Article Text

Abstract
Objectives Lupus nephritis (LN) requires renal replacement therapy in 10%–30% of patients. About 30% of these patients receive a kidney transplant. Belatacept is a second-generation, selective, T-cell co-stimulator blocker (inhibits cytotoxic, T-lymphocyte antigen 4, CTLA-4) used as an alternative to calcineurin inhibitors (CNI) for maintenance regimens after kidney transplantation. The pathogenic relevance of CTLA-4 inhibition and the favourable cardiovascular profile of belatacept make it an attractive therapeutic option in systemic lupus erythematosus (SLE). Intravenous administration of belatacept ensures therapeutic adherence.
Methods This retrospective, single-centre study evaluates the outcomes of LN kidney transplant recipients treated with belatacept for reasons not related to SLE at the Columbia University Lupus and Renal Transplant Cohort.
Results Belatacept was started in six patients on CNI regimens at 15.5±17.1 months following transplantation for LN. In five patients, creatinine levels stabilised 6 months after belatacept, one returned to haemodialysis due to CNI toxicity and pyelonephritis and one relisted for a kidney transplant following acute cellular rejection and cortical necrosis. Five patients are followed for extrarenal lupus; no extrarenal manifestations were documented in the other two patients. Data on SLE disease activity pre-belatacept and post-belatacept were available and scored in three patients using the SLE Disease Activity Index Glucocorticosteroid Index (SLEDAI-2KG), which accounts for clinical and laboratory manifestations, as well as steroid dose. Mean SLEDAI-2KG decreased from 13 to 7.6.
Conclusion Belatacept in LN kidney transplant recipients may decrease extrarenal manifestations, attenuate CNI toxicity and stabilise allograft function, providing a better alternative to CNI regimens. Furthermore, these data suggest that belatacept, although initiated for reasons not related to SLE, might have a beneficial effect in SLE.
- autoimmune diseases
- lupus nephritis
- systemic lupus erythematosus
- Treatment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune, multisystemic disease, which primarily affects women of childbearing age. Among its multiple manifestations, lupus nephritis (LN) is the main cause of morbidity and mortality in SLE.1 The prevalence of LN is 30.9/100 000 habitants in the USA.2 Ten to thirty percent of patients with LN eventually progress to end-stage renal disease (ESRD) within 15 years of diagnosis,3 and about 30% eventually become kidney transplant recipients.4 LN decreases life expectancy by 15.1 years compared with patients without renal involvement.5
Belatacept is a cytotoxic, T-lymphocyte antigen 4 (CTLA-4) immunoglobulin human fusion protein that acts as a selective T-cell co-stimulation blocker by inhibiting the CD28-CD80/86 costimulatory pathway. It differs from abatacept by two amino acids. Belatacept binds to CD80 and CD86 with approximately twofold and fourfold higher avidity, respectively, resulting in a 10‐fold increase in the biological potency compared with abatacept.6 Although abatacept failed to achieve the primary endpoint in several SLE clinical trials, CTLA-4 inhibition likely has a significant role in the treatment of lupus.7 Belatacept, with greater potency and similar mechanism of action, could show promise in SLE.
Belatacept-based immunosuppression, as compared with cyclosporine (CYC)-based immunosuppression, is associated with similar patient and graft survival and significantly improved renal function in kidney-transplant recipients.8 Switching from a calcineurin inhibitor (CNI)-based regimen to belatacept is a therapeutic option in SLE kidney transplant patients in a number of indications including in the setting of CNI nephrotoxicity, moderate/severe interstitial fibrosis and tubular atrophy (IFTA) or moderate/severe arteriosclerosis. In addition, belatacept regimens ensure some degree of therapeutic adherence for patients with complicated drug regimens. The current study was conducted to evaluate the effect of belatacept on allograft function in SLE transplant recipients.
Methods
Single-centre, cross-sectional study of adult kidney transplant patients with LN who were switched from CNI-based maintenance regimens to belatacept between June 2006 and June 2018. The decision to convert from CNI to belatacept was based on reasons unrelated to SLE diagnosis or lupus activity. Institutional Review Board approval was obtained and chart review was performed for patients with ESRD due to LN who had undergone kidney transplantation at Columbia University Irving Medical Centre. SLE was defined by American College of Rheumatology/Systemic Lupus International Collaborating Clinics (ACR/SLICC) criteria. LN was defined by International Society of Nephrology/Renal Pathology Society (ISN/RPS) criteria. Sociodemographic data, type of immunosuppression regimen, kidney allograft function and SLE activity were collected. Adherence was ascertained by clinician documentation. Biopsies of renal transplant recipients were performed as clinically indicated by decline in renal function or the onset of proteinuria.
All qualitative variables were analysed using descriptive statistics, calculating means, frequencies and SD. A p value<0.05 was considered statistically significantly different. Statistical calculations were performed using Stata/IC V.15.1.
Patient and public involvement
We did not involve patients or the public in our work as it is a cross-sectional study.
Results
In all, 48 patients with SLE were identified and included in the analysis. Of these, six were converted from CNI-based regimens to belatacept. Demographic and SLE data for patients converted to belatacept are presented in table 1A and B. All patients were women, with a mean age at SLE diagnosis of 19.67±3.27 years. The median interval and range between SLE diagnosis and kidney transplant was 15 (5–23) years. Two patients had native renal biopsies with LN Class V, three had combinations of features as defined by ISN-RPS (Class IV & VI, IV & III, IV & V). Native renal biopsy data for one patient was missing. All six patients were Epstein-Barr virus seropositive. The median and range follow-up time post-transplant was 39.8 (4–88) months.
Demographics and SLE characteristics of the six patients converted to belatacept
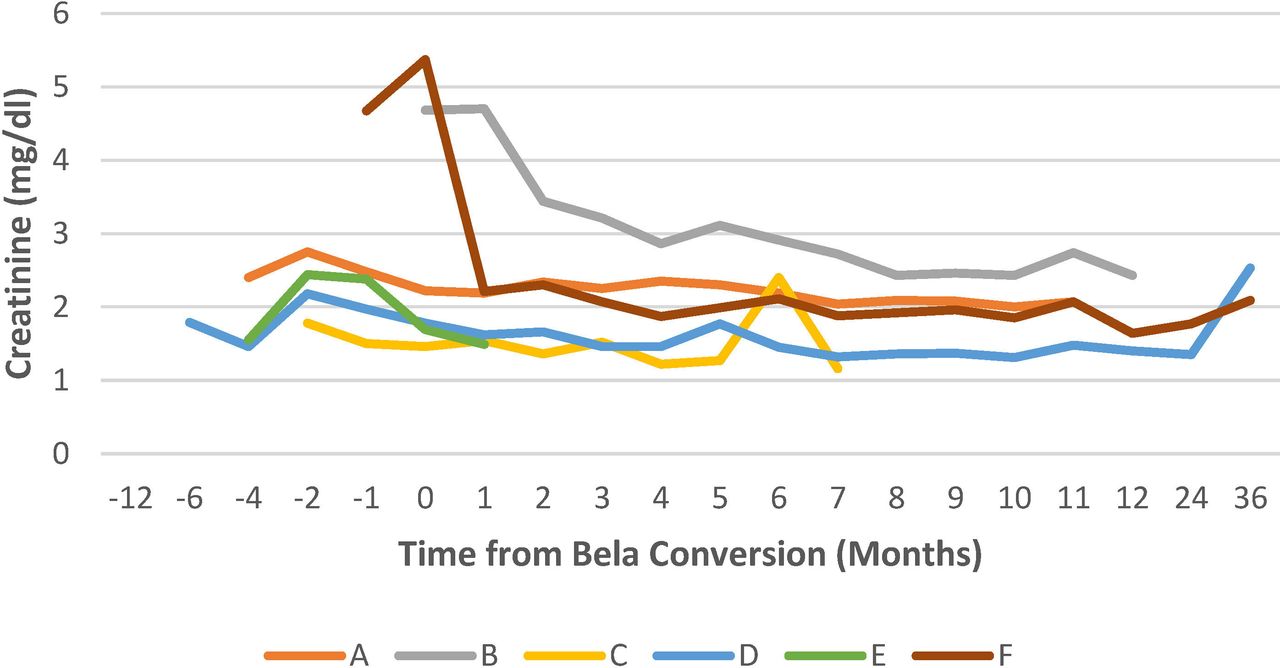
Four out of six transplant recipients patients (66.7%) received induction immunosuppressive therapy consisting of rabbit anti-thymocyte globulin (rATG), one with alemtuzumab (14%) and one with basiliximab (14%) which was followed by treatment of an acute cellular rejection episode with rATG. Maintenance regimens included tacrolimus (TAC) 9.2 mg ±1/day (n=5) or CYC 300 mg/day (n=1); mycophenolate mean dose 1520±488 mg/day (n=6), and prednisone at a mean dose of 5.8±3.8 mg/day (n=5). The decision to switch from a CNI-based regimen to belatacept was individualised. Three patients had treatment changed to belatacept because of CNI side effects, one because of non-adherence to oral treatments, one due to biopsy proven thrombotic microangiopathy (TMA) and one due to cortical necrosis. In transitioning to belatacept, CNI dose weaning was not standardised. Six months after switching to belatacept, five of six patients were still on concomitant CNI maintenance immunosuppression. Belatacept conversion dosing was performed with a dose of 5 mg/kg belatacept every 2 weeks for a total of 10 weeks (five doses total), then monthly 5 mg/kg dosing. Characteristics of kidney transplant and immunosuppressive regimens are detailed in table 2A and B. In four patients, the addition of belatacept was prompted by worsening allograft function. Three patients had improvement of renal function after conversion to belatacept, one progressed to ESRD on haemodialysis due to CNI toxicity and pyelonephritis (patient E), and one had progression of renal failure following ACR and cortical necrosis but not yet on dialysis, being evaluated for second kidney transplant (patient C). Recurrent LN class V was noted in one of the six patients, but it did not lead to graft failure. Variations in renal function before and after belatacept initiation are shown in figure 1.
Immunosuppression and KT characteristics of the six patients converted to belatacept

Creatinine trend before and after belatacept.
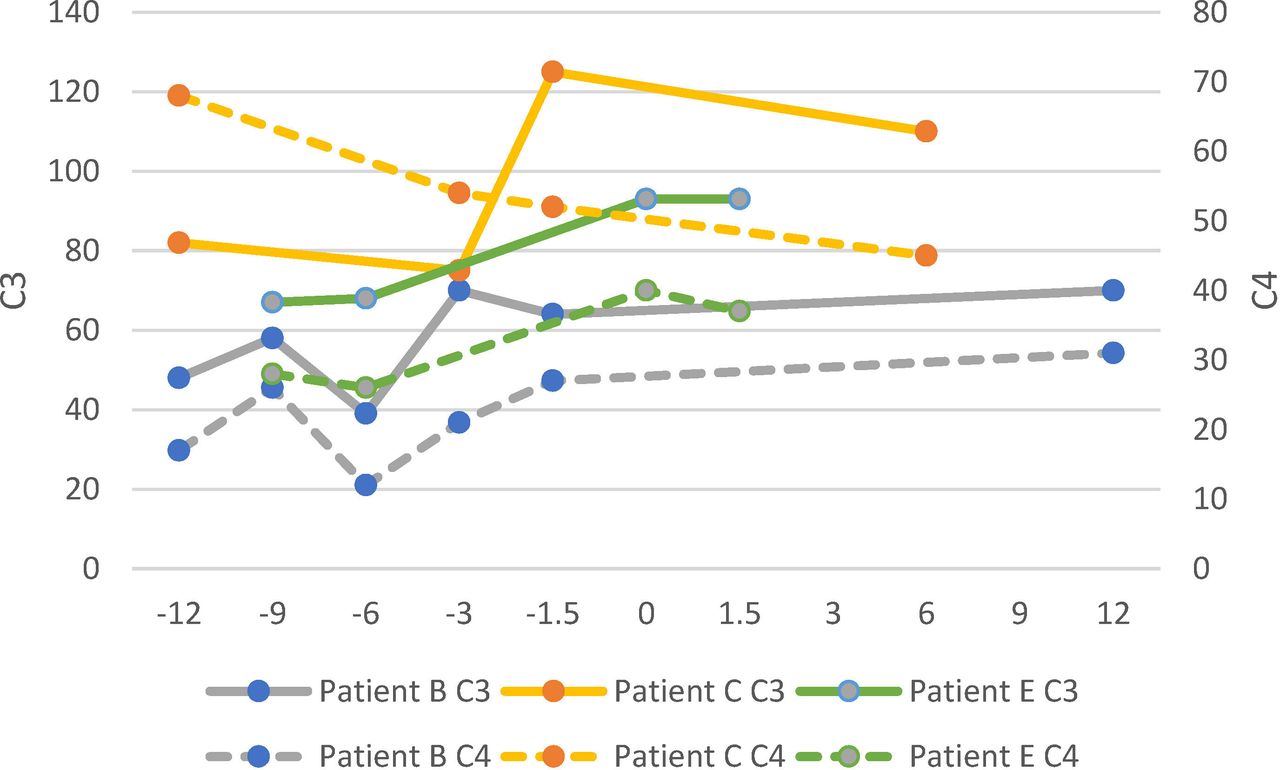
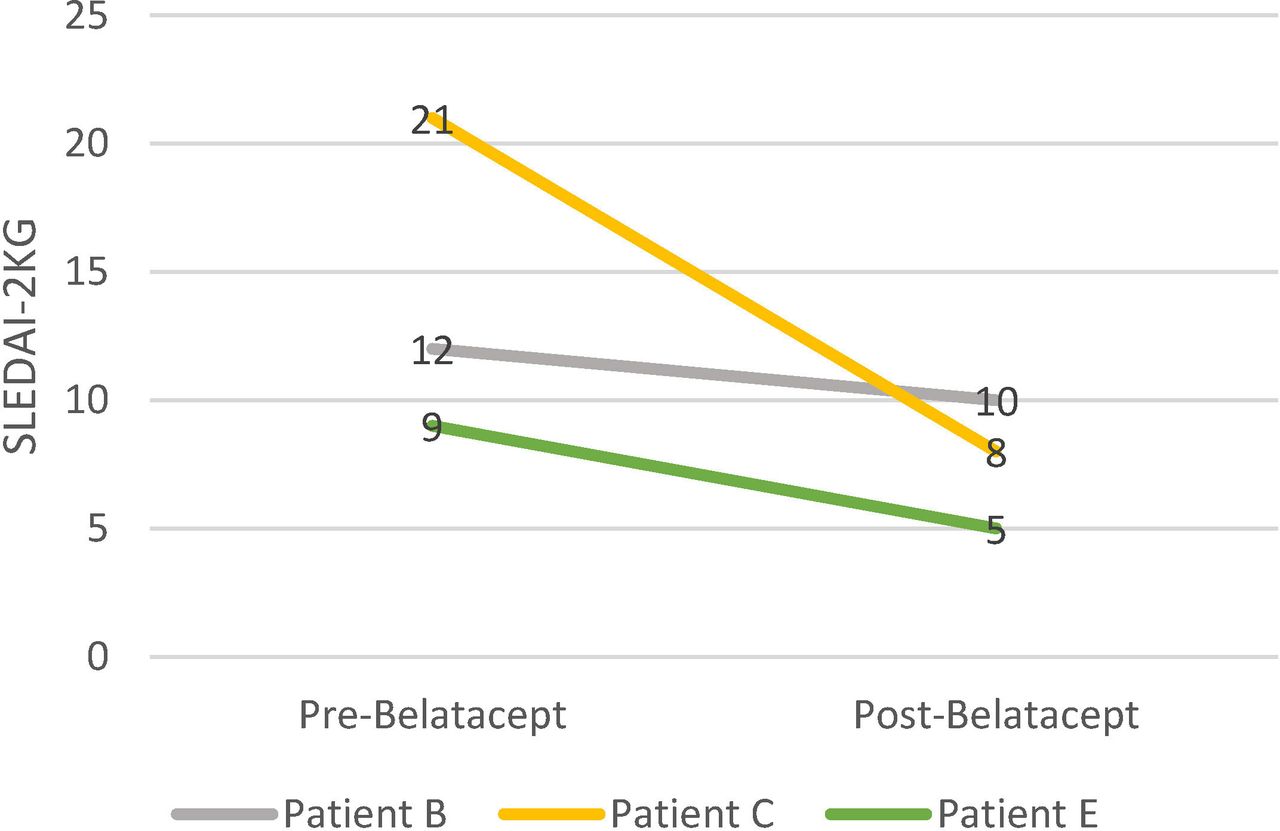
Five patients were also monitored by Rheumatology for persistent extrarenal lupus. No extrarenal manifestations were documented in the remaining two patients. SLEDAI and serological data could only be retrieved for three patients followed by rheumatologists at our centre. SLEDAI data were available and scored using the SLEDAI-2KG, which accounts for clinical and laboratory manifestations as well as steroid use, at a mean follow-up of 23.83±19.25 months after initiation of belatacept (figure 2). Mean ds-DNA value pre-belatacept was 133±178 UI/mL and 58±72 UI/mL post-belatacept. Mean C3 pre-belatacept and post-belatacept was 89±31 mg/dL and 91±21 mg/dL. Mean C4 35±15 mg/dL and 38±7 mg/dL, respectively. Figures 3 and 4 demonstrate trends in ds-DNA, C3 and C4 pre-belatacept and post-belatacept conversion.
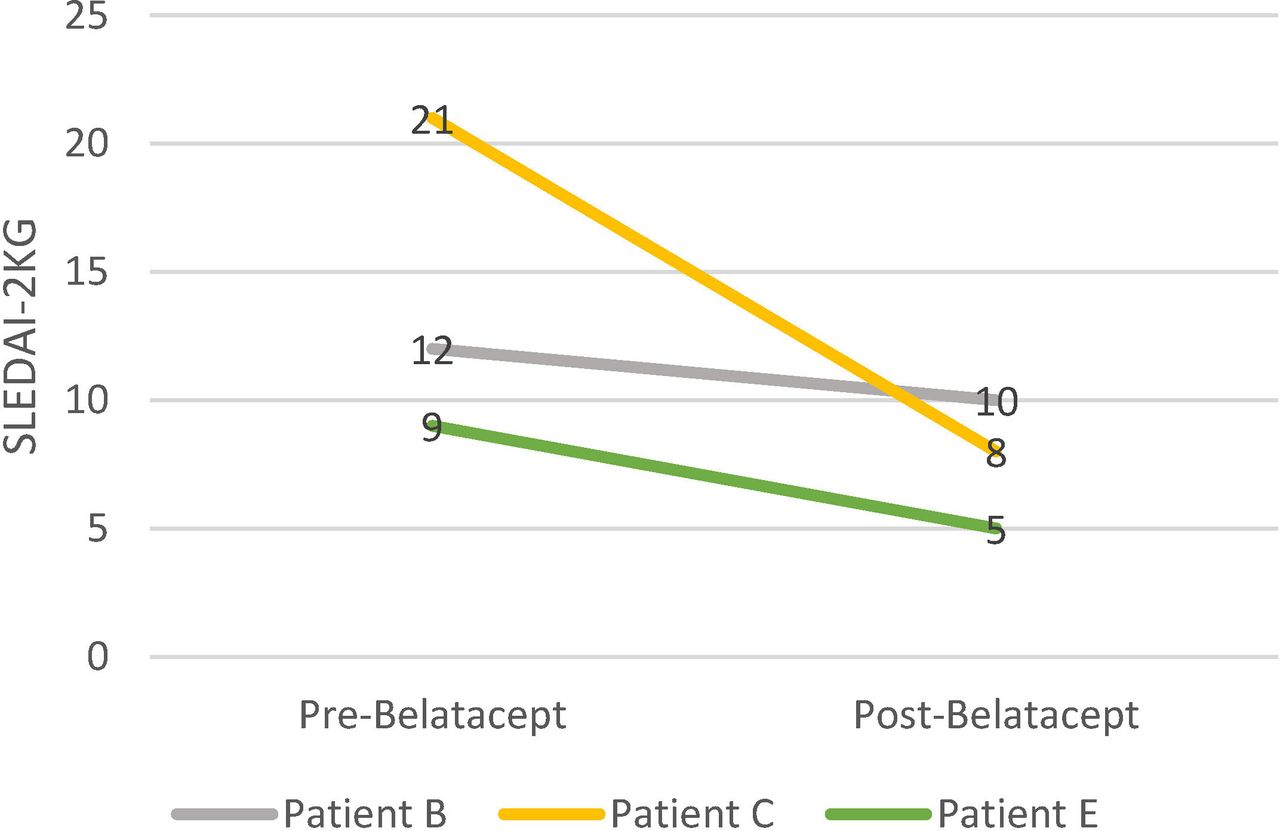
SLEDAI-2KG before and after belatacept.

Changes on ds-DNA antibodies levels pre-belatacept and post-belatacept.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes on complement C3 (left axis, continuous line) and C4 levels (right axis, discontinuous line) pre-belatacept and post belatacept.
Discussion
Patients converted to belatacept with or without withdrawal of CNI demonstrated a trend towards stabilisation of allograft function and lower SLEDAI-2KG following kidney transplantation. The SLEDAI-2KG decreased from a mean of 13 to 7.6, dsDNA and complement levels demonstrated improvement in three patients and allograft function stabilised in five patients. These data are the first to evaluate belatacept in SLE transplant recipients and to substantiate a possible role for this CTLA-4 inhibitor in the maintenance regimens of SLE kidney transplant patients and, although not specifically evaluated for SLE activity, a possible role in SLE.
Belatacept is currently used as an alternative treatment to CNI in the maintenance regimen of kidney transplant patients. Two phase III clinical trials, the Belatacept Evaluation of Nephroprotection and Efficacy as First-line Immunosuppression Trial (BENEFIT)8 and the Belatacept Evaluation of Nephroprotection and Efficacy as First-line Immunosuppression Trial-EXTended criteria donors (BENEFIT-EXT)9–11 showed no difference in the rates of patient survival, graft survival, and acute rejection in both low- and high-intensity belatacept regimen groups compared with the CNI group. Improved cardiovascular profile, better blood pressure, better lipid profile, lower incidence of diabetes mellitus, significantly less chronic kidney scarring and sustained improved renal function at 3 years post-transplantation were noted in the belatacept group. The increased rate of post-transplant lymphoproliferative disorder, particularly in Epstein-Barr seronegative patients, identified during the initial trials remains to be fully evaluated. In our cohort, three patients were switched to belatacept due to CNI side effects. One suffered from CNI neurological side effects (tremors, headaches and brain fog) documented by clinical history and physical examination, attributed to CNI regimens due to a clear temporal relationship with the initiation and discontinuation of CNI. The other two patients showed signs of acute graft CNI toxicity on biopsy. Renal biopsy in one of them (patient D) was performed 3 years after KT due to a rise in creatinine levels >20%. It showed acute CNI-toxicity and moderate/severe tubular atrophy and interstitial fibrosis. A renal biopsy was performed in the other patient (patient E) 4 months after KT, which showed signs of acute tubular injury due to CNI-toxicity, as well as ACR Banff grade 2B in a patient which also had poor adherence to oral therapeutic regimens. Furthermore, two other patients were switched from CNI to belatacept due to cortical necrosis and TMA on biopsy respectively, both attributed to their treatment with CNI regimens. TMA in the renal transplant setting has a wide differential, including antibody-mediated rejection, or antiphospholipid syndrome, but could also be due to CNI toxicity. Immunofluorescence findings provided evidence against glomerular disease or immune complex disease. C4d staining was negative on biopsy which was inconsistent with antibody-mediated rejection and renal function improved with conversion to belatacept. No post-transplant lymphoproliferative disorders were noted in this cohort. Cardiovascular disease is reported as the major cause of death in SLE patients who have received a renal transplant.12 No deaths were reported in our cohort, and none of these patients had cardiovascular events or other malignancies. Two patients had recurrent urinary tract infections.
When considering worsening kidney allograft function in SLE, recurrent LN is an important consideration. Recurrent LN incidence varies greatly, reported in 2%–44% of KT recipients with SLE.13 14 But it rarely leads to kidney allograft loss.15 One patient had recurrent LN class V on her renal allograft biopsy (patient D). While her allograft failed 7 years after kidney transplantation, her last allograft biopsy demonstrated ischaemic nephropathy and severe arteriolar narrowing attributed to CNI toxicity that did not recover after discontinuation of TAC.
In a patient population known to have difficulty with maintaining complicated medication regimens, belatacept improves therapeutic adherence through reduction of pill burden. As evidenced here, one patient was converted to belatacept after she self-discontinued all immunosuppressants for 2 weeks (with subsequent biopsy demonstrating acute cellular rejection). Immunosuppressive regimens tailored to assist patient adherence will improve allograft and patient outcomes.
Study limitations include the retrospective design, the small number of patients treated with belatacept post-kidney transplant, as well as the availability of rheumatologic data (SLEDAI-2KG, complement and ds-DNA antibodies levels) in only three of the six patients.
Patients who are maintained on typical post-kidney transplant immunosuppression regimens also tend to have improvement in extrarenal manifestations of SLE. Our report suggests that belatacept in LN kidney transplant recipients may decrease extrarenal manifestations, attenuate CNI toxicity, ensure therapeutic adherence and stabilise allograft function, providing an alternative therapy to CNI-based renal transplant maintenance regimens. Future prospective studies to evaluate belatacept as a personalised treatment option for SLE kidney transplant recipients are warranted.
Acknowledgments
We would like to thank the Rheumatology Spanish Foundation (FER) and laboratories KERN PHARMA for its support with 'Becas FER-KERN PHARMA'. Our manuscript is based on work previously presented at the 2019 ACR/ARP Annual Meeting and published as the following conference abstract: 'Belatacept in Systemic Lupus Erythematosus (SLE) Kidney Transplant Patients'. Irene Carrión-Barberà, Melissa Fajardo, Demetra Tsapepas, Cathy Guo, Yevgeniya Gartshteyn, Hilda Fernandez and Anca Askanase. https://acrabstracts.org/abstract/belatacept-in-systemic-lupus-erythematosus-sle-kidney-transplant-patients/
References
Footnotes
HF and AA are joint senior authors.
Contributors We state that all the authors have made substantial contributions to the work presented, the final manuscript has been seen and approved by all the authors and they have paid the necessary attention to ensure the integrity of the work.
Funding The first author has received a grant "FER-KERN PHARMA" from the Rheumatology Spanish Foundation (FER) together with laboratories KERN PHARMA.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.