Article Text

Abstract
Objective The severity and disease course of cutaneous lupus erythematosus (CLE) are highly variable. Consequently, outcome measures for CLE clinical improvement are heterogeneous, complicating treatment decisions and therapeutic development. This study characterises CLE outcome measures and identifies the influence of clinical improvement thresholds on strengths of associations with patient demographic and clinical factors.
Methods In this pilot cohort study, multivariable models identified factors associated with CLE activity and skin damage improvement, defined as relative decreases in Cutaneous Lupus Activity and Severity Index (CLASI) activity (CLASI-A) and damage (CLASI-D) scores, over ranges of response thresholds.
Results 66 patients with 119 visit-pairs were included in the CLASI-A analysis. 74 patients with 177 visit-pairs were included in the CLASI-D analysis. Factors associated with CLE activity and damage improvement depended on the response threshold. Some associations were stronger at more stringent thresholds, including subacute CLE predominance with increased likelihood of CLASI-A improvement (R 2=0.73; 50% reduction: OR 1.724 (95% CI 0.537 to 5.536); 75%: 5.67 (95% CI 1.56 to 20.5)) and African-American race with decreased likelihood of CLASI-D improvement (R 2=0.80; 20%: 0.40 (95% CI 0.17 to 0.93); 40%: 0.25 (95% CI 0.08 to 0.82)). Other associations were stable across multiple thresholds, including older age of CLE development with increased likelihood of CLASI-A improvement (R 2=0.25; 50%: 1.05 (95% CI 1.01 to 1.09]; 75%: 1.05 (95% CI 1.00 to 1.10)) and higher initial disease activity with decreased likelihood of CLASI-D improvement (R 2=0.55; 20%: 0.91 (95% CI 0.84 to 0.98); 40%: 0.88 (95% CI 0.79 to 0.97)).
Conclusions Examining a range of CLASI threshold outcomes can comprehensively characterise changes in disease course in patients with CLE. Insufficiently stringent thresholds may fail to distinguish meaningful clinical change from natural fluctuation in disease activity.
- outcomes research
- disease activity
- treatment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Cutaneous lupus erythematosus (CLE) is an autoimmune skin disorder, which can occur in the context of SLE or independent of other organ involvement.1–3 Its clinical manifestations, severity and course are highly variable. This variability confounds the development of appropriate outcome measures that are reproducible, reflect the range of patient experience and reliably distinguish meaningful clinical improvement from fluctuation intrinsic to the natural history of the disease. As a result, studies have differed on defining clinical improvement in CLE. Outcomes have been measured using subjective assessments of improvement4 5 and different semiquantitative severity scoring systems.6–8 In the absence of clear outcome measures, assessing the effectiveness of different therapies and selecting the most appropriate treatments for individual patients has been challenging. While a variety of treatment options are available for CLE, treatment selection remains largely based on expert opinion rather than objective data.
The most commonly used scoring system for CLE is the Cutaneous Lupus Activity and Severity Index (CLASI), which independently grades manifestations of CLE disease activity (CLASI-A), such as erythema and scaling, and skin damage (CLASI-D), such as dyspigmentation and scarring.9–11 In validation studies, CLASI demonstrates high inter-rater and intrarater reliability and correlates well with subjective physician and patient global assessments of disease burden.9 12 However, there is little consensus on how changes in CLASI scores should be used to classify treatment response. Prior studies have found four-point or 20% decrease in CLASI-A score on a 70-point scale to be indicative of noticeable clinical improvement.13 Despite the possibility that such modest changes may be less meaningful for patients with more severe involvement or may fail to distinguish treatment response from expected clinical variability, similar thresholds have been used to classify activity improvement in interventional and observational studies.8 14 Other endpoints used include larger relative changes in CLASI-A scores (eg, 50% improvement in CLASI-A),15 16 analogous to the Psoriasis Area Severity Index (PASI) percentage change endpoints common in psoriasis studies (eg, PASI50).17 Even less information is available regarding CLASI-D endpoints, as skin damage phenomena are generally regarded as permanent. However, modest improvement in CLASI-D scores has been observed in prior studies.9 18 19Because individual studies tend to rely on single CLASI thresholds to define clinical improvement, the impact of the particular threshold selected remains unclear. Just as a diagnostic test’s cut-off value affects the test’s sensitivity and specificity, the outcome threshold used with a disease severity scoring system will affect the performance of that scoring system in both observational and interventional studies. This effect has been observed in a number of other fields, including using body mass index thresholds to define obesity,20 blood pressure thresholds to define hypertension21 and serological testing thresholds to define chronic atrophic gastritis.22 Thus, defining how different CLASI thresholds influence models of CLE improvement is critically important for CLE study design.
This study addresses that gap. Using longitudinal data from a cohort of patients enrolled in the University of Texas Southwestern (UTSW) Cutaneous Lupus Registry, we analysed CLE activity and damage improvement defined across ranges of relative change in CLASI-A and CLASI-D scores. By examining a range of outcome definitions rather than focusing on a single threshold to classify treatment response, we identified patient demographic and clinical factors associated with likelihood of CLE improvement across different thresholds. We found that the strengths of these associations depend strongly on the CLASI improvement thresholds used. In particular, we found that less stringent thresholds may not reliably distinguish meaningful clinical improvement from expected fluctuations in disease course, particularly for CLASI-A. We also identified association patterns that will aid providers in setting expectations when counselling patients. These findings have important implications for our understanding of CLE patient response to treatment and help guide the design of future clinical trials.
Methods
The UTSW Cutaneous Lupus Registry is a longitudinal cohort study of patients with CLE recruited from the outpatient dermatology clinics of UTSW and Parkland Health and Hospital System. This study was approved by the UTSW Institutional Review Board. Patients or the public were not involved in the design, or conduct, or reporting, or dissemination of this research. Data collected include patient demographics, disease history, medication history, laboratory data and CLE disease severity using CLASI scores. For primary outcome measures of skin disease activity and damage improvement, we designated response thresholds based on percent change in CLASI-A and CLASI-D scores between two consecutive study visits, defined as a visit-pair. Specifically,


This approach was intended to target periods of approximately 6–12 months, a typical time course for evaluating treatment response or failure in practice and a common duration for clinical trials.7 23–25 Two response thresholds were initially selected to screen factors for each analysis. These included standard thresholds, representing relative decreases in CLASI-A (≥50%) or CLASI-D (≥20%) within the range of outcomes considered in prior studies,8 14–16 19 and stringent thresholds, representing larger relative decreases in CLASI-A (≥75%) or CLASI-D (≥40%) score.
Patients with at least two study visits between July 2009 and September 2016 were available for inclusion in this study. Patients with drug-induced CLE were excluded. We designated two study subsets from this cohort. Patients with CLASI-A ≥5 or CLASI-D ≥5 at the initial visit of a visit-pair were selected for analysis of CLE disease activity or damage improvement, respectively, thus excluding patients with disease activity or skin damage levels too low to detect noticeable improvement.
Statistical analysis was conducted using R software (version 3.4.4; https://www.R-project.org/) with the geepack package (version 1.2.1).26 Single-variable and multivariable logistic regression models were fit using generalised estimating equations with independence working correlation structures and robust variance estimators to account for potential lack of independence among visit-pairs from the same patient.27 As a sensitivity analysis, final multivariable models were also fit using exchangeable and first-order autoregressive correlation structures, which did not substantially impact the results. Single-variable models were used to screen potential independent variables selected based on literature review and clinical experience (online supplementary table 1). Factors with p<0.10 at either of the screening thresholds were included in the multivariable models, which were then fit across the response threshold ranges. Variation in parameter coefficients was characterised using Pearson product moment correlation, with the squared coefficient (R 2) representing the fraction of variation in the multivariable model parameter coefficient explained by linear change in the response threshold. P<0.05 was considered statistically significant.
Supplemental material
Results
Study population
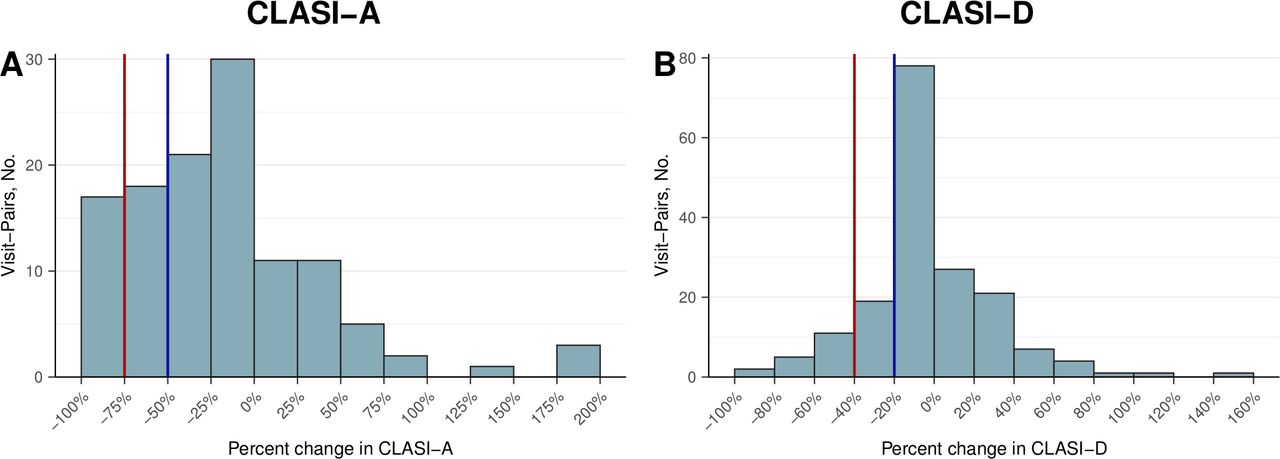
Data from 66 patients with 119 consecutive visit-pairs were included in the analysis of CLASI-A improvement, and data from 74 patients with 177 consecutive visit-pairs were included in the analysis of CLASI-D improvement (table 1). The two analysis groups partially overlapped; 52 patients with a total of 89 visit-pairs were included in both analyses. Both groups were predominantly women with median ages of 46 years for the CLASI-A analysis and 45 years for the CLASI-D analysis. More than half of the patients in each group met diagnostic criteria for SLE. However, compared with the CLASI-A analysis, the CLASI-D analysis included a higher proportion of patients who were African-American (62% vs 49%) and had predominantly chronic CLE (CCLE) lesions (100% vs 85%). The range in disease activity change from visit to visit was quite broad; 35 (29%) visit-pairs had a relative CLASI-A decrease of ≥50%, and 17 (14%) had a relative CLASI-A decrease of ≥75% (figure 1). In contrast, damage changes were smaller; 37 (21%) visit-pairs had a relative CLASI-D decrease of ≥20%, and 18 (10%) had a relative CLASI-D decrease of ≥40% (figure 1). Several factors demonstrated potential positive or negative associations with CLASI-A and CLASI-D improvement based on cross-tabulations and single-variable models (online supplementary tables 1 and 2 and figure 1). Factors with p<0.10 in single-variable screening models, including smoking, CLE subtype, and age of CLE development for CLASI-A improvement and initial CLASI-A score, African-American race, and positive ANA for CLASI-D improvement, were selected for inclusion in the multivariable models.
Supplemental material
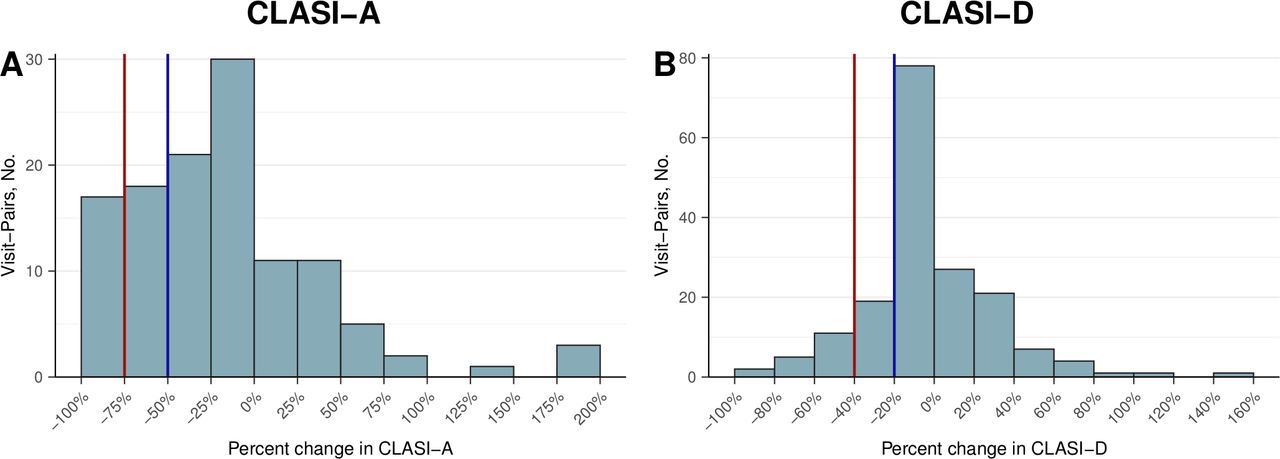
Percent change in Cutaneous Lupus Activity and Severity Index (CLASI) scores. Distribution of per cent change in CLASI activity (CLASI-A, top) and CLASI damage (CLASI-D, bottom) scores within visit-pairs. Blue line delineates ≥50% decrease in CLASI-A and ≥20% decrease in CLASI-D. Red line delineates ≥75% decrease in CLASI-A and ≥40% decrease in CLASI-D.
Demographic and baseline characteristics
Analysis across response thresholds
To more completely characterise the impact of outcome measure selection on factors associated with activity and damage improvement, we compared multivariable logistic regression models across ranges of CLASI-A and CLASI-D response thresholds. The impact of these thresholds was substantial, as demonstrated by differences between models at the predefined screening thresholds of ≥50% CLASI-A improvement, ≥75% CLASI-A improvement, ≥20% CLASI-D improvement and ≥40% CLASI-D improvement (table 2). In particular, subacute cutaneous lupus erythematosus (SCLE) predominance was associated with increased likelihood of CLASI-A improvement only at the 75% threshold (OR 5.67 (95% CI 1.56 to 20.5), p=0.008). Additionally, African-American race was modestly associated with decreased likelihood of CLASI-D improvement at the 20% threshold (OR 0.40 (95% CI 0.17 to 0.93), p=0.03) but more significantly at the 40% threshold (OR 0.25 (95% CI 0.08 to 0.82), p=0.02). In contrast, age of CLE development was similarly associated with a higher likelihood of CLASI-A improvement at the 50% threshold (OR per 10 year increase: 1.612 (95% CI 1.127 to 2.304), p=0.009) and at the 75% threshold (OR 1.616 (95% CI 1.015 to 2.574), p=0.04). Initial CLASI-A score was similarly associated with lower likelihood of CLASI-D improvement at the 20% threshold (OR per 5-point increase: 0.625 (95% CI 0.427 to 0.915), p=0.02) and at the 40% threshold (OR 0.514 (95% C I0.312 to 0.846), p=0.009).
Multivariable models
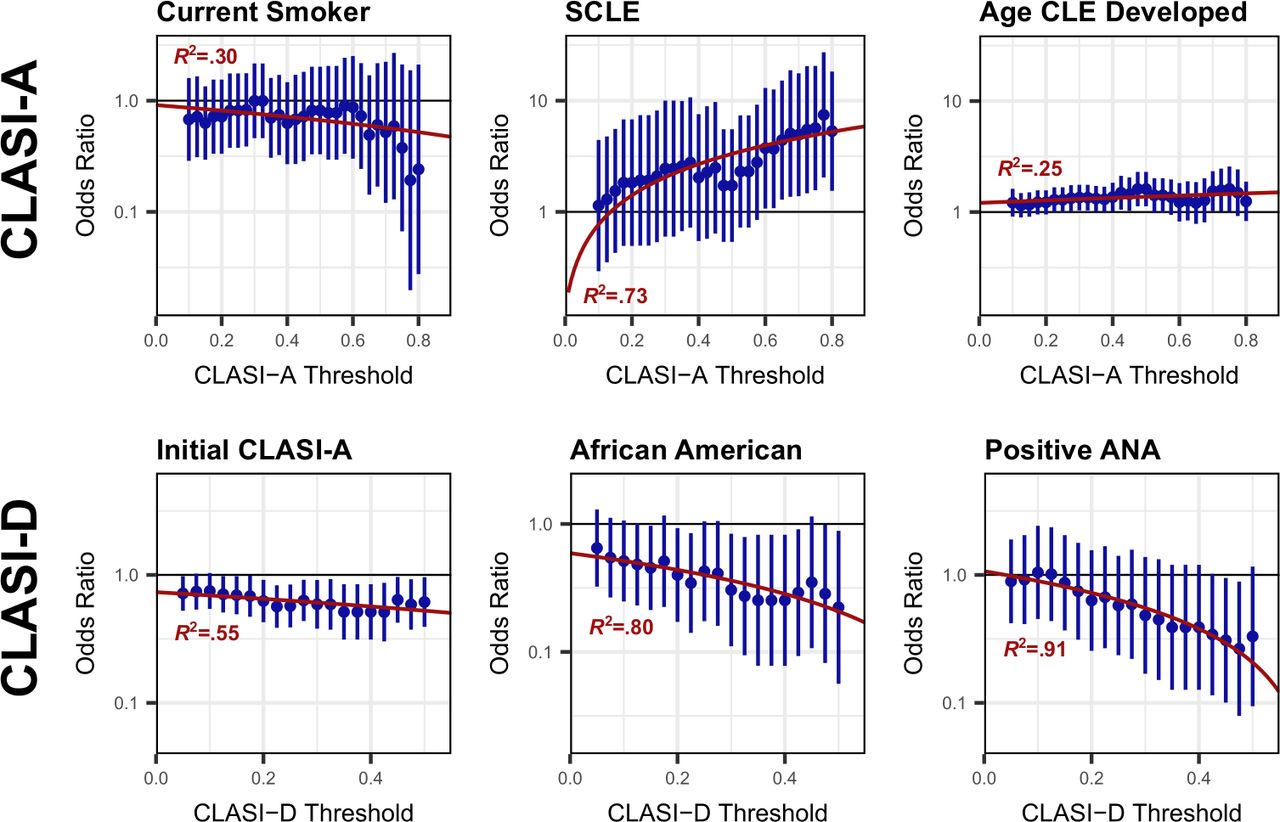
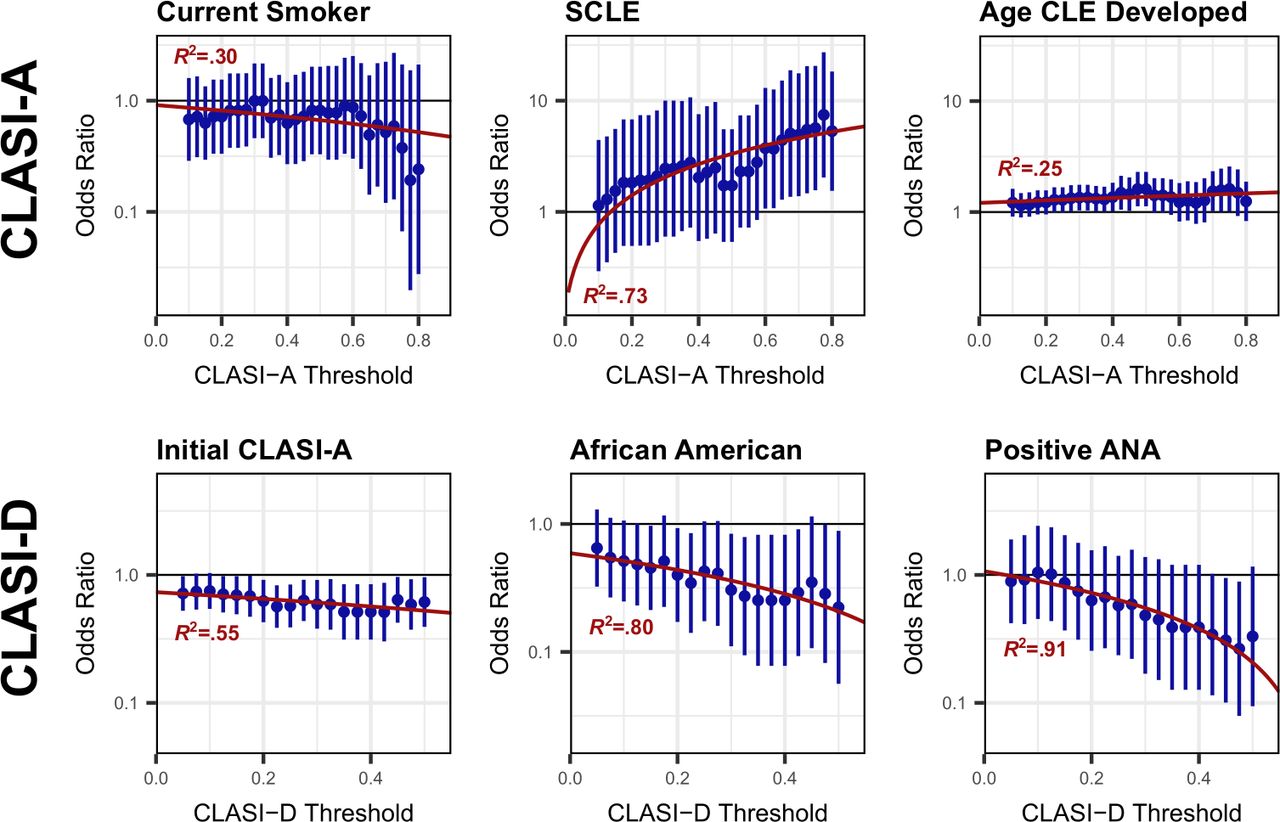
Model fits across the full CLASI-A and CLASI-D response threshold ranges (figure 2 and online supplementary table 3) further illustrate the considerable variation in strength of association between different independent variables and the likelihood of CLE activity or damage improvement, depending on the particular CLASI-A or CLASI-D threshold used. In figure 2, ORs for each parameter in the multivariable models are individually compared across thresholds. For some factors, the strength of association with likelihood of activity or damage improvement increased or decreased with greater relative changes in CLASI-A and CLASI-D. This was the case for SCLE predominance (R 2=0.73) in the CLASI-A analysis, where the strength of association increased with greater improvement in CLASI-A scores. In African-American patients (R 2=0.80) and those with history of positive ANA (R 2=0.91) in the CLASI-D analysis, the strength of association with damage improvement decreased with greater relative changes in CLASI-D, although the latter association was quite weak. In contrast, other factors showed more stable associations throughout the spectrum of relative changes of CLASI-A and CLASI-D scores. These included current smoking history (R 2=0.30) and age CLE developed (R 2=0.25) in the CLASI-A analysis and initial disease activity (R 2=0.55) in the CLASI-D analysis.
{kind=link}
{kind=link}
Associations between patient factors and cutaneous lupus erythematosus activity and damage improvement depend on the response threshold. Each panel compares ORs for a single independent variable in multivariable logistic regression models across different thresholds for activity or damage improvement, defined as per cent change in Cutaneous Lupus Activity and Severity Index (CLASI) Activity (CLASI-A, top row) or Damage (CLASI-D, bottom row). ORs (points) with 95% CI (vertical lines) are plotted on the y-axis, with the position on the x-axis corresponding to the CLASI-A or CLASI-D per cent change threshold. Red curves indicate linear OR trends. CLE, chronic cutaneous lupus erythematosus; SCLE, subacute cutaneous lupus erythematosus.
Exploratory secondary analyses
In order to fully explore potential associations in the dataset, we fit expanded multivariable models for CLASI-A and CLASI-D improvement including factors with p<0.20 in the single-variable models (online supplementary table 4). The expanded models identified several potential associations of interest, including use of immunosuppressant medications at baseline and decreased likelihood of CLASI-A improvement at the 50% (OR 0.246 (95% CI 0.083 to 0.732)) and 75% thresholds (OR 0.112 (95% CI 0.022 to 0.571)), and longer follow-up interval with increased likelihood of ≥40% CLASI-D improvement (OR per month: 1.042 (95% CI 1.007 to 1.078)). However, given the large number of parameters included in these models relative to the number of events, more data will be needed to confirm these associations.28 29
As SCLE predominance had the strongest association with ≥75% CLASI-A improvement in the multivariable model (table 2), and the pathophysiology of CLE subtypes may differ, we separated patients in the CLASI-A analysis into subgroups based on those with predominantly SCLE or predominantly CCLE lesions (online supplementary table 5). Compared with patients with CCLE, patients with SCLE developed CLE at an older age, another factor associated with increased likelihood of CLASI-A improvement in the multivariable models. However, older age of CLE development remained associated with CLASI-A improvement in a single-variable model of the CCLE subgroup at the 50% (OR per 10 year increase: 1.57 (95% CI 1.07 to 2.30), p=0.02) and 75% thresholds (1.58 (95% CI 0.87 to 2.89), p=0.13), although the latter did not reach statistical significance due to small sample size. Since stratifying by CLE subtype does not completely explain the association between age of CLE development and CLASI-A improvement, this supports inclusion of both CLE subtypes in the multivariable models.
Discussion
The relationships between patient factors and CLE activity and skin damage improvement depend on the CLASI-A and CLASI-D reduction thresholds used to classify clinical improvement. For example, SCLE predominance for activity improvement and African-American race for damage improvement had little association at lower changes in CLASI-A and CLASI-D but developed much stronger associations at higher changes, particularly ≥75% compared with ≥50% CLASI-A improvement and ≥40% compared with ≥20% CLASI-D improvement. These findings highlight the importance of evaluating a range of CLASI improvement threshold outcome measures to obtain a comprehensive picture of disease prognosis. There may be many difficult-to-identify factors influencing small to moderate changes in CLASI score, including the natural waxing and waning course of CLE as well as CLASI measurement uncertainty. Insufficiently stringent CLASI thresholds may thus fail to distinguish meaningful clinical benefit from other causes of fluctuation in disease severity. Future studies of potential CLE treatments can evaluate multiple thresholds that include large improvements in disease activity (eg, ≥75% CLASI-A improvement) rather than focusing solely on one threshold (eg, ≥50% CLASI-A improvement) and be powered accordingly.
Varying effects across threshold values can also reveal important properties of the underlying associations and may suggest separate processes influencing moderate compared with significant CLE improvement. For example, SCLE predominance was associated with CLASI-A improvement only at stringent thresholds, suggesting that while patients with SCLE or CCLE lesions may experience moderate activity improvement, dramatic short-term improvement is more common for SCLE than for CCLE. One possibility is that this divergence may reflect the relatively sparse superficial perivascular lymphocytic infiltrate in SCLE, compared with the denser perifollicular and perivascular inflammatory infiltrate in CCLE, particularly in discoid lesions.30 This information can be useful to providers, who can counsel patients with SCLE that they are more likely to experience significant improvement in their lesions with appropriate treatment. Additionally, African-American race was more strongly associated with decreased likelihood of ≥40% CLASI-D improvement compared with ≥20% CLASI-D improvement. This finding may reflect the potentially greater visibility of damage phenomena, particularly dyspigmentation, in darker skin types. This finding will also help providers set appropriate expectations for these patients regarding their disease damage course. Consistent with this result, other studies have demonstrated higher levels of CLE damage in African-American patients, although a higher prevalence of CCLE in African-Americans could confound this relationship.31 32
Other predictor variables showed varying patterns across different CLASI-A or CLASI-D thresholds. Age of CLE development was modestly associated with increased likelihood of activity improvement at both the ≥50% and ≥75% CLASI-A thresholds, although increasing uncertainty at more stringent thresholds complicates the interpretation. This result suggests that patients who develop CLE early in life may be less responsive to treatment than those with later-onset disease. In a similar pattern, other studies have found that early-onset SLE patients present with more activity than those with late-onset disease due to higher frequency of major organ involvement33 34 and may also be less responsive to treatment.35 However, while younger age of CLE development was associated with decreased likelihood of CLE activity improvement between visits in our analyses, it was not associated with higher CLASI-A scores (data not shown). Additionally, initial CLE activity was similarly associated with lower likelihood of CLE damage improvement at both the ≥20% and ≥40% CLASI-D thresholds. This pattern fits with our understanding that CLE disease activity can later develop into manifestations of skin damage. Thus, patients with higher initial CLASI-A scores are less likely to experience even modest improvement in CLASI-D scores between visits.
While the varying effect sizes across CLASI improvement thresholds found in this study demonstrate the importance of examining a range of thresholds, they also present two potential pitfalls. First, varying effect sizes across thresholds should not be exploited to select one threshold, which maximises the effect of a particular parameter of interest. Such optimisation methods will significantly bias results of the analysis to inflate the effect size of the selected parameter. Additionally, when relying on a null hypothesis significance testing framework, care should be taken to manage potential type I error rate inflation from multiple comparisons. Appropriate strategies could include prespecification of a small number of primary outcome thresholds, as we have done in this study, or statistical methods for controlling global level type I error rates, such as the Bonferroni correction.36
Limitations of this study include small sample size and selection bias due to the study occurring at a single tertiary centre. In addition, while many study participants started or stopped medications, these changes were distributed over a wide range of treatments. As a result, individual therapies could not be included in the analysis, and treatment changes were instead grouped by medication class (table 1). However, we did not find that adding or stopping classes of medications were significant factors in changes in CLASI activity or damage. Our study was also limited to analysing changes between visits, thus providing a relatively short-term perspective. One recent study has described longer term trends in patients with CLE but did not examine relative changes in CLASI-A or CLASI-D scores.19 Finally, this observational study cannot definitively determine the underlying causes of the identified associations and their variation with CLASI improvement thresholds, and future studies will be needed to better define these mechanisms.
The factors associated with CLE activity and damage improvement identified in this study can inform patient counselling and treatment planning. For example, our data support the idea that patients with SCLE can reasonably expect significant improvements in their skin disease activity. Additionally, the variability of these associations depending on the CLASI reduction thresholds used to define clinical response highlights the need to examine a range of response thresholds in future studies. Individual threshold-based outcome measures may miss important effects or fail to adequately capture the clinical context. In particular, smaller changes in CLASI may occur in patients, but they may be more difficult to attribute to a particular predictor or intervention. Based on these results, larger multicentre studies currently being pursued can include evidence-based outcome measures that adequately assess therapeutic efficacy for CLE.
Acknowledgments
The authors would like to thank Dr Yulun Liu for reviewing the biostatistical analyses of our manuscript, and Drs Elaine Kunzler, Rebecca Vasquez, Andrew Kim, Daniel Grabell, Noelle Teske, Tina Vinoya, Jack O’Brien, Danielle Lin, Jenny Raman and Justin Raman for recruiting patients, and the participants of the University of Texas Southwestern (UTSW) CLE Registry for their contributions to lupus research.
References
Footnotes
Contributors BAN and BFC designed the study and drafted the manuscript. All authors were responsible for acquisition, analysis and interpretation of the data. BAN performed the statistical analysis. BFC obtained funding and supervised the study.
Funding This study was supported in part by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under Award Number K23AR061441.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the University of Texas Southwestern Medical Center at Dallas and its affiliated academic and health care centers or the National Institutes of Health.
Competing interests BFC is an investigator for Daavlin Corporated, Biogen Incoporated and Pfizer Incorporated. He is a consultant for Viela Bio.
Patient consent for publication Not required.
Ethics approval This study was approved by the UTSW Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.