Article Text

Abstract
Objective Arthritis in SLE is poorly described, and there is no objective measure for quantification of arthritis. In this pilot study, we aim to assess the utility of the Rheumatoid Arthritis MRI Scoring System (RAMRIS) for the quantification of lupus arthritis.
Methods Patients were eligible for entry into the study if they were evaluated at the Medical University of South Carolina Lupus Center and determined by their treating rheumatologist to have active hand arthritis due to SLE. Standard of care lupus activity measures were collected, along with a detailed physical exam. MRIs were obtained using standard musculoskeletal sequences with gadolinium contrast. Semiquantitative scoring of the images used the Outcome Measures in Rheumatology Clinical Trials RAMRIS system.
Results RAMRIS demonstrates large amounts of synovitis, tenosynovitis, bone marrow oedema and erosive disease in only a minority of patients. Some patients were not scored as having any synovitis or tenosynovitis. We describe potential features of lupus arthritis that are not captured in the RAMRIS scores and may be contributing to symptoms.
Conclusion Lupus arthritis is an entity separate from rheumatoid arthritis and requires the development of new quantitative methods to describe and quantitate it. MRI findings suggest the inadequacy of a typical lupus musculoskeletal measure including swollen/tender joint counts to assess the level of disease activity.
- SLE
- arthritis
- “disease activity”
- MRI
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
SLE (lupus) is an autoimmune disease that can involve any organ system. While kidney and nervous system involvement is the more severe manifestation, involvement of the skin and the musculoskeletal system is the most common manifestation. The myriad rashes of lupus are well described with the recent Systemic Lupus International Collaborating Clinics (SLICC) criteria describing 12 separate subtypes.1 However, the musculoskeletal manifestations of lupus described by this criteria include only synovitis of at least two joints and tenderness of two joints with 30 min of morning stiffness. Clinical experience suggests that this is an inadequate representation of the myriad symptoms experienced by patients with lupus with true inflammatory arthritis.
An improved description and quantification of lupus arthritis is necessary to move lupus treatment into an era of precision medicine. First, the symptoms of lupus arthritis are experienced by 90% of patients, and most patients consider it one of the most disabling features of the disease.2 Second, interventional trials for lupus generally require moderate disease activity. Frequently, this includes arthritis. Unfortunately, the available quantitative measures to describe lupus arthritis, such as SLE Disease Activity Index-2000 (SLEDAI-2K) and British Isles Lupus Assessment Group (BILAG), are rough measures and not particularly responsive to change. This has led to modifications such as the SLEDAI-2000 Responder Index 50 and the BILAG-Based Composite Lupus Assessment to detect partial responses, each of which has individual strengths.3 The complexity of SLE necessitates that these indices attempt to account for all the possible changes in disease activity in multiple organ systems. For the most part, they do so and correspond to physicians’ global assessment of disease activity and intention to treat. Nevertheless, within the musculoskeletal system, most measures continue to use mostly subjective assessments of disease activity and improvement. A third reason why improved quantification is necessary is the general difficulty of assessing lupus arthritis on physical exam in the clinical setting. In the vast majority of cases, patients with lupus arthritis do not have the easily palpable synovial hypertrophy of rheumatoid arthritis. The obesity epidemic has not spared the lupus population and significant adipose tissue can mask subtle swelling. Further, as fibromyalgia coexists with SLE in approximately 20% of patients,4 the subjective measures of tenderness and stiffness become even less reliable.
The utility of advanced imaging is just beginning to be applied to lupus arthritis. In 2003, early investigations with MRI noted the different features of SLE arthritis compared with rheumatoid arthritis,5 particularly the presence of oedematous tenosynovitis and capsular swelling. Since that time, a few new evaluations of lupus arthritis using MRI have been reported.6–8 Mosca and colleagues9 evaluated a series of patients with lupus with both ultrasound and MRI. They found that approximately half of the patients judged to be clinically quiescent on clinical exam had inflammation when evaluated with one of these imaging techniques. Additionally, they were able to show a significant amount of erosive damage that was not detected by standard diagnostic radiology. They hypothesise that these ‘sub-clinical’ findings are the causes of subsequent damage and warrant therapeutic intervention. Ball and colleagues8 investigated active lupus arthralgia with contrasted high-field MRI and found a large majority of patients with at least low-grade synovitis and erosive disease.
In rheumatoid arthritis, there are validated measures of arthritis using advanced imaging (MRI and ultrasound). The Outcome Measures in Rheumatology Clinical Trials (OMERACT) Rheumatoid Arthritis MRI Scoring System (RAMRIS) is a validated measure of the inflammatory features of rheumatoid arthritis seen on MRI.10 In multiple clinical trials11 12 MRI is a reliable, responsive and early indicator of outcome. The increased objectivity and quantitation of RAMRIS can allow for small trials (less than 50 patients) that have power to show response.13 The RAMRIS is composed of scores for erosions, bone marrow oedema and synovitis. It has also been supplemented with a score for tenosynovitis.14 The combination of synovitis, tenosynovitis and bone marrow oedema is used to indicate a total MRI inflammatory score and is decreased in patients in clinical remission.15
This study assessed the utility of RAMRIS in scoring lupus arthritis, as well as identified features of lupus arthritis that are incompletely captured by the RAMRIS.
Methods
Twenty lupus patients were recruited to this study from within the Medical University of South Carolina (MUSC) rheumatology practice. The MUSC is a university referral centre for SLE with a large cohort of predominately African–American patients. The entry criteria included that the patient has SLE using the American College of Rheumatology criteria and that the treating rheumatologist believed that the patient had significant inflammatory musculoskeletal lupus activity (defined loosely as lupus arthritis). Notably, the patients were not entered into the study to evaluate IF they had presence of inflammatory activity—the confidence of the treating rheumatologist was high that the patient did have clinically relevant active lupus arthritis. Nephritis was permitted, but patients had to have stable disease and glomerular filtration rate>30 mL/min. All patients signed informed consent documentation.
Clinical scoring of lupus disease activity
There are a variety of methods to score arthritis in lupus. While SLEDAI is collected as standard of care, we focused on swollen and tender joint count. A single evaluator (ESZ) scored each of the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints and the wrist as swollen, tender or both (maximum score of 9 for each). Further record was made of tenderness in the forearm and dorsal hand, palm tenderness proximal to MCPs, and pain with flexion/extension of the wrist and fingers. Routine clinical data were collected during the visit, including the presence of activity in other organ systems. Typical laboratory evaluation was performed for assessment of SLE disease activity and included measurement of anti-double-stranded DNA (anti-dsDNA) (by ELISA), complement levels, white cell count and urinalysis. A standard continuous measure of disease activity on a scale of 0–3 scored on a Visual Analogue Scale16 was collected, as well as a patient-reported pain scale from 0 to 10 on a Visual Analogue Scale.
MRI scoring of arthritis
Patients who consented to the study had an MRI scan of the wrists and hands performed on the same day as their clinical visit. The MRI machine was a whole-body Siemens 3T machine using a medium four-channel flex coil. The MRI protocol consisted of T1 (axial, coronal), T2 fat-saturated axial, proton density fat-saturated coronal, and STIR (short-tau inversion recovery) and T1 volumetric interpolate breath-hold (VIBE) coronal 0.4 mm precontrast and postcontrast sequences were used. The images were scored by RC (musculoskeletal radiologist) and ESZ (rheumatologist). The scoring method was the OMERACT for assessing activity in rheumatoid arthritis, RAMRIS.10 The RAMRIS scores erosions (23 anatomical areas, range 0–10), synovitis (7 anatomical areas, range 0–3) and bone marrow oedema (23 anatomical areas, range 0–3). The tenosynovitis score is scored in 10 areas with a score of 0–3. Tenosynovitis is scored only in the wrist, while the other scores are for the MCPs as well as the wrist. The images were scored independently by the two evaluators without access to any patient information. After the patients were scored, we reviewed the images together to arrive at consensus scores.
Statistics
Descriptive statistics were calculated for all participant characteristics. Spearman’s rank correlation was used to assess the relationships between RAMRIS component scores with self-reported pain and with swelling/tenderness scores. The consistency of scoring between the two raters for each of the RAMRIS scores was evaluated using the intraclass correlation coefficient estimated from a series of linear mixed models. All analyses were performed using SAS V.9.4. Statistical significance was assessed at α=0.05. Given the exploratory nature of the study, no correction for multiple comparisons was made.
Results
A total of 20 patients were enrolled, of whom 75% (n=15) were self-reported African–Americans (table 1). Summary statistics are shown table 1, with individual clinical data presented in online supplementary table S1. While the average duration of disease was 9 years, eight patients had relatively new diagnoses. Patients’ historical manifestations of disease activity are similar to patients in clinical trials with a preponderance of skin and joint manifestations.17 The higher serositis fraction in our cohort is likely due to African–American ethnicity.18 19 Two patients had nephritis, only one of whom was judged to still have active disease. Jaccoud’s (reducible deformity) was clinically apparent in three patients.
Supplemental material
Clinical characteristics of the study population
In terms of SLE disease activity at the time of the MRI scan, all patients were judged to have active SLE arthritis. Other manifestations of disease activity other than arthritis are shown in table 2. Other than the serological markers of disease activity, eight patients had lupus manifestations that would count in the SLEDAI. These were leucopaenia in two, six with rash or mucocutaneous lesions, and only one patient with concomitant nephritis. No neurological manifestations were observed as active. Most patients were on immunosuppression in addition to hydroxychloroquine. The majority of patients did not have serological markers of lupus disease activity. For anti-dsDNA antibody, 8 of 20 patients had an elevated value. If the SLICC criteria of two times the upper limit of normal is used, then only 4 of 20 had a positive anti-dsDNA. Six of 19 (32%) had hypocomplementaemia (one patient did not have complement levels checked at the time of visit).
Disease activity and current treatments
We compared the MRI scores of the radiologist (RC) and the rheumatologist (ESZ) prior to arriving at the consensus scores. There were very few areas of significant disagreement when looking at every joint, and the differences tended to be small (ie, scoring an erosion as 2 out of 10, or 3 out of 10). Higher variability was seen in scoring bone marrow oedema due to subtle variations among low values. The intraclass correlation20 was 0.96 for the erosion score, 0.91 for bone marrow oedema, 0.969 for synovitis and 0.94 for tenosynovitis. These scores are quite high and show internal consistency as well as ease of application of the atlas-based RAMRIS scores.
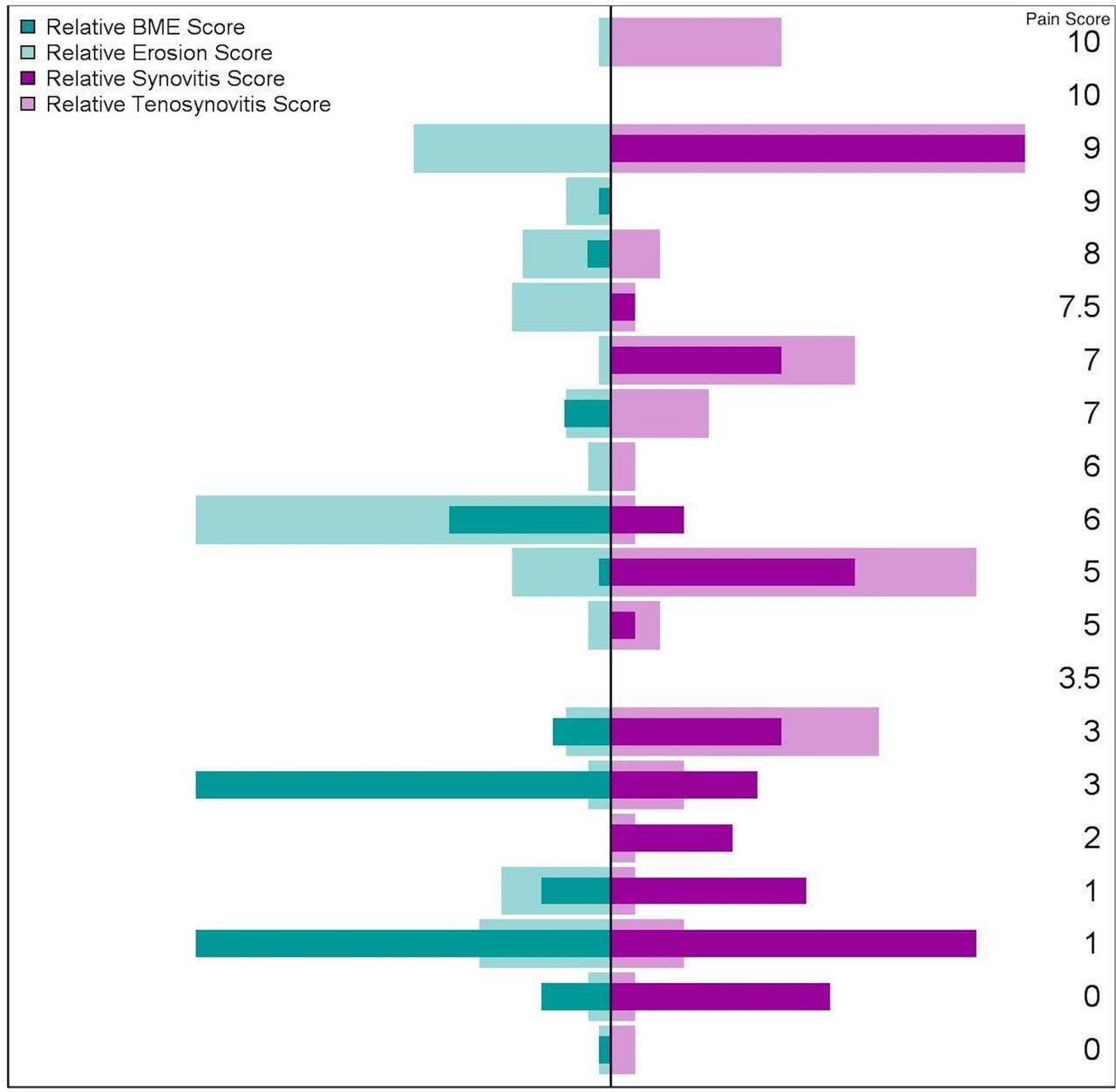
The MRI scores are shown in table 3. The large majority (90%) had some detectable erosions. One patient with long-standing disease and a positive rheumatoid factor had significant erosive disease (patient 2). A majority (55%) of patients had some detectable bone marrow oedema; however, only two patients had high signal. As was expected, 60% of patients had some RAMRIS synovitis, although most was low grade. Tenosynovitis at the wrist was also seen in a majority of patients (85%). The relative contribution of the RAMRIS components for each patient is shown in figure 1.
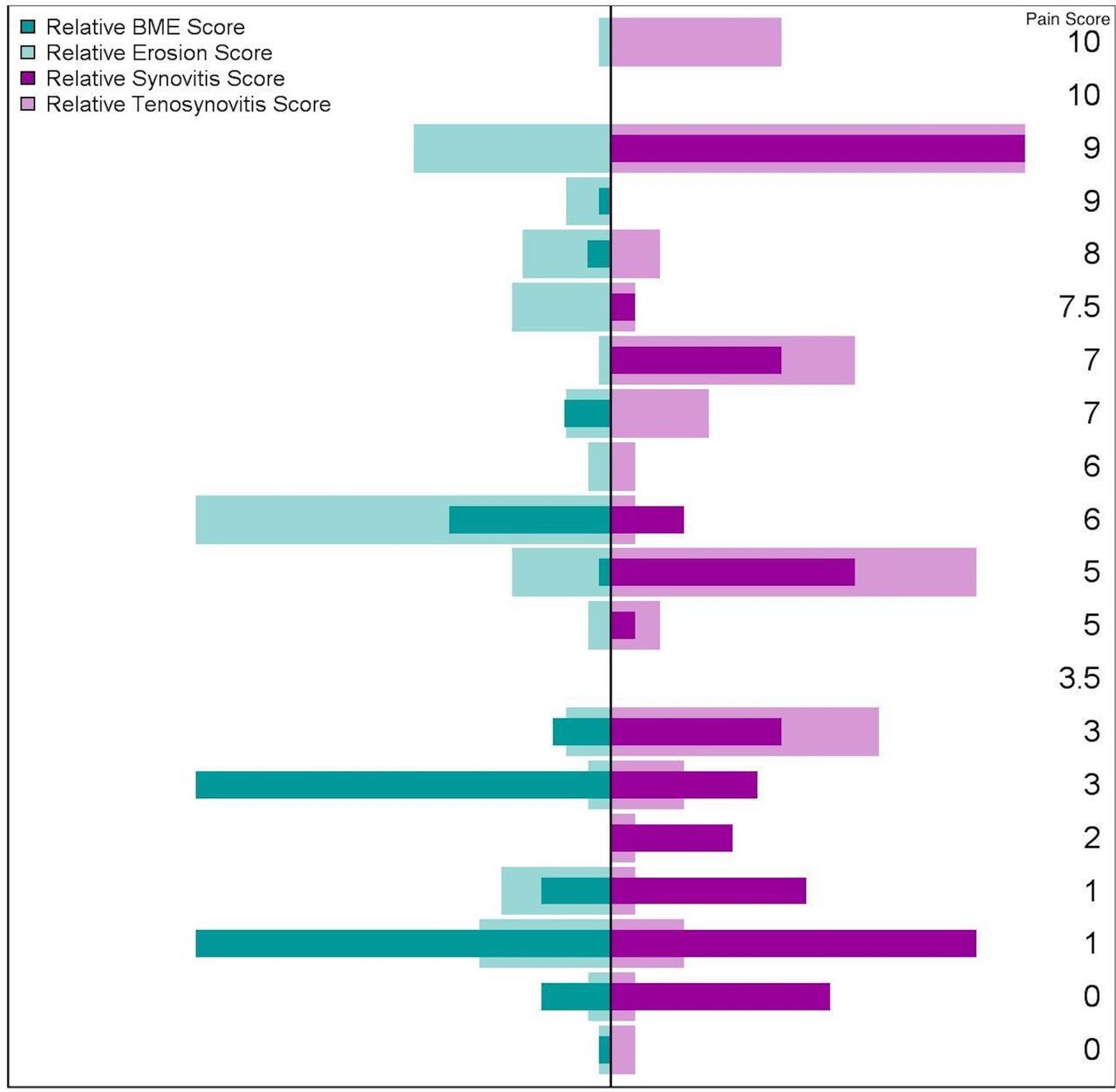
Distribution of the RAMRIS component scores sorted by pain score. The patient with the highest pain score is at the top and the lowest pain score at the bottom. The scores are normalised. Erosion and BME are in the left panel. Synovitis and tenosynovitis are in the right panel. BME, bone marrow oedema; RAMRIS, Rheumatoid Arthritis MRI Scoring System.
MRI scores and swollen tender joint counts
An impetus of the study was to begin developing an objective, quantitative measure of lupus arthritis. This includes attempts to uncover manifestations of joint involvement by MRI that are below the sensitivity of the physical exam. In figure 2 we show the associations between the individual RAMRIS scores and the swollen joint count and the global pain score. There was not a significant association between damage nor swelling (figure 2A and E). Bone marrow oedema was not associated with swelling but nor was it associated with pain (figure 2B and F). The objective measure of joint swelling shows the strongest correlation with the MRI measure of synovitis (r=0.57) (figure 2C) and moderate correlation with tenosynovitis (r=0.42) (figure 2D). Notably, however, the synovitis score was negatively associated with pain. The total inflammatory score (the sum of synovitis, tenosynovitis and bone marrow oedema) has an intermediate correlation of 0.50 with swelling (not shown). Adding just the synovitis and tenosynovitis scores together did not increase the correlation with the swelling count. There was a low association between swollen joints detected by exam and those reported as tender by the patient (table 3; r=0.2). There are patients with significant swelling/minimal tenderness as well as those with minimal swelling/significant tenderness. Of note, the four patients with fibromyalgia have the fewest number of swollen joints (0–2) with higher pain scores (6–10) but have varied tenderness scores (1–8).

The first row shows the association between evaluator-assessed swelling and the RAMRIS component scores: (A) erosion, (B) BME, (C) synovitis and (D) tenosynovitis. The second row shows the association with patient-reported pain and the RAMRIS component scores: (E) erosion, (F) BME, (G) synovitis and (H) tenosynovitis. Pearson’s correlation, r, is reported in the inset. BME, bone marrow oedema; RAMRIS, Rheumatoid Arthritis MRI Scoring System.
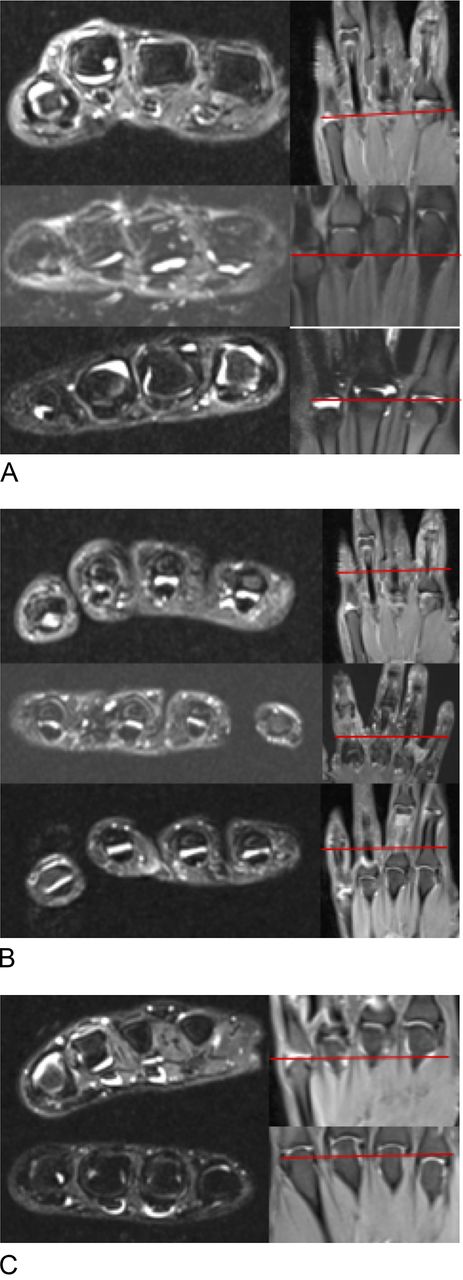
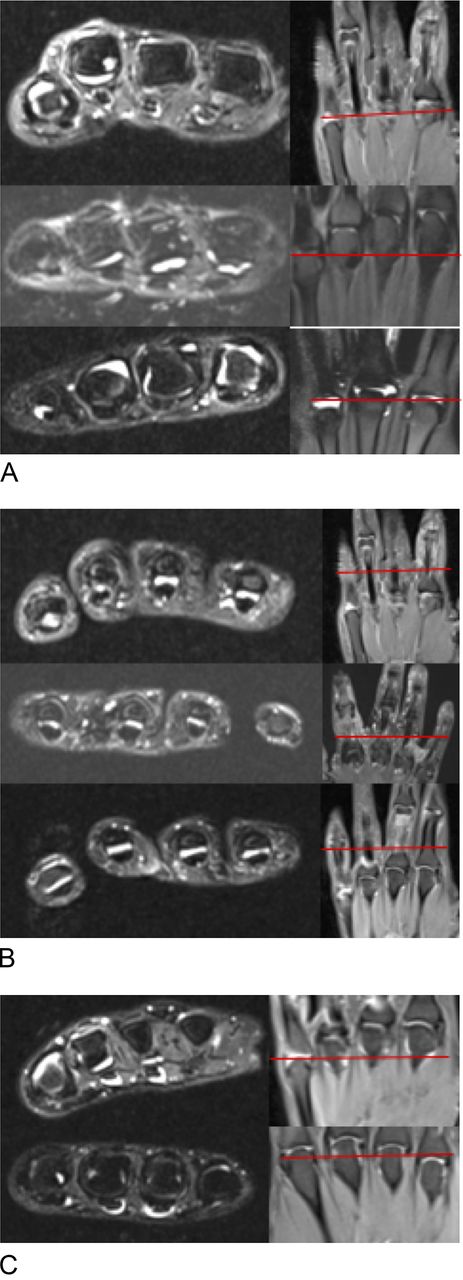
We conducted an extensive evaluation of the images to uncover other features of inflammatory arthritis not scored by RAMRIS (figure 3). Every series was annotated with potentially inflammatory features. While multiple findings were identified in individual patients, there were some common features seen in multiple patients. Focusing on those patients who had synovitis scores of 0, the presence of swollen joints on exam revealed joint effusions that neither enhanced with gadolinium nor had thickened, proliferative synovium (figure 3A). These are appropriately scored as 0 by the RAMRIS criteria but are obviously abnormal on T2 MRI signals. Another group of abnormalities seen on MRI was increased fluid signal around the flexor tendons between the MCPs and PIPs, likely representing a tenosynovitis. In the three examples shown in figure 3B, they all had notable signal in the fingers with minimal tenosynovitis scores in the wrist. Finally, figure 3C shows patients with tendon effusions proximal to MCPs. When we started noticing these findings, we began assessing tenderness in the palm proximal to the MCPs and were able to note some association. This is an area of ongoing investigation.
{kind=link}
{kind=link}
{kind=link}
The left side images are T2 fat-saturated axial images showing the relevant finding, and the right side images are coronal PD fat-saturated images with the red bar localising the finding. (A) Non-enhancing joint effusions on three patients (5, 15 and 16) who all have synovitis scores of 0 but swollen joints on physical exam. (B) Flexor tendon effusions between the MCP and PIP on three patients (5, 7 and 8) who have tenosynovitis scores of 0, 1 and 1 at the wrist. (C) Flexor tendon effusions in the palm proximal to the MCPs in two patients (8 and 11) who have tenosynovitis scores of 1 and 4 at the wrist. MCP, metacarpophalangeal; PD, proton density; PIP, proximal interphalangeal.
Discussion
The goal of this pilot study was to begin developing a method to quantitate active lupus arthritis. We have started with the RAMRIS semiquantitative method that has years of development and validation within rheumatoid arthritis. The long-term goal is to develop a quantitative index that is responsive to change to allow small, focused interventional trials in lupus arthritis.
All patients in this study were thought by the treating rheumatologist to have active arthritis. The perceived degree of joint activity would be similar to those patients considered for a clinical trial, although notably with the current typical criteria in SLE clinical trials (typically an SLEDAI score of 6, 4 points that must come from non-laboratory criteria) only 40% would have met the criteria for inclusion. Two of three patients with the most active arthritis by RAMRIS would not meet the criteria due to receiving only 4 points for SLEDAI arthritis. Two of four patients with the most active tenosynovitis by RAMRIS would not meet the criteria for entry. Of the two patients with profound bone marrow oedema, a process in rheumatoid arthritis that is thought to indicate progression into destructive arthritis, only one would have met the entry criteria.
From a large active cohort of patients with lupus, those patients referred for this study had relatively mild disease outside of the musculoskeletal domain. Granted, significant nephritis or central nervous system disease was an exclusion, but this is common in the SLE trial design. Our findings have implications for trial design in lupus arthritis. An interventional trial targeted to lupus arthritis should be able to recruit significant numbers of patients who do not have significant extra-articular disease. Then, methods to reduce heterogeneity such as removing background medications21 can be performed safely. Further, with an objective, quantitative marker, we should have more sensitivity to detect response.
Heterogeneity was seen in the MRI measures of lupus arthritis and neither patient-reported pain/tenderness nor lupus activity serologies were associated with these measures. The patients with the highest synovitis scores (patients 14 and 9), highest tenosynovitis scores (patients 14 and 20) and highest bone marrow oedema scores (patients 10 and 20) all had normal lupus activity serologies. As shown in figure 1 individual patients could have different quantities of erosions, synovitis, tenosynovitis and bone marrow oedema.
Mild erosive damage was seen in many patients and some had severe rheumatoid arthritis-like damage. The very low scores are of unclear clinical significance. Low-grade erosions were reported in 2.2% of MCP joints and 1.7% of wrist joint bones22 in a study applying RAMRIS to healthy controls. More recently, Tani and colleagues23 applied RAMRIS to rheumatoid arthritis, SLE arthritis and healthy controls using non-contrasted, low-field, extremity-dedicated MRI. They were focused on damage and found low RAMRIS scores in many wrists of healthy controls. They found average scores of 5±2.9, 9.1±8.6 and 13.4±9.4 in healthy controls, lupus arthritis and rheumatoid arthritis. By a similar metric our patients had a mean erosion score of 6.3±8.9, showing a slightly lower burden of erosive disease but similar variability. They proposed a ‘normality’ threshold above which only 2.5% of healthy controls would be expected to score. With this metric 63% of their patients with rheumatoid arthritis and 24% of their patients with SLE surpassed the normality threshold. Three of our 20 (15%) patients meet these criteria. The variability even among these three patients is worth commenting on. Patient 2 (erosion score 38) has long-standing disease, elevated bone marrow oedema score and a positive rheumatoid factor. She had minimal synovitis and tenosynovitis. Patient 14 (erosion score 18) has no bone marrow oedema and a negative rheumatoid factor. She had the highest synovitis and tenosynovitis scores in this cohort. Patient 20 (erosion score 12) was a new diagnosis, with very high bone marrow oedema and a positive rheumatoid factor. She had a very high synovitis score as well. It is unclear based on the MRI findings from the patients in this cohort who would fit the definition of ‘rhupus’, a loose term indicating an overlap of rheumatoid arthritis and lupus.
There is no ‘gold standard’ for the quantification of lupus arthritis; thus, we have nothing to compare with the performance of RAMRIS other than clinical exam and typical metrics in interventional clinical trials. To this end we compared patients who had objective findings of swelling on exam and low RAMRIS component scores. We found joint effusions that would not be scored as there was no enhancement with gadolinium and no synovial proliferation. We note also the tenosynovitis throughout the hand and fingers seen in these patients with SLE even when tenosynovitis was minimal in the wrist. It is worth recalling that RAMRIS is the Rheumatoid Arthritis MRI Scoring system, and perhaps we will need an SLE MRI scoring system.
There are quite a few limitations to this study. Primarily, the small size limits interpretation of the observed heterogeneity. We simply did not have enough patients to comment on various subsets such as treatment, prednisone use or duration of disease. At this point we cannot comment on whether the novel radiological findings discussed here are unique to SLE or could be found in other diseases. However, separating lupus arthritis from other diseases was not an aim of the study. At this time, we cannot comment on response to change as we have not reported any longitudinal follow-up. Thus, we do not know the MRI features that are most likely to have response to typical therapies. Nearly all of these patients were on immunosuppression in addition to hydroxychloroquine still with the persistent findings described here. This observation alone suggests the need for more specific therapies for lupus arthritis. MRI, although expensive in the USA, if shown to be responsive to clinical change, may have utility in a research setting for the assessment and monitoring of lupus arthritis, allowing smaller trials of a single endpoint.
References
Footnotes
Contributors ESZ: designed the study, acquisition and analysis of data, drafted the manuscript, and final approval. MH: designed the study, analysis of data. BW: designed the study, analysis of data. RC: designed the study, acquisition and analysis of data.
Funding This study was funded by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (grant number P60 MCRC AR062755) and NIH-NCATS (grant number UL1TR001450).
Competing interests None declared.
Patient consent Not required.
Ethics approval The study was approved by the MUSC IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data statement None.