Article Text

Abstract
Objectives Previous studies demonstrated associations between reduced serum 25-hydroxyvitamin D (25OHD), inflammation and disease activity in paediatric systemic lupus erythematosus (pSLE). The goal of this study was to assess parathyroid hormone (PTH) in its relationship to vitamin D and inflammation, as well as to better understand the role of human cathelicidin (LL-37) in pSLE.
Methods Frozen serum samples collected at baseline of the Atherosclerosis Prevention in Paediatric Lupus Erythematosus (APPLE) study were assayed to determine 25OHD, PTH and LL-37 levels. Pearson’s correlations and Χ2 tests were used to evaluate the relationships between 25OHD, PTH, LL-37, inflammation, disease activity and infection using baseline values collected as part of the APPLE study.
Results 201/221 APPLE participants had serum available for analysis. Serum 25OHD was inversely associated with serum PTH, but not LL-37. Serum PTH was not associated with high sensitivity C-reactive protein, carotid intima media thickness or high-density lipoprotein (HDL) or low-density lipoprotein (LDL) cholesterol, but was negatively associated with lipoprotein(a) levels. Despite no association with serum 25OHD, LL-37 was negatively associated with total cholesterol, HDL and LDL cholesterol and positively associated with age. There was no significant difference in mean LL-37 levels in participants with reported infection as an adverse event during the 3-year APPLE study.
Conclusions Despite links to vitamin D levels in other studies, LL-37 levels were not associated with baseline serum 25OHD concentrations in paediatric patients with pSLE. Despite the lack of correlation with 25OHD, LL-37 levels in this study were associated with cholesterol levels. Some subjects with pSLE have significantly elevated levels of LL-37 of unknown significance. These exploratory results addressing the role of LL-37 levels in pSLE appear worthy of future study.
- systemic lupus erythematosus
- Childhood/paediatric lupus
- autoimmune diseases
- infections
- inflammation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Several previous studies have demonstrated a relationship between paediatric systemic lupus erythematosus (pSLE) and severe vitamin D deficiency.1–3 Specifically, these studies showed that vitamin D deficiency, especially severe deficiency (<10 ng/mL), is more common in patients with pSLE as compared with healthy controls.2 In addition, studies showed a tendency towards greater SLE Disease Activity Index (SLEDAI) scores in those with moderate to severe vitamin D deficiency.1 Studies by Petri et al demonstrated that an increase in serum vitamin D levels by 20 ng/mL (up to 40 ng/mL) was associated with a 21% decrease in the odds of having a high activity score.4 Prior studies using data from the Atherosclerosis Prevention in Paediatric Lupus Erythematosus (APPLE) cohort showed a statistically significant inverse relationship between serum 25-hydroxyvitamin D (25OHD) levels and high sensitivity C-reactive protein (hsCRP), suggesting that vitamin D deficiency is associated with heightened inflammation seen in patients with pSLE.3
Human cathelicidin (LL-37) is an antimicrobial peptide (AMP) that belongs to a class of proteins present in mammals, called cathelicidins, which may confer an important role in innate immunity.5 LL-37 is a 37 amino acid protein, derived from a precursor molecule called human cathelicidin antimicrobial protein (hCAP18) and is the only form of cathelicidin found in humans.6 Secreted LL-37 is found at many barrier sites, typically epithelial surfaces throughout the body, including the skin, gastrointestinal (GI) tract, testis and respiratory tract.7 LL-37 is mainly upregulated when disease is present, especially bacterial, fungal and viral infections. It has been hypothesised that LL-37 may function by interacting with the microbial membrane, thereby disrupting the membrane’s normal activity and serving as an antimicrobial.8
Vitamin D is a known regulator of LL-37 in humans. Vitamin D administered in vitro in human monocytes results in the increased expression of hCAP18 and production of the protein LL-37 due to activation of a vitamin D response element (VDRE).9 10 Further, oral vitamin D therapy has been shown to increase the expression of hCAP18 in peripheral monocytes cultured ex vivo from adults with HIV and osteoporosis.4 11 Lowered expression of vitamin D or low levels of serum vitamin D have been linked to impaired immune response.12 This suggests a relationship between lowered LL-37 levels and deficient immune response.
The hypothesis of this study was that vitamin D status was associated with circulating serum LL-37 and parathyroid hormone (PTH) concentrations in children with pSLE in the Atherosclerosis Prevention in Paediatric Lupus Erythematosus (APPLE) trial. Additionally, we examined the relationship of LL-37, infection and markers of inflammation in patients with pSLE. Cardiovascular markers which had previously been examined demonstrated a correlation between 25OHD deficiency and CRP and low-density lipoprotein (LDL) cholesterol,3 so we hypothesise that PTH will also have a correlation with these same factors due to the known relationship between 25OHD and PTH.
Methods
The APPLE study
The design and methods of the APPLE trial have been reported previously.13 Briefly, APPLE was a prospective, randomised, placebo-controlled trial, enrolling 221 participants with paediatric-onset SLE (1997 American College of Rheumatology criteria) from 21 North American centers.14 15 Patients were excluded if they had nephrotic syndrome, liver disease, renal insufficiency, hypercholesterolaemia (total cholesterol >350 mg/dL), myositis or were pregnant or lactating.13 Data were collected on disease activity (SLEDAI), disease damage (Systemic Lupus International Collaborating Clinics Damage Index (SLICC)) and relevant laboratory data. Grade 3 and above National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) Adverse Events, including infection, were collected during the 3-year trial. Reports of infection were separated into bacterial, viral and fungal.
Serum analysis
Frozen serum samples collected at baseline of the APPLE trial were available for analysis. 25OHD, PTH and LL-37 levels were measured. 25OHD was measured using the automated chemiluminescent technique (IDS-iSYS automated machine, Immunodiagnostic Systems, Fountain Hills, Arizona, USA) in a laboratory that participates in the National Institute of Standards and Technology (NIST)/National Institutes of Helath (NIH) Vitamin D Quality Assurance Programme and the Vitamin D External Quality Assessment Scheme (Emory University, Atlanta, Georgia, USA). PTH was measured by ELISA (Immutopics, San Clemente, California, USA) as was LL-37 (Hycult Biotech, Uden, Netherlands).
Statistical analysis
In general, continuous variables were summarised with a median, and discrete variables were summarised with percentages. To assess the relationship between baseline levels of 25OHD, PTH and LL-37 versus relevant demographic and disease activity markers such as age, body mass index, SLEDAI and various cardiovascular atherosclerosis biomarkers, bivariate scatterplots were generated and Pearson correlation coefficients were calculated with associated p values. Logistic models were constructed to assess changes in observed infections (yes/no) with natural log of LL-37. Transformations such as natural log were performed for variables after visual assessment for linearity. Association of observed infections with baseline LL-37 levels was assessed with Χ2 tests in the logistic model framework.
Statistical significance was defined as a two-tailed p value <0.05. No adjustments were made for multiple comparisons.
Results
Baseline characteristics
Of 221 APPLE subjects, 201 had baseline samples available to be used in the analysis (there was no statistical demographic difference seen between the 20 patients not included in the study and the 201 who provided biosamples). Participants’ median age at entry was 16 years and median duration of SLE was 24 months. Mean SLEDAI score at the time of entry was 4, representing mild activity. Eighty-three per cent of participants were female, 51% Caucasian, 27% African-American and 23% Hispanic. Table 1 shows correlations between 25OHD, PTH and LL-37, as well as correlations with markers of cardiovascular risk and inflammation. Immunosuppressive and immunomodulatory medications were not found to have any significant association with levels of either 25OHD15 or LL-37.
Relationships between baseline levels of 25OHD, PTH and LL-37 versus relevant demographic and disease activity markers
25OHD, PTH and LL-37
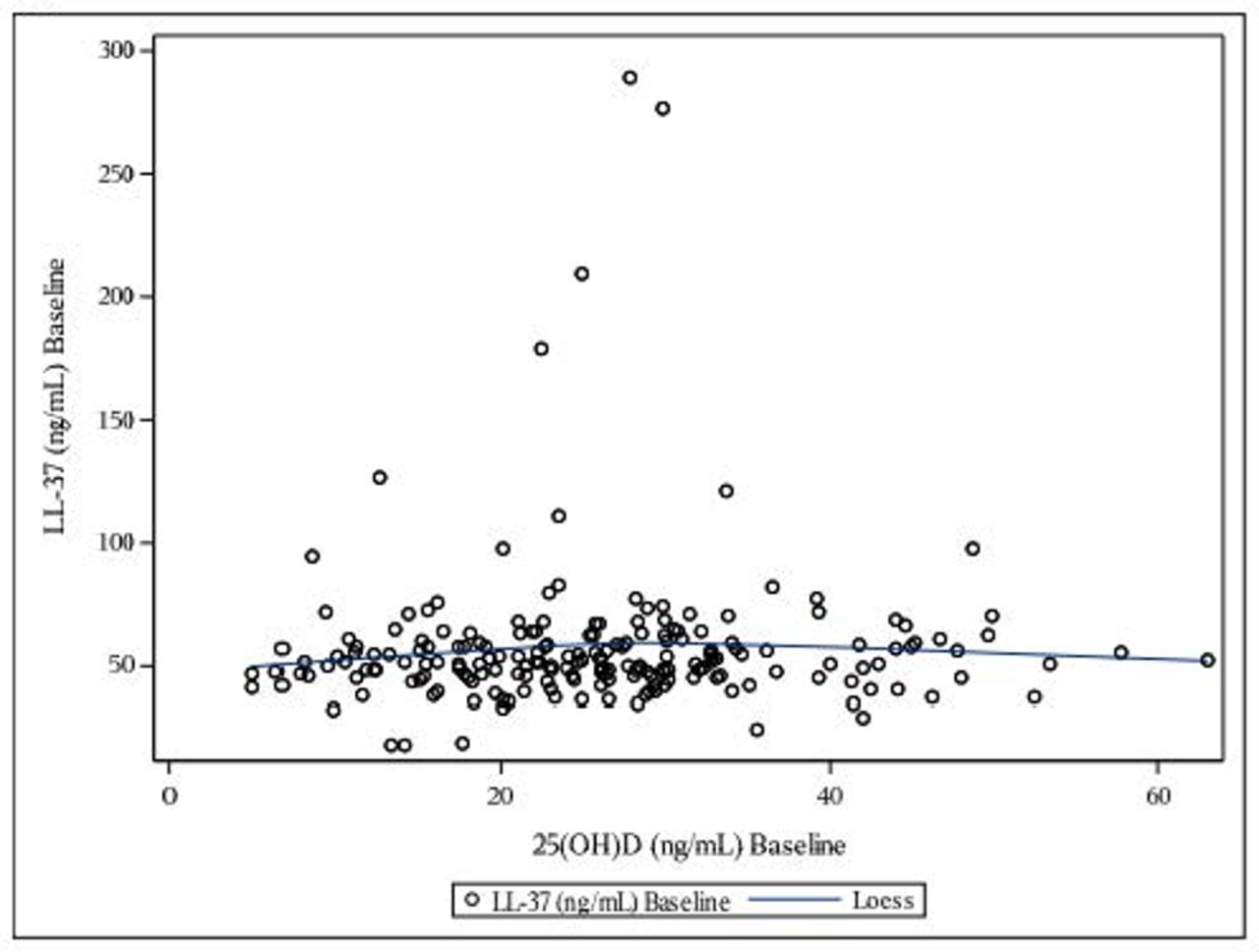
Overall, 61/201 (30%) of participants with available samples had vitamin D deficiency (25OHD <20 ng/mL) at baseline and 139/201 (69%) had vitamin D insufficiency (25OHD <30 ng/mL). Median serum 25OHD levels were 25.8 ng/mL (IQR 18.2–31.7). As expected, 25OHD was negatively correlated with PTH (r=−0.39; p<0.01) (table 1). LL-37 was not associated with 25OHD levels or PTH (p≥0.30) (figure 1 and table 1). The median level of LL-37 was 51.2 ng/mL (IQR 45.5–60.5 ng/mL; absolute range 18.3–289.2 ng/mL). One outlying data point was excluded from the final analysis (LL-37 value >1000 ng/mL) to avoid data skewing.
{kind=link}
No relationship demonstrated between serum 25-hydroxyvitamin D (25OHD) and human cathelicidin (LL-37) in this study.
Associations between PTH, disease activity, and cardiovascular risk
No significant relationship was found between PTH and SLEDAI, hsCRP, HDL cholesterol or LDL cholesterol. However, PTH was weakly associated with lipoprotein(a) levels (r=−0.12, p=0.03).
Associations between LL-37, disease activity and cardiovascular risk
LL-37 was negatively associated with HDL, LDL and total cholesterol (r=−0.19, –0.19 and −0.22, respectively; p<0.01 for all three). LL-37 was also positively associated with age (r=0.15; p=0.03). Data analysed categorically grouping LL-37 values as greater or less than the 75th percentile of 60 ng/mL showed similar results. The association between SLEDAI and LL-37 trended towards significance (r=−0.14; p=0.062) when comparing populations with LL-37 above and below the cut values. Log transformation of LL-37 was used to improve model fit, but did not change the overall results.
LL-37 and infection
LL-37 levels were not significantly different in participants reporting CTCAE Grade 3 or higher infection during the study. Χ2 models were performed on bacterial, fungal and viral infections individually as well as for any infection overall (table 2). Baseline white cell counts also were not associated with LL-37 levels (p value=0.38).
Modelling results of infections versus the Log of human cathelicidin (ng/mL)
Discussion
This is the first analysis of LL-37 levels in pSLE. No correlation was found between vitamin D levels and LL-37 serum levels in the APPLE cohort despite postulated associations between these two markers. LL-37 was also not associated with disease activity, markers of inflammation or infection rates in this study.
It has been demonstrated that vitamin D induces LL-37 expression in non-inflammatory conditions but causes downregulation in the presence of inflammation.12 This may be relevant in that although SLE is an inflammatory condition, the subjects in our cohort did not have high SLEDAI scores. Low SLEDAI scores may indicate relatively low disease activity overall at the time that the samples were drawn. Low disease activity therefore may have resulted in the absence of a relationship between vitamin D and LL-37 levels. It is also possible that the decreased levels of 25OHD prevented subjects from being able to synthesise adequate amounts of LL-37 mRNA.16 Since 25OHD and LL-37 were only measured at a single timepoint, it is difficult to establish causation. In interventional studies, vitamin D supplementation has consistently led to an increase in hCAP18.11
Another possible explanation for the observed discordance is that systemic levels of LL-37 may not reflect local tissue concentrations and LL-37 activity at local barrier sites. One of the limitations of our study is that Hycult Biotech who performed our LL-37 ELISA states that the most reliable results are obtained with plasma samples, which we did not have. It is possible that the LL-37 precursor molecule, hCAP18, may be a better serum marker. While previous studies have shown that precursor hCAP18 is found at low levels in blood and serum, LL-37 is found at much higher concentrations in the context of infection.17 Since the current cohort did not report active infection at the time of enrolment into APPLE when LL-37 levels were obtained, it is possible that hCAP18 would have been a better indicator of disease activity. Unfortunately, there were no prior studies linking hCAP18 to lupus, which kept us from examining this marker in the present study. Additionally, the promoter region of LL-37 contains VDREs, which have 1,25(OH)2D dependent expression.18 It is the 1,25(OH)2D form of vitamin D that is linked to the increased expression of LL-37, possibly explaining the disconnect between 25OHD levels and LL-37. Other studies have also been unable to show a relationship between 25OHD and LL-3719 although studies have shown hCAP induction by 25OHD.11 Future studies measuring serum hCAP18 would possibly need to measure serum 1,25(OH)2D levels, as previous studies have shown that even in the setting of infection and insufficient levels of both 25OHD and 1,25(OH)2D, there was only a statistically significant relationship between 1,25(OH)2D and hCAP18.20 Technically, testing of 1,25(OH)2D can vary on a daily basis and can be a difficult variable to study.
LL-37 is relevant to the discussion of SLE because of its effect on type I IFNs, which are usually found to be elevated in SLE and thought to contribute to disease pathogenesis.21 LL-37 activity often perpetuates an inflammatory cycle by affecting various components of the inflammatory process that take place in disease activity, such as mast cells, neutrophils and dendritic cells. A study by Kreuter and colleagues showed increased AMPs in cutaneous lupus erythematosus, one of which was LL-37, and a lower prevalence of skin infections.22 In our study of paediatric patients, we were not able to distinguish reported skin infections versus other types of infection, but there was no association between baseline LL-37 levels and reported infections over the 3-year follow-up period. We were unable to determine LL-37 levels at the times of reported infection, and this is a weakness of this evaluation.
The relationship between LL-37 and SLE in adult patients has been examined in only a handful of small studies focusing on cutaneous disease22 23; however, this is the first study examining paediatric-onset SLE and LL-37. In the small study by Sun et al, the adult patients with SLE (n=9) were experiencing active disease at the time of sampling, unlike the current study, and high levels of LL-37 expression were found as compared with the normal controls (n=6). Both this study and our results indicate some subjects with SLE have elevated levels of LL-37, which have not, however, been associated with SLEDAI.
A few subjects in the APPLE trial had unusually elevated levels of LL-37 of unknown significance, ranging up to 1000 ng/mL. Fifty-two subjects (26%) had levels greater than the 75th percentile of 60 ng/mL. In a study by Tangpricha et al in which measurements were performed in the same laboratory as the current study, healthy controls reported median LL-37 levels of 51.3 ng/mL with an IQR of 41–98 ng/mL24 (SE was unavailable, so populations could not be compared statistically). Similar to our study, the Tangpricha study was examining relationships between HIV, CD4 and inflammatory markers like LL-37. CD4 count, which is a marker of HIV disease activity, was not always correlated with LL-37 levels. The authors found that LL-37 levels were generally not correlated with inflammatory markers other than IL-6 and also were unable to find a relationship between LL-37 and 25OHD. Unfortunately, in our population, IL-6 was not available to study. These results from paediatric HIV patients mimic those of this study in pSLE.
Finally, the data analysis revealed a negative correlation between LL-37 and total, HDL and LDL cholesterol. Previous analysis of the APPLE cohort actually demonstrated a relationship in disease activity (represented by SLEDAI score) with elevated LDL levels and higher hsCRP with decreased overall HDL levels.25 This suggests that since there is a relationship between LL-37 and cholesterol, and cholesterol and disease activity, there may be an indirect relationship between LL-37 and disease activity. Additionally, in other studies, increased cholesterol levels were found to be associated with increased resistance to LL-37, and it is postulated that elevated cholesterol levels may impair the antimicrobial effect of LL-37.26
Given that LL-37 was not associated with SLEDAI, hsCRP or infection in the current cohort, it is hard to know what the elevated levels represent in the study group. Even though vitamin D and LL-37 have a known relationship, our data did not demonstrate a statistically significant correlation between these two variables. Previous studies support our results in that they have also shown that serum levels did not correlate with circulating LL-37 but rather with cultured ex vivo expression of hCAP18. The demonstrated LL-37 association with cholesterol in our study may be significant in its indirect relationship to disease activity and requires further investigation. Further study is needed to evaluate the relationship between LL-37, vitamin D and cells of the immune system in SLE.
References
Footnotes
Presented at An abstract of this paper was presented at the ACR Annual Meeting for 2016.
Contributors The following participated in this study by enrolling patients at sites or by performing study procedures at sites: Esi Morgan Dewitt, C Egla Rabinovich, Janet Ellis, Janet Wootton (Duke University Medical Center, Durham, North Carolina, USA), Peter Chira, Joyce Hsu, Tzielan Lee, Jan Perea (Stanford University School of Medicine, Palo Alto, California, USA), Beth Gottlieb, Patricia Irigoyen, Jennifer Luftig, Shaz Siddiqi, Zhen Ni, Marilynn Orlando, Eileen Pagano (Cohen Children's Medical Center, New Hyde Park, New York, USA), Andrew Eichenfield, Deborah Levy, Philip Kahn, Candido Batres, Digna Cabral (Morgan Stanley Children's Hospital of New York–Presbyterian, New York, New York, USA), Kathleen A. Haines, Suzanne C Li, Jennifer Weiss, Mary Ellen Riordan, Beena Vaidya (Hackensack University Medical Center, Hackensack, New Jersey, USA), Michelle Mietus-Snyder (University of California at San Francisco Medical Center, San Francisco, California, USA), Lawrence Ng (Hospital for Sick Children, Toronto, Ontario, Canada, USA), Susan Ballinger, Thomas Klausmeier, Debra Hinchman, Andrea Hudgins (Indiana University School of Medicine, Indianapolis, Indiana, USA), Shirley Henry, Shuzen Zhang (Texas Scottish Rite Hospital for Children, Dallas, Texas, USA), Elizabeth B Brooks, Stacy Miner, Nancy Szabo, Lisabeth Scalzi (University Hospitals/Case Medical Center, Cleveland, Ohio), Libby Dorfeld, Sarajane Wilson, Jenna Tress (Children's Hospital of Philadelphia, Philadelphia, Pennsylvania, USA), Tatiana Hernandez, Jyotsna Vitale (University of California Los Angeles Medical Center, Los Angeles, California, USA), Angela Kress, Nicole Lowe, Falguni Patel (Children's Memorial Hospital, Chicago, Illinois, USA), Stephanie Hamilton (Seattle Children's Hospital and Regional Medical Center, Seattle, Washington, USA), Katie Caldwell, Diane Kamen (Medical University of South Carolina, Charleston, South Carolina, USA), Becky Puplava, Atanas Lonchev (University of Chicago, Chicago, Illinois, USA), Monica Bacani (Nationwide Children's Hospital, Columbus, Ohio, USA), Cynthia Rutherford, Jamie Meyers-Eaton, Shannen Nelson, Alexei Grom (Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA), Teresa Conway, Lacey Frank, Lori Kuss (Creighton University Medical Center, Omaha, Nebraska, USA), Hazel Senz (University of Colorado, Aurora, Colorado, USA), Thomas Mason, Jane Jaquith, Diana E Paepke-Tollefsrud (Mayo Clinic, Rochester, Minnesota, USA).
Funding APPLE supported by the NIH (National Institute of Arthritis and Musculoskeletal and Skin Diseases contract N01-AR-2-2265), the Edna and Fred L Mandel Jr. Center for Hypertension and Atherosclerosis and Pfizer. Secondary analysis supported by the Rainbow Babies and Children’s Hospital Pediatrics Pilot Award and the NIH (National Institute of Arthritis and Musculoskeletal and Skin Diseases contract 5P30-AR-047363-12).
Disclaimer The views expressed in the stated article are those of the authors and are not an official position of the affiliated institutions or funders.
Competing interests None declared.
Patient consent Obtained.
Ethics approval CWRU IRB EM-17-19, approved through 5/14/2023.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There is no additional unpublished data from the study.