Article Text

Abstract
Background SLE is an autoimmune condition affecting predominantly women. Little is known regarding Chlamydia trachomatis infection in women with SLE, which may drive autoimmunity and contribute to obstetrical and vascular complications.
Methods This single-centre, case–control study set primary endpoint in the comparative seropositivity rate to C. trachomatis major outer membrane protein (MOMP) and chlamydial heat-shock protein-60 (cHSP60) in age-matched subjects. The secondary endpoints were obstetrical outcomes, cardiovascular events and results from screening procedures for cervical cancer.
Results Eighty-four women with SLE and 50 age-matched controls were included. Seropositivity to C. trachomatis did not differ significantly between groups (10% of cases positive for anti-MOMP vs 12% of controls; 43% of cases positive for anti-cHSP60 vs 32% of controls). Women with SLE were more often of non-Caucasian ethnicity and had lower educational level. They relied less frequently on oral contraception and resorted more frequently to elective pregnancy termination. Pre-eclampsia and ectopic pregnancy occurred only in SLE. Women with SLE also experienced more cardiovascular events. In SLE, antibodies to cHSP60 were associated with a history of pericarditis and abnormal screening tests for cervical cancer. Antibody titres to C. trachomatis were not associated with disease activity or SLE treatment, nor were there associations with other gynaecological, obstetrical or vascular outcomes.
Conclusion Prevalence of antibodies to C. trachomatis was not increased in women with SLE. No significant association was found between these antibodies and obstetrical or cardiovascular complications.
- systemic lupus erythematosuschlamydia trachomatis
- i>, heat-shock protein 60, reproductive health, cardiovascular events
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
- systemic lupus erythematosuschlamydia trachomatis
- i>, heat-shock protein 60, reproductive health, cardiovascular events
Introduction
SLE is a chronic inflammatory disorder characterised by multiorgan damage and the generation of a vast array of autoantibodies. SLE mainly affects women of reproductive age. The strong gender predilection suggests that sexual hormones are involved in disease pathogenesis and progression, but gender-specific genetic and environmental differences may also be implicated.1–3 It has been postulated that the autoimmune processes underlying SLE may be triggered by certain pathogens in genetically susceptible individuals. One prime candidate is Epstein-Barr virus,4 although results regarding its implication in SLE are conflicting. Information on the role of sexually transmitted pathogens in SLE is limited. Chlamydia trachomatis is a common sexually transmitted obligatory intracellular bacteria. Infection with C. trachomatis usually results in urethritis in men and cervicitis in women. In women, C. trachomatis infection is frequently clinically silent, and some develop endometritis, salpingitis or pelvic inflammatory disease, which may lead to ectopic pregnancy, miscarriage and tubal infertility.5 6 About 10% of individuals in the general population have antibodies to C. trachomatis.7–9 In Switzerland, C. trachomatis seroprevalence and C. trachomatis prevalence assessed by quantitative PCRs in urogenital samples are similar to those in other European countries, being respectively 10%6 and 5%.10 This prevalence of chlamydia DNA was slightly lower (about 2%) in young asymptomatic Swiss men.11 C. trachomatis infection has been linked to reactive arthritis, an autoimmune entity mostly diagnosed in male subjects.12 C. trachomatis produces microbial heat-shock proteins (HSP), such as chlamydial HSP60 (cHSP60), a stress molecule with a high degree of homology between species.13–15 Thus, infection with C. trachomatis may trigger an immune response with generation of anti-cHSP60 antibodies, which could cross-react with human HSP60. Human HSP60 is expressed on endothelial cells. HSP60-reactive T cells as well as anti-HSP60 antibodies have been linked to atherosclerosis.16 In SLE, the presence of antibodies to human HSP60 was associated with increased arterial vascular events, when associated with antiphospholipid antibodies.17 Accelerated atherosclerosis is of particular concern in SLE. Based on the role of C. trachomatis in autoimmunity and vascular damage, we hypothesised that infection with C. trachomatis may be more prevalent in women with SLE. A study in patients with reactive arthritis had indeed found an increased seroprevalence of antibodies to C. trachomatis in controls with SLE compared with healthy subjects, although this difference was not statistically significant.18 Serology for C. trachomatis, both against chlamydial major outer membrane protein (MOMP) and cHSP60, has a limited sensitivity for acute infection.19 It is however the most reliable tool to assess past infection. A positive serology tends to be associated with more severe infections (eg, pelvic inflammatory disease).20 Our main objective was to investigate the prevalence of both antibodies to C. trachomatis MOMP and to the less specific cHSP60 in female patients with SLE, compared with age-matched controls. We also investigated pregnancy outcomes and cardiovascular events in both groups, as these are of particular concern in women with SLE21 22 and because of their potential link with C. trachomatis infection.
Methods
We conducted a case–control study between 15 December 2014 and 13 April 2015. All participants were recruited sequentially. Cases were female adults with SLE attending the outpatient clinic of Lausanne University Hospital. Controls were women attending the same outpatient clinic for allergy tests. Cases and controls were matched per decade of age, in order to obtain the same age distribution between groups. All participants provided a blood sample and completed a questionnaire on reproductive health outcomes. Additional information was gathered from hospital files and gynaecologists’ records, when available. Inclusion criteria for cases were definite SLE according to the revised American College of Rheumatology (ACR)23 and/or the Systemic Lupus International Collaborating Clinics criteria.24 Cases were recruited into the Swiss SLE Cohort Study and assessed according to a detailed questionnaire on SLE features. Exclusion criteria for controls were evident autoimmunity or non-allergic inflammatory conditions. Exclusion criteria for both groups were active neoplasia or infection.
The questionnaire assessed demographical, gynaeco-obstetrical and cardiovascular variables. Data included age at menarche, age at first intercourse, means of contraception, number of sexual partners, number of pregnancies and pregnancy outcomes, occurrence of menopause and frequency of gynaecological follow-up. Additional data were extracted from the hospital medical file and obtained from gynaecologists in private practice through a telephone interview, and included details on screening procedures for cervical cancer (Pap test according to Bethesda classification, and where available colposcopy and biopsy results), on pregnancy outcomes (spontaneous fetal losses, extrauterine pregnancies, preterm births before the 32nd week of gestation, pre-eclampsia defined as hypertension >140/90 mm Hg and proteinuria >300 mg/24 hours since the 20th week of gestation, and eclampsia defined as status epilepticus in a context of pre-eclampsia) and on thromboembolic events (significant ischaemic stroke translating in an acute neurological symptomatology, acute ST-elevation myocardial infarction (STEMI) or non-STEMI, unprovoked acute deep venous thrombosis and clinically significant acute pulmonary embolism; all cardiovascular events were documented by radiological findings or coronarography).
Serology against C. trachomatis was performed in all participants using ELISA, with IgG to C. trachomatis MOMP (Chlamydia trachomatis-IgG-pELISA; ref 497-TMB; Medac, Wedel, Germany) and HSP60 (cHSP60-IgG-pELISA; ref 435; Medac). The MOMP Medac assay is described as one of the most sensitive and specific commercially available, noticeably because it does not cross-react with C. pneumoniae MOMP and HSP60.25 Cross-reactivity of C. trachomatis anti-HSP60 with human anti-HSP60 is unknown and was not assessed in the present study. Intra-assay variability was 3.4% (coefficient of variation for MOMP assay) and 4.3% (coefficient of variation for cHSP60 assay), as reported by the manufacturer.
Relative luminescence (defined according to the manufacturer’s instruction) of 1.1 or more was considered as a positive result, and a relative luminescence of 0.9 or less was considered negative. Before analyses, we decided to consider borderline antibody titres 0.9–1.1 as negative.
Clinical information regarding lupus disease duration, activity according to Safety of Estrogens in Lupus Erythematosus National Assessment-Systemic Lupus Erythematosus Disease Activity Index (SELENA-SLEDAI) score,26 and past and present treatment was were documented for SLE cases.
Distribution comparisons (Student’s t-test) and bivariate analyses (χ2 and Fisher’s methods according to the number of cases) were used to assess differences between groups (group matching). P values under 0.05 were considered statistically significant. Missing values were excluded from analyses. Given the explorative nature of the study, we did not apply post-hoc procedures to correct for multiple comparisons.27 Analyses were conducted using SPSS V.22 for Windows.
Results
Baseline characteristics
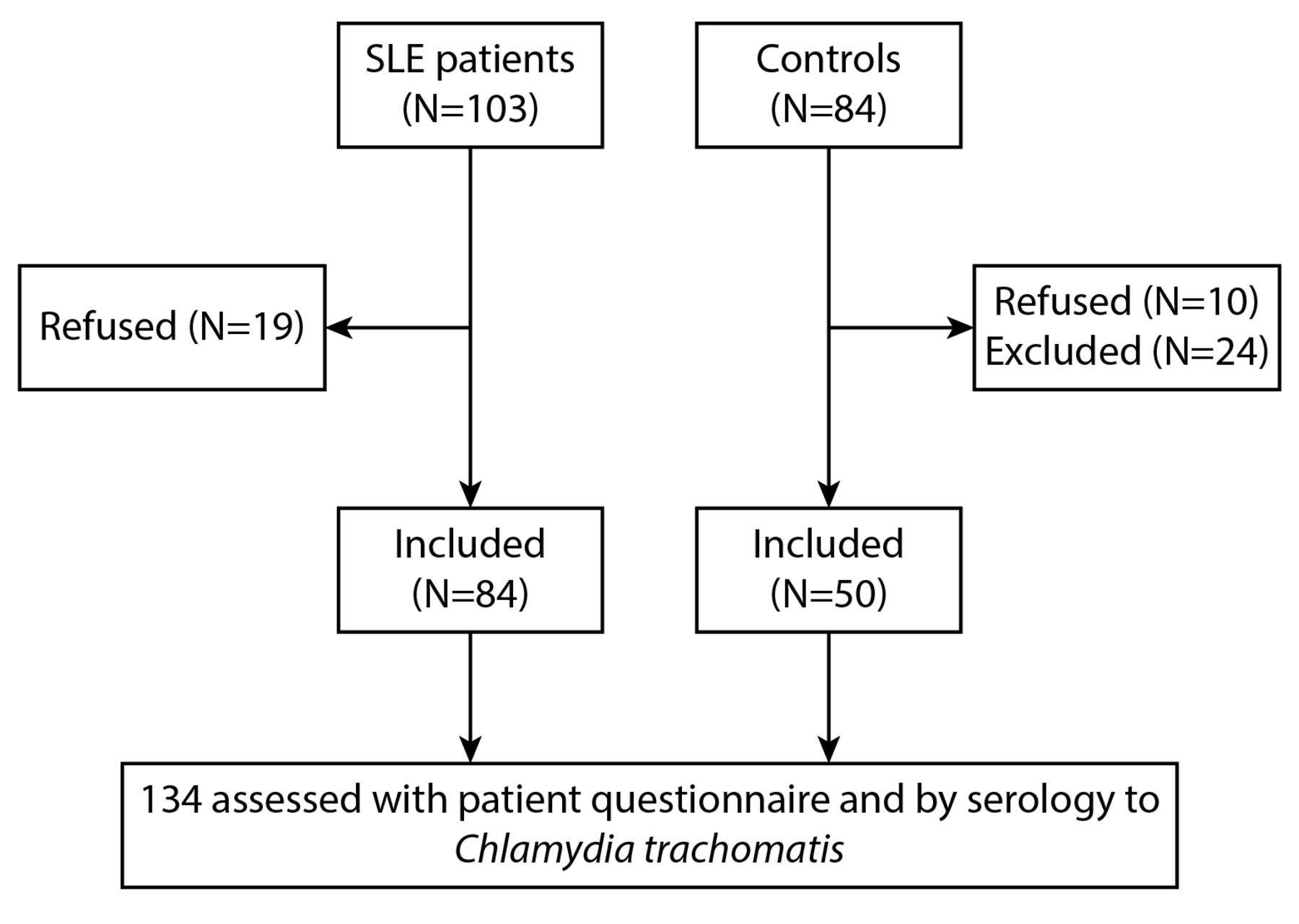
Eighty-four women with SLE and 50 age-matched controls were included (figure 1). The mean age at inclusion was 44 years. Demographics in women with SLE and controls are compared in table 1. Women with SLE significantly differed from controls with regard to ethnic background, with 58% being Caucasians, compared with 88% in the control group. Educational level also tended to be lower in the SLE group, with 57% having attended college, professional school or university, compared with 72% in the control group.
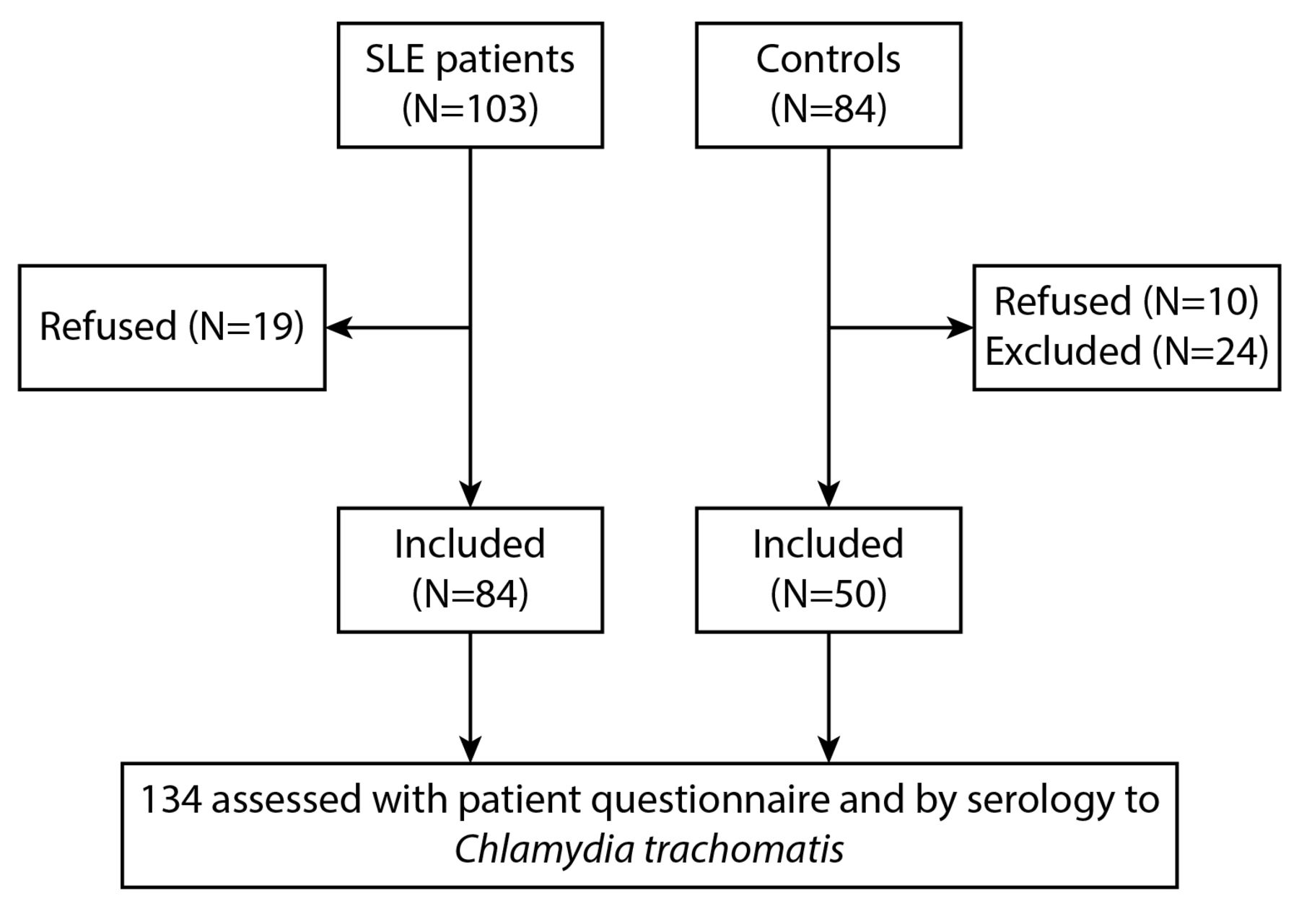
Study flow chart. Cases with SLE are on the left and age-matched controls are on the right. Controls excluded after screening had systemic autoimmunity (n=8), autoimmune endocrinopathy (n=6), chronic spontaneous urticaria (n=4), active neoplasia (n=3) and other unclear medical conditions (n=3; pulmonary transplant for cystic fibrosis, non-allergic asthma and pruritus of unknown origin).
Baseline characteristics of 84 women with SLE and 50 age-matched controls
There was no difference in age at menarche, age at first intercourse or number of sexual partners between groups. The use of oral contraceptives was significantly lower in SLE and reported by 66% of women, compared with 82% of controls. On the other hand, only women with SLE had received medroxyprogesterone acetate injections. Other means of contraception did not differ between groups. Forty-one (49%) women with SLE declared having reached menopause, compared with 18 (36%) of controls (NS). In the SLE group, 79% had seen a gynaecologist in the 2 years preceding inclusion, compared with 90% of controls (NS).
Primary outcomes
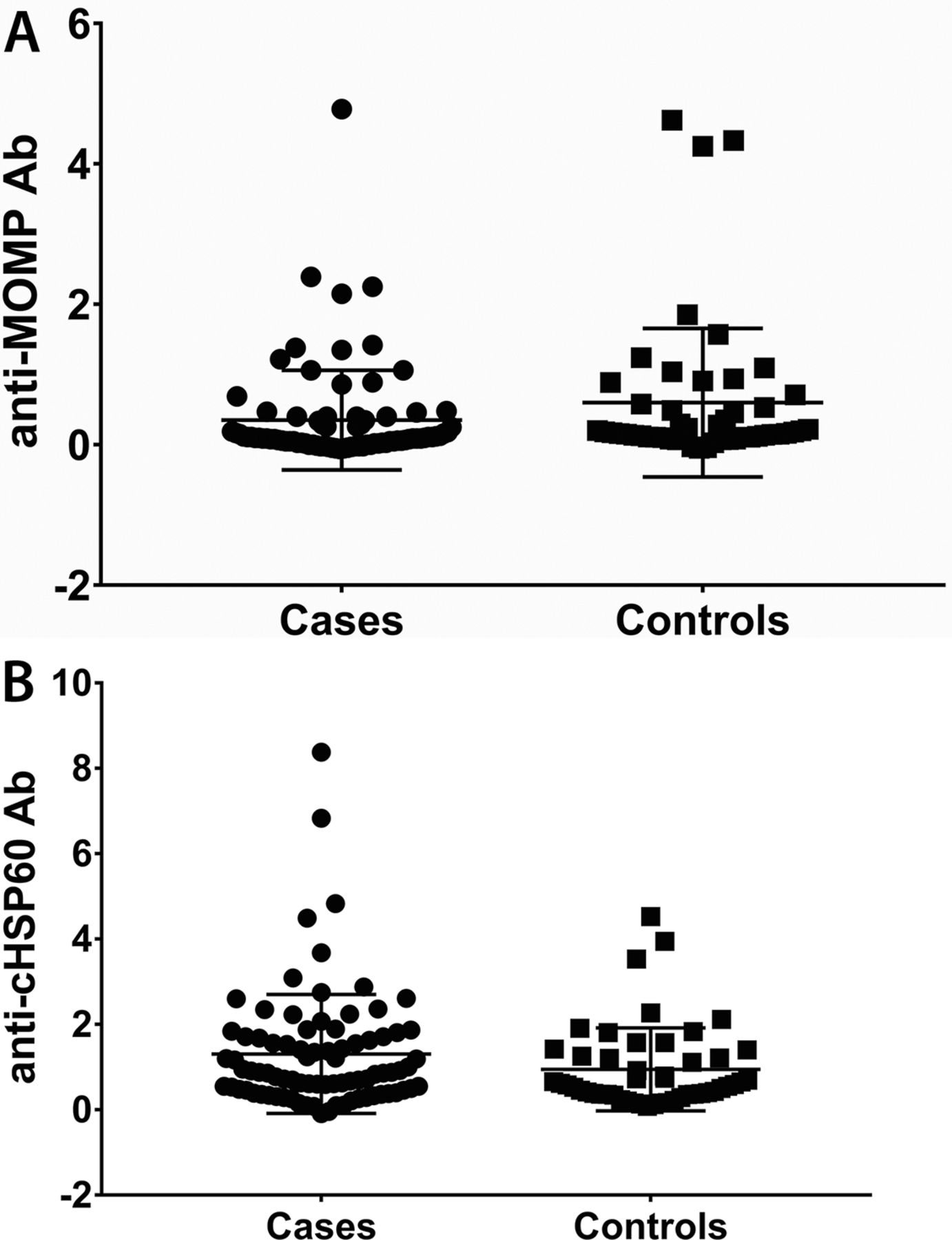
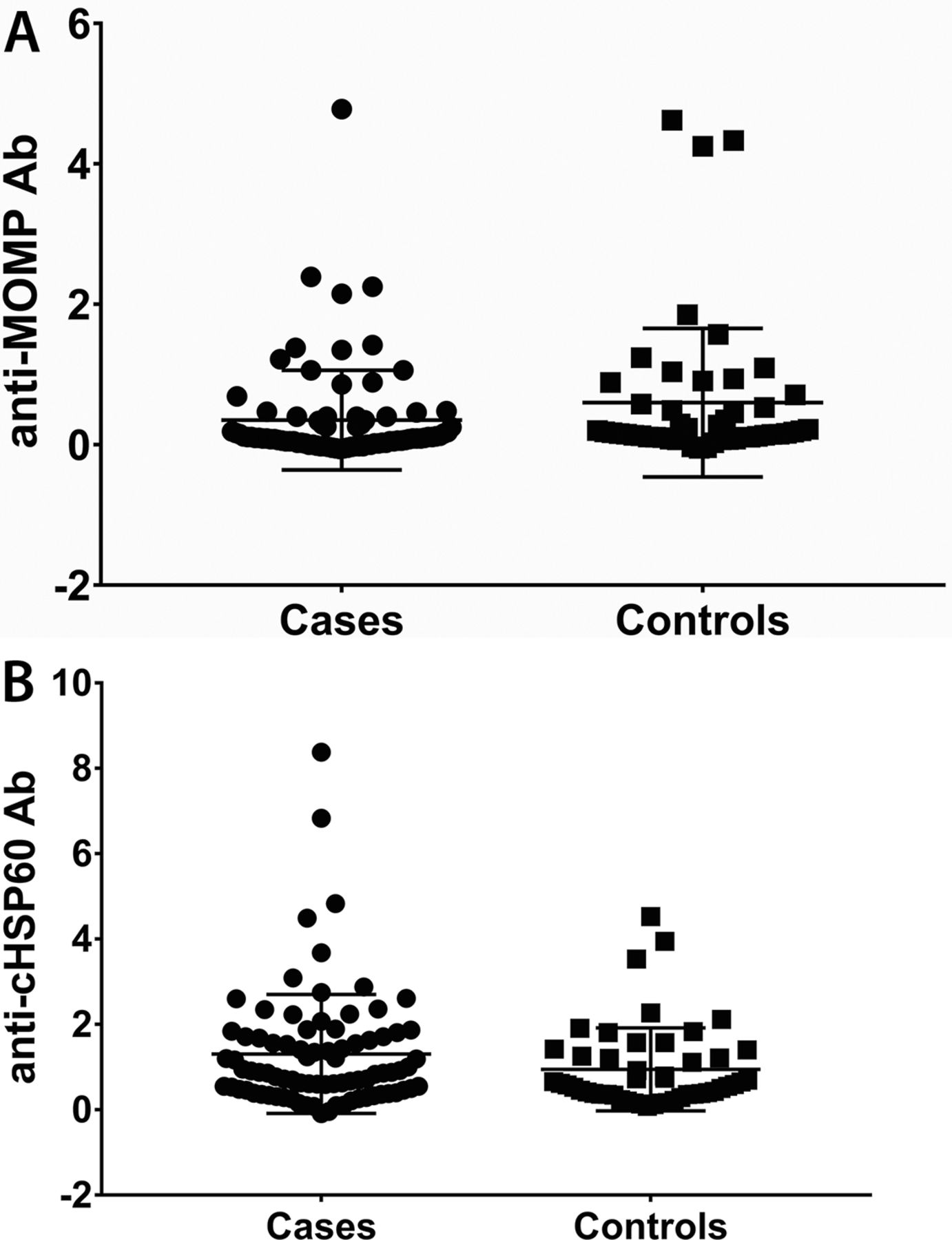
Antibody titres to C. trachomatis MOMP and cHSP60 are shown in figure 2. As expected, there was a moderate correlation between MOMP and cHSP60 antibody titres (Spearman’s r=0.29). The proportion of seropositives did not differ between groups, with 8 (10%) cases positive to MOMP compared with 6 (12%) controls, and 36 (43%) cases positive to cHSP60, compared with 16 (32%) controls (p=0.77 and p=0.27, respectively). The rate of seropositivity to C. trachomatis antigens did not correlate with age, socioeconomic background, ethnicity, early sexual activity, type of contraception used and number of sexual partners reported. Also, seropositivity to MOMP or cHSP60 was not associated with historical results for C. trachomatis vaginal swab testing, although only performed in 25% of patients and exceptionally positive. Finally, seropositivity was not associated with self-reported C. trachomatis infection (data not shown).
{kind=link}
{kind=link}
Antibody (Ab) titres to Chlamydia trachomatis major outer membrane protein (A) and chlamydial heat-shock protein-60 (cHSP60) (B) in 84 women with SLE (cases) and 50 age-matched controls.
Secondary outcomes
Pregnancy rates did not differ between groups (71% of patients in the SLE group and 72% of controls). Obstetrical outcomes are shown in table 2. There was no difference in the number of live births and spontaneous fetal losses. Extrauterine pregnancies were reported in three patients with SLE and did not occur in controls. Elective abortions were more frequent in SLE and reported by 48% of women with pregnancies, compared with 22% of controls. Pre-eclampsia, eclampsia and hemolysis, elevated liver enzymes, low platelet count (HELLP) syndrome occurred only in the SLE group and were reported in 10% of patients with pregnancies. No association was observed between elective abortion or any pregnancy complication (fetal losses, prematurity in subjects with SLE or in controls; extrauterine pregnancy, pre-eclampsia/eclampsia in subjects with SLE) and either anti-MOMP or anti-cHSP60 antibodies (data not shown).
Pregnancy outcomes in 60 women with SLE and 36 age-matched controls
Cardiovascular events are listed in table 3. Taken together, arterial and venous vascular events had occurred in 29% of women with SLE, compared with 4% of controls (p=0.001). This difference was mainly due to venous thromboembolism, which had only occurred in patients with SLE. Stroke and myocardial infarction were more frequent in SLE, although not statistically significant. Patients with arterial vascular events were older than those without, although this was not statistically significant (median age 51 years compared with 43; p=0.055). Within the SLE group, vascular events occurred in 15 of 41 (37%) of those without a history of positive testing for antiphospholipid antibodies, compared with 7 of 42 (16%) of those negative (p=0.047). This association was only seen with arterial vascular events, which occurred in 10 patients positive to antiphospholipid antibodies, compared with 1 patient negative to antiphospholipid antibodies (p=0.003). No association was found between cardiovascular events (stroke, myocardial infarction, pulmonary embolism, deep venous thrombosis) and either anti-MOMP or anti-cHSP60 antibodies, in patients with SLE or in controls (data not shown). The results from screening procedures for cervical cancer were available in 80% of participants, with abnormal tests reported in 30% of screened subjects with SLE and 27% of controls (NS). Findings were atypical squamous cells of undertermined significance (ASC-US) in 8 patients, low-grade squamous intraepithelial lesions/cervical intraepithelial neoplasia-grade 1 (LSIS/CIN-1) in 15, high-grade squamous intraepithelial lesions/cervical intraepithelial neoplasia-grade 2-3 (HSIL/CIN2-3) in 7, and 1 had an unspecified abnormal result.
Cardiovascular events in 84 women with SLE and 50 age-matched controls
Association of serological results within the SLE group
Disease characteristics and treatment modalities of patients with SLE are shown in table 4. Subjects with SLE had a median disease duration of 8 years and fulfilled a median number of 6 ACR classification criteria for SLE. Most patients with lupus suffered from photosensitive rash, arthritis and haematological disorder. Forty-three (52%) had lupus nephritis, with four patients under permanent dialysis or one having received a kidney graft. The median SELENA-SLEDAI score was 5, consistent with moderately active SLE in most patients. Seventy-one per cent of patients were taking antimalarials, and approximately half were taking low-dose corticosteroids and/or immunosuppressants during the month preceding assessment. The most frequently used immunosuppressant was mycophenolate mofetil (45% of subjects under immunosuppression). Twelve patients received biologics at the time of assessment (rituximab in 6, belimumab in 4, abatacept in 1 and tocilizumab in 1 patient). Seventy-five per cent of patients had been under immunosuppressant therapy at least once during the course of the disease.
Disease features of 84 patients with SLE according to cHSP60 serology
Patient characteristics with regard to cHSP60 serology are shown in table 4. Those positive for cHSP60 antibodies had more often a history of pericarditis (42% in cHSP60-positive, compared with 19% in cHSP60-negative; p=0.03). As previously reported, there was no significant association between cHSP60 seropositivity and vascular events (17% of arterial events in cHSP60-positive, compared with 10% in cHSP60-negative). There was no significant association of antibodies to cHSP60 with other disease features, including global disease activity and treatment modalities. No associations between anti-MOMP and clinical characteristics were found (data not shown).
There was a significant association between anti-cHSP60 and abnormal Pap smear results in patients with SLE (50% with abnormal results in patients with anti-cHSP60 antibodies, compared with 16% in patients without these; p=0.004). No such difference was found in controls, nor was seropositivity to MOMP associated with cervical dysplasia in either group.
Discussion
In this single-centre study, prevalence of antibodies to chlamydial MOMP and cHSP60 did not significantly differ between women with SLE and age-matched controls. The seroprevalence of 10% specific antibodies to C. trachomatis we found is similar to the reported frequency of C. trachomatis exposure in the general Swiss6 and European female population.8 9 Only a minority of subjects had undergone vaginal swab tests for C. trachomatis, and serology did not correlate with these findings nor with self-reported C. trachomatis infection. When comparing known risk factors for sexually transmitted diseases such as early onset of sexual activity and increased number of sexual partners, we did not find a significant association with serology results nor differences between SLE and controls. Aside from these classic risk factors, contraceptive methods differed between SLE and controls, with lower use of combined oral contraceptive in women with SLE and higher use of medroxyprogesterone acetate injections (likely secondary to SLE diagnosis). A higher rate of elective abortion in patients with SLE may reflect a lower socioeconomic status and reduced access to effective contraception. Cases and controls differed in terms of ethnicity, with more patients with SLE being of African or Asian descent. In addition, fewer patients with SLE had achieved higher professional education compared with controls. This may reflect the increased prevalence of SLE in ethnic minorities and lower socioeconomic status.28 29 Only women with SLE did experience pre-eclampsia, which is a well-known risk in this population.30 Ectopic pregnancies were reported by three patients, all in the SLE group. However, the rate of live births was the same in SLE and controls. No association between pregnancy outcomes and seropositivity to C. trachomatis was found. These results contrast with previous observations suggesting a relationship between miscarriage and C. trachomatis infection.6 31 Cardiovascular events were significantly more frequent in women with SLE compared with age-matched controls. Indeed, accelerated atherosclerosis and thrombotic events linked to antiphospholipid antibodies are feared complications of SLE. Most of our patients with lupus had long-standing disease and half had severe disease with renal involvement. While vascular events were more frequent in patients with SLE with antiphospholipid antibodies, we did not find an association with antibodies to MOMP or cHSP60.
Very few studies have assessed exposure to C. trachomatis in SLE. One study on reactive arthritis had included 30 patients with SLE, which displayed a threefold increase in seroprevalence against C. trachomatis compared with healthy controls.18 A study assessed C. trachomatis by vaginal swab test and did not find an increased prevalence in patients with SLE.32 Another study investigated the potential relationship between coronary calcifications as a marker of atherosclerotic burden and PCR for C. pneumoniae and C. trachomatis in the peripheral blood monocytes of patients with SLE, without finding a clear association.33 Most patients with SLE included in our study had disease features beyond articular and cutaneous involvement. A majority had received immunosuppressive treatment. Most patients had long-lasting and well-controlled disease at assessment. Antibodies to cHSP60 were slightly more prevalent in SLE and were associated with a history of lupus pericarditis. Others have found that a history of lupus pericarditis might define a subgroup of patients with more aggressive disease.34 We did not find an association of anti-cHSP60 antibodies with other features of severe SLE, although more patients in this group had end-stage renal disease. A possible explanation for an association of antibodies to cHSP60 with pericarditis could be the tendency of Chlamydia species to induce serositis, as in the Fitz-Hugh-Curtis syndrome or in some reported cases of pericarditis and myocarditis.35 However, no association between anti-MOMP antibodies and pericarditis was found. Another finding with regard to anti-cHSP60 antibodies was their association with abnormalities on screening tests for cervical cancer. One could argue that human papilloma virus (HPV) usually underlying cervical dysplasia might be transmitted together with C. trachomatis, as coinfection frequently occurs and facilitates oncogenesis,36 a finding reflected by the presence of antibodies to cHSP60. On the other hand, no association between cervical dysplasia and antibodies to C. trachomatis MOMP was found that would support this hypothesis. More studies relying on PCR techniques are needed to assess the role of HPV and C. trachomatis coinfection in SLE. Upregulation of HSP60 expression has been reported in women with cervical cancer.37 One could argue that upregulation of HSP60 by dysplastic cells in the cervix might trigger cross-reactive antibodies, given the high grade of homology with cHSP60. We did however not assess whether antibodies to cHSP60 cross-react with human HSP60, which was beyond the scope of this study. It is finally possible that due to the multiplicity of statistical tests performed, the association of anti-cHSP60 antibodies with pericarditis and cervical dysplasia in the lupus subset is due to chance. We did not find an increase in cervical dysplasia in patients with SLE compared with controls. However, larger population-based studies have shown that cervical dysplasia is an important issue in SLE and that the risk increases in women with long-standing immunosuppression.38
Although this study has limitations, such as its cross-sectional design and the limited sample size, its strengths lie in the detailed assessment of participants and the use of two reliable and complementary serological tests for C. trachomatis. We considered the possibility that infection with C. trachomatis might drive autoimmunity in SLE, but the results show an equal distribution of antibodies to C. trachomatis in age-matched controls, which speaks against a prominent role of this pathogen in lupus and associated damage. Studies relying on PCR techniques to detect ongoing infection with C. trachomatis in patients with early lupus are needed to confirm these results. Our study results also support known issues in women with SLE, which are increased risk of adverse obstetrical outcomes and cardiovascular events.
Acknowledgments
We thank the study participants, the nurses of the Department of Ambulatory Care and Community Medicine, André Cyril and Vincent Aubert of the Diagnostics Laboratory of Immunology in CHUV Lausanne for their help and Carlo Chizzolini of the Geneva University Hospital Geneva for his review of the participant questionnaire.
References
Footnotes
Contributors AS: conception of the work; acquisition, analysis and interpretation of data for the work; drafting the work; final approval of the version to be published; agreement to be accountable for all aspects of the work. GG: contribution to the conception of the work; interpretation of data for the work; revising the work critically; final approval of the version to be published; agreement to be accountable for all aspects of the work. SA: acquisition of data; revising the work critically; final approval of the version to be published; agreement to be accountable for all aspects of the work; DW: contribution to the conception of the work; interpretation of data for the work; revising the work critically; final approval of the version to be published; agreement to be accountable for all aspects of the work. GP: interpretation of data for the work; revising the work critically; final approval of the version to be published; agreement to be accountable for all aspects of the work. CR: conception of the work; analysis and interpretation of data for the work; drafting the work; final approval of the version to be published; agreement to be accountable for all aspects of the work.
Funding Association of the Swiss SLE Cohort Study (ASSCS) unrestricted grant from USB to Carlo Chizzolini, Geneva University Hospital and Medical School.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study was approved by the local ethics committee (Commission cantonale d'éthique de la recherche sur l'être humain, VD, CH) on 15 December 2014 (protocol n° 470/14).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.