Article Text

Abstract
Objectives To describe how immunosuppressant use and hospitalisation patterns for SLE have evolved by comparing admission statistics at one academic centre between 2005 and 2013.
Methods We identified admissions for SLE and for all hospitalised patients by using the hospital electronic database. For adult patients with SLE, a comprehensive chart review was conducted to identify primary indications for hospitalisation, in-hospital mortality, mean length of stay and immunosuppressant use.
Results The number of yearly SLE patient hospitalisations decreased from 178 to 86 between the two times of observation. Infection was the most common reason for hospitalisation accounting for 39.9% of hospitalisations in 2005 versus 31.4% of hospitalisations in 2013 (p=0.29). Lupus flare accounted for 9.6% of admissions in 2005 versus 8.1% of admissions in 2013 (p=0.72). Seven patients died during their hospitalisation (3.9% of admissions) in 2005 as opposed to no inpatient deaths in 2013. Of the 261 admissions between 2010 and 2013, six admissions resulted in death (2.3% of admissions). SLE patient mean length of hospital stay decreased from 7.6 days to 6.4 days (p=0.36) compared with all patient length of stay, which decreased from 6 days to 5.8 days. Corticosteroid use decreased (79.8% to 61.6%, p=0.11) while hydroxychloroquine (27.0% to 59.3%, p<0.001) use increased over time.
Conclusions The number of hospitalisations, mortality and length of stay among hospitalised patients with SLE decreased over time. Infection was the primary reason for inpatient hospitalisation. Hydroxychloroquine use more than doubled over this same time period with statistical significance. These pilot data suggest improvements in SLE hospitalisation outcomes over time, but larger studies are needed to examine these trends and to understand the relationship between changing medication prescribing patterns and hospitalisation outcomes in patients with SLE.
- systemic lupus erythematosus
- corticosteroids
- dmards (synthetic)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
SLE is an autoimmune disease with an estimated prevalence ranging from 40 to 150 cases per 100 000 individuals in the USA.1–4 SLE is clinically characterised by flares and remissions, and often requires patient hospitalisation. It has been estimated that 22% to 28% of US patients with SLE are hospitalised each year.1 In fact, SLE and other connective tissue diseases have been ranked the sixth most likely conditions to result in 30-day re-admission to the hospital5 with an estimated 16.5% to 27.2% of patients requiring re-admission.5 6 Furthermore, a study from 1998 to 2002 demonstrated that 3% of SLE hospitalisations resulted in death.7 Understanding trends in hospitalisation outcomes for SLE is important for monitoring outcomes of the disease and for examining the impact of changing treatment paradigms on these outcomes.
Traditionally, SLE has been treated with corticosteroids, which are known to promote infections, hyperglycaemia, hypertension, osteoporosis and avascular necrosis among other adverse effects.8 Over the past few decades, new medications with different side effect profiles have been developed or have been repurposed for SLE. For instance, hydroxychloroquine usage patterns may have changed in recent years due to emerging evidence suggesting damage prevention and/or efficacy.9–11 However, few studies have examined whether changes in hospitalisation outcomes may correlate with treatment patterns.12 13
To address this gap, we performed a pilot study at an academic medical centre to examine SLE hospitalisations and changes in medication use between 2005 and 2013.
Methods
Data source and population
Data were derived from a comprehensive chart review of all SLE hospitalisations at the University of California San Diego (UCSD) Medical Center in 2005 and 2013. The UCSD Medical Center is an academic training centre that offers primary through tertiary medical care to a wide spectrum of socioeconomic and ethnic/racial groups. San Diego County serves as its primary referral base. According to the US Census Bureau, the population of San Diego County was approximately 2.8 million in 200514 and 3.2 million in 2013.15 The medical centre’s ambulatory care offices served an estimated cohort of 490 patients with SLE.
Patients with SLE were identified by querying the UCSD hospitalisation databases for records containing one or more billing codes for SLE (710.0 of the International Classification of Diseases, Ninth Revision, Clinical Modification or ICD-9-CM). For the year 2005, billing codes were available through an inpatient electronic database, and physician notes and other clinical variables were available through paper charts; after 2010, UCSD adopted the electronic medical record system EPIC, so data were derived from queries and review of comprehensive electronic health records. The medical centre maintains historical data to monitor all cause hospitalisation rates and patient insurance use.
The year 2013 was chosen as the end date of the study so that ICD-9 diagnosis and procedure codes would be used at both time points. During our project planning stages, ICD-10-CM implementation was planned to be required by 1 October 2014 (this was later delayed by lawmakers to 1 October 2015). Patients who were identified by a treating rheumatologist as not meeting at least 4 of the 11 diagnostic criteria for the 1997 update of the 1982 American College of Rheumatology (ACR) Revised Criteria for Classification of SLE were excluded, as were patients less than age 18.
Primary outcomes
The primary outcomes for the analyses were (1) all-cause hospitalisations, derived from the hospital electronic database; (2) in-hospital mortality, derived from chart review; and (3) prescription information, derived from chart review.
Additional variables
Patient demographics, diagnoses during the hospitalisation, hospital length of stay and 30-day readmissions for patients with SLE were obtained directly from the chart. Hospital length of stay was obtained from the hospital electronic database with chart confirmation when available. Reasons for hospitalisation were identified and classified by the reviewing physician. Admissions classified as neurological included seizure, optic neuritis, infarct, amaurosis fugaux, headache and low intracranial pressure. Pulmonary embolism was classified under thrombosis. Examples of cardiac admissions include acute coronary syndrome, congestive heart failure, and arrhythmia. Examples of admissions classified as other include miscellaneous surgical procedures, atypical non-cardiac chest pain and psychiatric admissions. Hospital-wide patient data including number of hospitalisations, mean length of hospital stay and payer mix were obtained from hospital electronic records. In additional analyses, we reviewed all mortality data for patients with SLE admitted between 2010 and 2012. Chart reviews and data abstraction were performed by the primary reviewer (CA). Any uncertainty was adjudicated by another reviewer (KK).
Statistical analysis
Continuous variables are presented as mean±SD, while categorical variables are presented as counts and percentages for the two time periods. Statistical tests were not performed on mortality data due to the rare number of events. Length of stay was compared between years using an independent two-sample t-test. To compare the rates of reasons for hospitalisation and medications associated with each hospitalisation between years, we use a Poisson generalised linear model with an offset term to account for subjects with multiple hospitalisations. The outcome of this model was the number of hospitalisations due to each specific reason or the number of times a medication was associated with a hospitalisation for each subject. The log of the total number of hospitalisations for that subject is included as an offset term to act as an exposure variable, accounting for the heterogeneous number of hospitalisations across subjects. The only predictor in this model is a binary indicator for year 2013, and the effect associated with this predictor indicates a change in the rate of hospitalisations due to each reason or a change in the rate of hospitalisations associated with each medication. Each model was checked for overdispersion and zero inflation by visual inspection of histograms of the count data, plots of standardised residuals and through Vuong’s non-nested likelihood test against a similar model fit under the negative binomial framework, which allows additional modelling of a dispersion parameter. If overdispersion was detected for any outcome, inference is drawn instead from the negative binomial model. The p value from this model can be interpreted as evidence of a change in the relative rate of events (reasons for hospitalisations or medications associated) between years.
Results
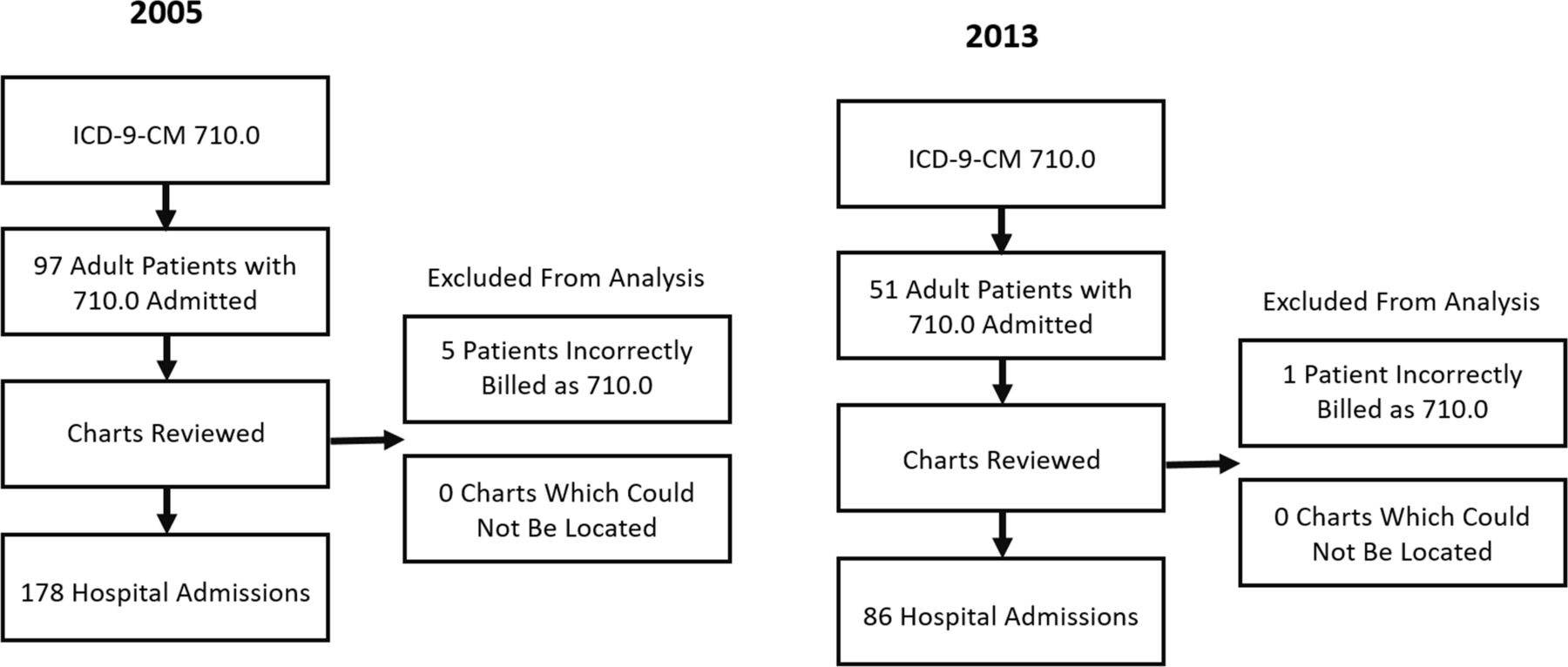
We identified 183 hospitalisations in individuals with SLE in 2005 and 87 hospitalisations in 2013 (figure 1). Five patients in 2005 and one patient in 2013 had an ICD-9-CM code for SLE but did not fulfil the ACR criteria; most of these patients were subsequently diagnosed with a different autoimmune condition and all were excluded from the analysis. The final sample included 178 hospitalisations in individuals with SLE in 2005 and 86 hospitalisations in 2013. Patient characteristics are listed in table 1.
{kind=link}
Flow diagram of patient chart identification. ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification.
Characteristics of hospitalised individuals with SLE in 2005 and 2013
All-cause hospitalisations at our institution rose over the 9 years from 21 333 in 2005 to 25 999 in 2013. SLE admissions accounted for 0.83% of total admissions in 2005 as compared with 0.33% of total admissions in 2013. The average age of all admitted patients to UCSD in 2013 was 52 years. The percentage of admitted patients at UCSD in California’s Medicaid programme was 28.3% in both 2005 and 2013.
Seven patients (7.6% of patients with SLE and 3.9% of SLE admissions) died during their hospitalisation in 2005. Four of the seven deaths were due to overwhelming infection. The other deaths were due to thrombotic thrombocytopenic purpura, cancer and a gastrointestinal bleed. The mean and median ages of deceased patients were 44 and 48, respectively. No patients died in 2013. Of the 261 admissions between 2010 and 2013, six admissions resulted in death, leading to a mortality rate of 2.3% of SLE admissions.
Corticosteroid use decreased over the measured time period (table 2). Hydroxychloroquine use increased. Within the cohort of patients admitted with infections, the percentage of oral glucocorticoid use dropped from 2005 to 2013 (70% to 55%) while the percentage of hydroxychloroquine (23% to 59%) and mycophenolate mofetil/mycophenolic acid (5.5% to 15%) use more than doubled. Similarly, within the cohort of patients admitted for non-infectious illness, oral glucocorticoid use decreased from 2005 to 2013 (62% to 46%) while hydroxychloroquine (30% to 51%)%) and mycophenolate mofetil/mycophenolic acid (3.6% to 12%) use increased.
Medications associated with hospital admissions among individuals with SLE
Patients could have had more than one diagnosis requiring hospitalisation. The most common reason for hospitalisation was infection at both time periods, but the percentage of patients with SLE being hospitalised with infection decreased over time (table 3). The change in relative rate of events was not statistically significant for any reason for hospitalisation.
Reason for hospitalisation among individuals with SLE in 2005 and 2013
Cardiac admissions were almost twice as frequent in 2013; however, part of this difference was likely due to multiple admissions in the year for cardiac disease from a subset of patients. When repeating the analysis measuring whether or not each patient was admitted for a cardiac condition during the year, the difference is smaller with 12% of patients having at least one admission for cardiac disease in 2013 versus 9.7% in 2005.
Mean length of hospitalisation decreased from 7.6 days to 6.4 days (p=0.361) between 2005 and 2013. The decrease in length of stay did not reach statistical significance. In contrast, mean length of stay of all patient hospitalisations decreased from 6 to 5.75 days between 2005 and 2013.
There were thirty-five 30-day readmissions in 2005 (19.6% of total admissions) compared with fourteen 30-day readmissions in 2013 (16.3% of total admissions). Within the entire year, 51% of the 178 hospitalisations in 2005 as opposed to 39% of the 86 hospitalisations in 2013 were due to patients requiring two or more admissions in 1 year.
Discussion
In this pilot study, we examined trends in hospitalisation outcomes for SLE at a single centre and also evaluated medication use patterns in these patients over time. Our primary findings were that key hospitalisation outcomes, including number of hospitalisations and hospital mortality, decreased over this period, and that more patients used hydroxychloroquine. Although the small size of our study does not allow us to determine if these trends are generalisable or whether improved hospitalisation outcomes are causally related to changing treatment patterns, these preliminary findings suggest that additional work in this area is warranted.
SLE patient hospitalisations dropped over the studied time period. Conversely, all-cause hospitalisations at our institution rose over the 9 years. The percentage of admitted patients at UCSD in California’s Medicaid programme was unchanged in 2013 compared with 2005, suggesting that changes in hospitalisations are likely not related to the hospital’s payer mix. It is unlikely that the change in hospitalisation was due to change in patient racial demographics because by 2013 the patient population had a higher percentage of blacks and a lower percentage of Asians. Black patients are more likely to be diagnosed younger, to have higher disease burden and to be hospitalised more frequently than other racial groups.4 16 Further studies are needed to confirm our results of fewer SLE hospitalisations over time.
Adult SLE patient hospital mortality at our California-based academic medical centre fell between 2005 and 2013. This mirrors the global trend of improving survival in patients with SLE. Whereas the SLE 5-year survival rate in 1950 had been estimated at approximately 75%, it had risen to approximately 95% by 2010.17 A different study evaluating all SLE hospitalisations in Washington State found a similar outcome with a drop in hospital mortality from 3.1% in 2003 to 1.3% in 2011.16 Improving mortality has also been demonstrated in paediatric patients.18 Patients with SLE who died in our hospital had a median age of 48 years. Their relatively young ages highlight the importance of focusing research efforts on identifying ways to limit SLE patient mortality. The majority of deaths at our institution were due to overwhelming infection.
Mean length of hospital stay dropped by 1.2 days for patients with SLE compared with less than 1 day in the general UCSD population. If this decrease in length of hospital stay is reproducible and statistically significant with a larger sample size, this could potentially lead to monetary savings for healthcare systems.
We found that hydroxychloroquine use doubled between 2005 and 2013 among hospitalised patients with SLE. A handful of studies have demonstrated an association between hydroxychloroquine use and decreased infection rate or mortality.9 19–21 Some research has previously suggested that hydroxychloroquine may protect against seizure occurrence,22 and hydroxychloroquine has been correlated with reduced thrombotic cardiovascular events.19 We cannot determine whether the increased use of hydroxychloroquine among patients with SLE contributed to the improved hospitalisation outcomes in the current study. Nevertheless, it would be useful to link outpatient medication use data with hospitalisation data in larger studies to understand variables affecting SLE outcomes.
The drop in corticosteroid use trended towards statistical significance. Corticosteroid use has been shown to increase infection risk in patients with SLE in multiple studies,20 21 23 but the potential impact of outpatient corticosteroid use on hospitalisation rates and outcomes needs to be more thoroughly evaluated.
Infections accounted for the majority of overall admissions during both study years, and the percentage of infections decreased over time. Our retrospective study was not statistically powered to detect a change in infection rate, but we believe the numerical decrease in infectious hospitalisations is important to further investigate. Multiple other studies around the world also demonstrate that infection is the first or second most common reason for hospitalisation in their SLE patient cohorts.13 24 25 Moreover, at our institution, repeated admissions in 1 year dropped by 12% from 2005 to 2013 with a substantial part of that decrease being due to fewer admissions for infections. Assuming that physician admission criteria for infections has not dramatically changed over the 9 years, these results may suggest that patients with SLE are getting fewer infections requiring hospitalisation. Similarly, the percentage of admissions for lupus flare decreased over the study period. Trending these clinically important findings over time and with bigger populations may prove useful.
Our research protocol’s strength lies in that we individually reviewed the chart of each admitted patient with SLE, allowing for an accurate and thorough appraisal of each patient’s medical history. However, these results represent data from one academic centre, so the results may not be widely applicable. We chose to use 2005 as the start date because we hypothesised that clinical practice would significantly change over the coming years due to important publications highlighting benefits of medications, which were repurposed for SLE.9 11 26 This start date presented a challenge in that all charts were still paper at that time. As a consequence, we were unable to identify the total outpatient cohort of patients with SLE at UCSD in 2005. Ideally, we would be able to compare the demographics and medication profile of admitted patients with outpatients not admitted that same year in order to better examine changes in hospitalisation trends among our ambulatory population. Although we observed changes in medication therapy for hospitalised patients with SLE over the time period examined, we cannot determine whether these medication changes contributed to the changing hospitalisation patterns.
In conclusion, our research demonstrates that the number of hospitalisations and inpatient mortality among patients with SLE at our academic medical centre decreased from 2005 to 2013. Length of stay and 30-day readmissions also dropped, but our study was not powered to detect significant changes in these outcomes. Hydroxychloroquine use more than doubled with statistical significance and corticosteroid use decreased. Infections were the primary reason for inpatient hospitalisation at both time points. Overall, this pilot study suggests both improved SLE hospitalisation outcomes over time and evolving medication prescribing patterns. A larger investigation examining the relationship between hospitalisation outcomes and medication use is warranted.
References
Footnotes
Contributors Study design: AB, CA, KK. Acquisition of data: CA, OD,AB, KK. Analysis and interpretation of data: CA, OD, KK. Manuscript preparation: CA, OD, JP, KK. Statistical analysis: JP, SV, CA, KK.
Funding William Wolfe Research Fund, University of California San Diego.
Competing interests None declared.
Patient consent Not required.
Ethics approval This study was reviewed and approved by the University of California San Diego Institutional Review Board under Project number 140746. A waiver of individual authorisation for the use of Protected Health Information (PHI) was granted based on HIPAA Privacy Rule 45 CFR 164 section 512 (I) and the research satisfying the following criteria: the use or disclosure of PHI involves no more than minimal risk; granting of waiver will not adversely affect privacy rights and welfare of the individuals whose records will be used; the project could not practicably be conducted without a waiver; the project could not practicably be conducted without the use of PHI; the privacy risks are reasonable related to the anticipated benefits of research; an adequate plan to protect identifiers from improper use and disclosure is included in the research proposal; an adequate plan to destroy identifiers at the earliest opportunity, or justification for retaining identifiers, is included in the research plan; the project plan includes written assurances that PHI will not be re-used or disclosed for other purposes.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.