study, compared with 6/71 participants without hypogammaglobulinaemia (9.7% vs 8.4%). None of the SIAEs occurred in participants with hypogammaglobulinaemia at screening.
Of the 11 SIAEs that occurred, at least 6 were bacterial in nature. Cellulitis occurred the day following the first dose of study medication in one participant with IgG 630 mg/dL at the screening visit, who later developed IgG 431 mg/dL at week 4. The other bacterial infections occurred in participants in whom hypogammaglobulinaemia was never observed (table 2). No participants with hypogammaglobulinaemia withdrew from ACCESS due to an infectious AE. One participant with IgG 270 mg/dL at week 4 was withdrawn from the study and received intravenous immunoglobulin at the discretion of the site investigator, but no infectious AE occurred.
Discussion
In 102 ACCESS participants with LN, hypogammaglobulinaemia was observed in nearly a third but was not associated with an increase in serious bacterial or other infections. Serum IgG correlated inversely with UPCR in a 24-hour collection, and participants with nephrotic range proteinuria were more likely to have serum IgG <450 mg/dL prior to initiation of induction therapy. Furthermore, hypogammaglobulinaemia resolved with treatment of the active LN in all but one participant.
Factors other than urinary loss likely contribute to low serum IgG in active LN. Hypogammaglobulinaemia was significantly more common in participants with LN of ≥12 months’ duration. Certain medications, including corticosteroids, are reported to cause secondary hypogammaglobulinaemia.7 8 In ACCESS, recent treatment with corticosteroids or mycophenolate mofetil in the prior 30 days was not associated with hypogammaglobulinaemia at study entry. However, serum IgG levels dropped following induction therapy with low-dose cyclophosphamide and prednisone, and then gradually rose, such that hypogammaglobulinaemia resolved in nearly all participants by 24 weeks. A similar result was observed in another study of IgG levels in LN, in participants treated with methylprednisolone and mycophenolate mofetil.2
Persistent hypogammaglobulinaemia in common variable immunodeficiency and X linked agammaglobulinaemia is associated with risk for serious infections.3 Sustained very low levels of IgG <100 mg/dL are associated with the highest risk, while transient or less severe hypogammaglobulinaemia is tolerated in most subjects.7 Transient hypogammaglobulinaemia is also generally well-tolerated in the setting of autoimmune disease.8 A retrospective study of rituximab-associated hypogammaglobulinaemia in multisystem autoimmune disease showed that hypogammaglobulinaemia occurred in 56% of 243 subjects treated with rituximab, and IgG replacement was undertaken in only 4.2% of subjects due to recurrent infection.9 10 In contrast, recurrent infections have been associated with hypogammaglobulinaemia in smaller vasculitis series,11 12 and a phase II/III trial with atacicept in LN was halted when severe infections occurred in the setting of hypogammaglobulinaemia.4
The ACCESS results demonstrate that hypogammaglobulinaemia in active LN is common, transient and well-tolerated. Most participants with hypogammaglobulinaemia in ACCESS did not develop serious infections, although a small increased risk of infection might not have been detected. The results are consistent with intact production of IgG despite urinary loss, and the adequate humoral response to vaccination observed in SLE.13
A number of factors can contribute to hypogammaglobulinaemia in LN, including proteinuria, corticosteroids and other immunosuppressive medications. Comorbid common variable immunodeficiency can also occur.14 15 Although these other factors should be considered, treatment of LN with induction therapy should not be delayed due to hypogammaglobulinaemia alone, and in ACCESS induction therapy for LN was followed by resolution of hypogammaglobulinaemia in nearly all participants. The ACCESS results do not support routine prophylactic treatment with replacement immunoglobulin for transient asymptomatic hypogammaglobulinaemia that occurs in LN, nor do they support exclusion of participants with hypogammaglobulinaemia from LN clinical trials. Nevertheless, vigilance is required for serious or recurrent infections in LN, and for comorbid common variable immunodeficiency.
Acknowledgments
The authors wish to thank the ACCESS Trial Group and the ACCESS participants. They also wish to thank their colleagues at the Immune Tolerance Network and the Lupus Nephritis Trials Network for their collaboration and intellectual contributions.
References
Footnotes
Contributors DES, LD, SGM, BD and DW designed the study. LD, BD and DW participated in data acquisition. All authors participated in analysis and interpretation of data. All authors participated in developing the manuscript and approved the final version to be published.
Funding This study was conducted by the Immune Tolerance Network. Research reported in this publication was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under Award Numbers NO1AI15416 and UM1AI109565. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Study medication was provided by Bristol-Myers Squibb.
Competing interests DW has received consulting fees, speaking fees and/or honoraria from Genentech and GlaxoSmithKline.
Ethics approval Received institutional review or ethics board approval at each clinical site.
Provenance and peer review Not commissioned; internally peer reviewed.