Article Text

Abstract
Objective The type I interferon pathway is activated in many patients with systemic lupus erythematosus (SLE), and anti-double-stranded DNA (dsDNA) and anti-RNA binding protein autoantibodies are correlated with high interferon-α (IFNα) activity. We studied whether antiphospholipid (APL) antibodies, which should not stimulate Toll-like receptors, are also associated with high levels of IFNα activity.
Methods Serum IFNα activity was measured in patients with SLE using the WISH cell bioassay. IgG APL, anti-RBP and anti-dsDNA antibodies were measured in the clinical laboratory, and standard clinical cut-offs were used to define the positive results.
Results High IFNα activity was associated with anti-RBP and anti-dsDNA antibodies in all three ancestral backgrounds. Strikingly, African-American subjects with a positive APL antibody test had higher IFNα activity than those without IgG APL antibodies. This was not shared with other ancestral backgrounds. This finding was independent of other autoantibody profiles, and clinical features did not differ between IgG APL antibody positive versus negative African-American patients.
Conclusion The difference in association between IFNα activity and IgG APL status between ancestral backgrounds supports differences in molecular pathogenesis. This may suggest B cell hyperactivity in the setting of type I IFN in African-Americans and could suggest ways to individualise therapy.
- systemic lupus erythematosus
- cytokines
- antiphospholipid antibodies
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Systemic lupus erythematosus (SLE) is an inflammatory autoimmune disease caused by dysregulation of the immune system, affecting women nine times more often than men. The incidence and prevalence of SLE are higher in non-European ancestry, especially in African ancestry. The severity of SLE also varies among the ancestral backgrounds, being more severe in non-European populations and genetic factors are believed to contribute to this difference.1
Type I interferon, in particular interferon-α (IFNα), plays a crucial role in the pathogenesis of SLE, having pleiotropic effects on various cell types.2 It is known that IFNα activity is higher in patients with SLE compared with other autoimmune disease (eg, rheumatoid arthritis) or healthy individuals3–5 and is proven to be a heritable risk factor in patients with SLE6 also associated with more severe disease.2 Moreover, IFNα activity levels are higher in African-American patients with SLE as compared with other ancestral backgrounds.4 The evidence that recombinant IFNα treatment for hepatitis C leads to de novo lupus and characteristic autoantibody production supports the importance of IFNα in the pathogenesis of SLE.2
Autoreactive B cells are the source of pathogenic autoantibodies in SLE and serological presence of certain autoantibodies are associated with the excess expansion of plasma cells in patients with SLE.7 IFNα plays a role in B cell differentiation and could promote autoantibody production. Ducreux et al reported that culturing healthy peripheral blood mononuclear cells with IFNα promotes signal transducer and activator of transcription 3 phosphorylation in naive B cells and induce the same skewed activation pattern in B cells that is spontaneously seen in patients with SLE: decreased naive B cells, decreased unswitched memory B cells, increased switched B cell and increased plasma blasts.8
Previous studies have shown that the presence of specific autoantibodies (ie, anti-Ro, anti-Sm, anti-double-stranded DNA (anti-dsDNA) and antiribonucleoprotein (anti-RNP) antibodies) in patients with SLE are associated with high IFNα activity.4 In vitro studies support the idea that immune complexes formed by these autoantibodies can stimulate Toll-like receptors (TLRs) via their nucleic component,9 10 suggesting a mechanistic link between antinuclear antibodies and IFNα.
Thus, while it seems that the downstream impact of autoantibody immune complexes in inducing type I IFN is fairly well supported, this would not rule out an effect of IFN on the initial production of autoantibodies via B cell activation. There is no evidence to date that antiphospholipid (APL) antibody immune complexes can activate TLRs, providing an opportunity to explore this question in patient cohorts. We sought to examine whether APL antibodies in patients with SLE are associated with high levels of IFNα activity in patients with SLE. Finding an association could suggest the importance of IFNα in the initial formation of autoantibodies in human SLE.
Patients and methods
Patients and samples
Serum samples were obtained from 382 patients with SLE (216 African-American, 67 Hispanic-American, 99 European-American) from the University of Chicago and Rush University Medical Centre. All the patients fulfilled ≥4 of the American College of Rheumatology (ACR) revised criteria for the diagnosis of SLE.11 All patients provided informed consent.
Autoantibody detection
ANA were measured by indirect immunofluorescence methods. APL, anti-Ro/La, anti-Sm and anti-RNP antibodies were measured by ELISA methods and anti-dsDNA antibodies were measured using Crithidia luciliae immunofluorescence, with detectable fluorescence was considered positive. In this study, APL positivity is defined as a positive IgG anticardiolipin test (>20 GPL U/mL). All the samples were assayed and analysed in the same clinical laboratory at University of Chicago, and standard clinical cut-offs were used to define a positive result.
Serum IFNα activity measurement
Reporter cells (WISH cells, ATCC #CCL-25) are used to measure the ability of sera to cause IFNα-induced gene transcription. WISH cells are incubated with patient sera for 6 hours and then lysed and three canonical IFNα-induced transcripts (ie, IFN-induced protein with tetratricopeptide repeats 1, myxovirus resistance 1,and protein kinase R) are measured by reverse transcriptase-PCR. Relative expression data from the three transcripts are then normalised by the healthy multiancestral control data and presented as an IFNα activity score (full method outlined in Niewold et al6).
Statistical analysis
The study population was stratified by ancestral background prior to analysis. In the univariate analyses, the Χ2 was used to compare differences in proportions of the baseline profiles and antibody status between the three ancestral backgrounds. A stepwise multivariate regression was performed including age and all antibodies as predictor variables and IFNα as the outcome variable, and P value <0.05 was considered significant.
Results
Baseline data and prevalence of antibodies in patients with SLE stratified by ancestral background
Around 90% of the study population was female, resembling the general female/male ratio in patients with SLE. Mean age was younger in Hispanic-American population. Prevalence rate of a positive test for ANA was over 95% in each ancestral patient group. African-Americans had a higher prevalence rate of positive test for anti-Sm, anti-RNP and anti-Ro antibodies as compared with other ancestral backgrounds. African-Americans were significantly less likely to have a positive IgG APL antibody test than European-Americans (P=0.015, OR=2.3, Fisher’s exact test) (table 1). Consistent with previous reports, baseline IFN activity was higher in African-American patients compared with other ancestral backgrounds (P<0.0001, Kruskal-Wallis test) (table 1).4
Baseline data and antibody profiles in patients with SLE stratified by ancestral background
Univariate analyses between the prevalence of antibody status and IFNα activity in patients with SLE stratified by ancestral backgrounds
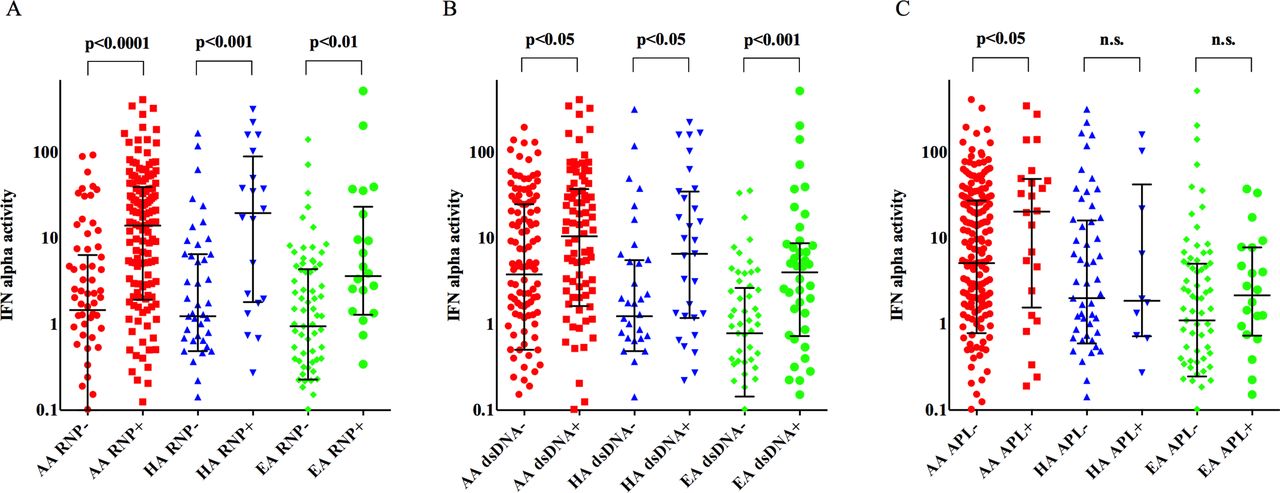
Patients with SLE with positive test for anti-RNP or anti-dsDNA antibody had higher IFNα activity in all three ancestral populations (figure 1A, B). African-American subjects with a positive IgG APL antibody test had higher IFNα activity than those without APL antibodies (P=0.037). This was not shared with other ancestral backgrounds, although there was a non-significant trend in a similar direction in European-Americans (figure 1C). There were no differences in prevalence rate of other autoantibodies when comparing IgG APL antibody negative and IgG APL antibody positive African-American patients. In addition, age did not differ between IgG APL antibody negative and IgG APL antibody positive African-American patients, which is important as younger patients typically have higher serum IFNα activity.12

{kind=link}
Association of autoantibody profile and IFNα activity in each ancestral background. (A–C) Difference in IFNα activity between negative and positive test for autoantibodies (anti-RNP antibody, anti-dsDNA antibody and APL antibody, respectively) in each ancestral background. The horizontal bars represent median and IQR for each group. P values are indicated (P<0.05 was considered significant, Mann-Whitney test). AA, African-American; anti-dsDNA, antidouble-stranded DNA; APL, antiphospholipid; anti-RNP, antiribonucleoprotein; EA, European-American; HA, Hispanic-American; IFNα, interferon-α; n.s., not significant.
Multivariate regression to detect independent associations with high IFNα activity in African-American patients with SLE
Multivariate regression analysis revealed that the positive test for APL antibody independently correlates with high IFNα activity in African-American populations. As expected, anti-Sm and anti-dsDNA antibodies each also contribute to high IFNα activity; however, APL antibodies were a strong independent factor associated with high IFNα activity in African-American patients with SLE, while this was not observed in other ancestral backgrounds (table 2). A positive test for anti-La and anti-RNP antibodies in Hispanic-American patients and a positive test for anti-RNP antibody in European-American patients were independently associated with high levels of IFN alpha activity in these ancestral backgrounds, respectively (table 2).
Results of stepwise multivariate regression analysis for detecting independent associations with high IFNα activity in patients with SLE
Discussion
In this study, we identified for the first time that positive test for APL was a strong independent factor associated with high IFNα activity in African-American patients with SLE. This was not observed in previous studies5; however, in previous studies patients of multiple ancestral backgrounds were typically analysed together and the majority of the study populations were of non-African-American ancestry.5 Although our data was cross-sectional, the study population was large and the association with positive test for APL antibody and high levels of IFNα in African-Americans was robust across both univariate and multivariate analyses.
A report has shown that non-bilayer phospholipid arrangement, a transient lipid component modification, can stimulate TLR2/6 and TLR4.13 While it could be possible that APL immune complexes could stimulate IFNα production, if this was the case, we would expect to see APL antibodies associated with IFNα activity across all ancestral backgrounds as we observed with anti-RNP autoantibodies. As mentioned above, IFNα is also known to play an important role in skewing B cell differentiation and promoting autoreactive B cells.8 Data from a trial of IFN-kinoid showed that neutralising IFNα reduces the expression level of transcripts that are related to B cell activation via TLR9 signalling pathways,14 supporting a connection between IFNα and B cell activation in human patients with SLE. When considering our findings specific to African-American SLE, there is an interesting recent report supporting an activated B cell phenotype in African-American patients with SLE as compared with European-American patients with SLE.15 Menard et al recently showed a distinct memory B cell subset expansion (double negative B cells: CD19+ IgD− CD27− and activated B cells expressing high levels of CD80, CD86, PD-1 and CD40L) in African-American but not European-American patients with SLE.15 As in other studies, we find that the baseline level of type I IFN activity is significantly higher in African-American patients (table 1). It is possible that both intrinsic B cell factors and increased exposure to type I IFNs result in this B cell activation observed in African-American patients.15 The present study emphasises the biological diversity between patients with SLE of different ancestral backgrounds, which will be important in considering targeted therapies, such as anti-IFNα and others.
References
Footnotes
Contributors TI and TBN designed the study, analysed the data and wrote the manuscript. JD performed the experiments, analysed the data and contributed to the manuscript. MJ and XYH generated and analysed the data and contributed to the manuscript.
Funding NIH grants (AR060861, AR057781, AR065964, AI071651), the Mayo Clinic Foundation, the Lupus Research Alliance and the Colton Center for Autoimmunity to TBN. National Natural Science Fund of China (No. 81072477)
Competing interests TBN has received research grants from Janssen and EMD Serono which are unrelated to the current study.
Patient consent Obtained
Ethics approval Institutional Review Board at the respective institutions.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Interferon data from this paper could be made available upon request for a meritorious and non-overlapping project proposed with appropriate ethics approval.