Article Text

Abstract
Objective Fas/Fas ligand (FasL) and B cell-activating factor (BAFF) signalling have pivotal roles in SLE pathogenesis. We investigated the clinical associations of serum concentrations of soluble Fas (sFas) and soluble FasL (sFasL) in SLE and their relationship with BAFF.
Methods Serum sFas and sFasL were quantified by multiplex assay, and BAFF by ELISA, in 118 patients with SLE and 17 healthy controls (HC). SLE disease activity and organ damage were assessed using the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) and the Systemic Lupus International Collaborating Clinics Damage Index.
Results sFas, sFasL and BAFF were detectable in all samples. Serum sFas and sFasL were significantly higher in SLE compared with HC. In univariable regression analyses, patients with active renal disease and those with flare had significantly higher levels of sFas compared with those without. High serum BAFF in patients with SLE was associated with increased sFas but not sFasL. The association between sFas and renal disease remained significant after adjusting for BAFF, but the association with flare attenuated. High sFas levels were associated with increased time-adjusted mean SLEDAI-2K, even after adjusting for BAFF, and with higher odds of flare over time. In contrast, high sFasL was associated with reduced organ damage over time. Serum sFasL/sFas ratio was negatively associated with active overall disease, flare and organ damage.
Conclusions Serum sFas is associated with active renal SLE, and active disease and flare over time, while sFasL/sFas ratio is negatively associated with disease activity and organ damage accrual. Treatments correcting abnormal levels of sFas/FasL may be worthy of evaluation in SLE.
- autoimmunity
- cytokines
- systemic lupus erythematosus
- lupus nephritis
- autoimmune diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
SLE is an idiopathic heterogeneous chronic systemic autoimmune disease.1 Among many implicated cytokine systems, evidence suggests that the tumour necrosis factor (TNF) superfamily ligand Fas ligand (FasL), which signals through Fas, may play a role in SLE pathogenesis.2 Signalling by FasL through Fas leads to apoptosis,3 and impaired activation-induced cell death induced by mutations in mouse genes encoding for Fas (lpr) and FasL (gld) leads to spontaneous mouse models reminiscent of human SLE.4–6 The soluble forms of Fas (sFas) and FasL (sFasL) both act mainly as decoys for the Fas-mediated apoptosis pathway,7–11 potentially leading to increased survival of Fas-bearing target cells. However, sFasL mediates proinflammatory effects through Fas,12–14 while a proapoptotic function of oligomeric, but not monomeric, sFas has been described,15 indicating potentially divergent functions of sFasL and sFas that are especially relevant when sFas is abundant, such as in autoimmune disease.15 16
Compared with healthy controls (HC), serum sFas concentrations are reported in most studies to be elevated in patients with SLE.10 17–25 However, reported findings are inconsistent in regard to the relationship between serum sFas and disease activity, in that a positive relationship is shown in some studies,17 18 22 25 26 but not in others.16 19 24 Only a very few studies have investigated serum sFas as a biomarker for specific organ activity, particularly associated with renal, neurological and mucocutaneous SLE.16 18 20 27 28 Fewer studies have focused on sFasL in SLE, although it has been reported to be elevated compared with HC in most studies.21 23 26 29 A positive relationship between sFasL and SLE disease activity has been reported in one study,26 but not in another.30
In light of these discrepancies, measuring the ratio between sFas and sFasL may be of interest, since both proteins belong to the same immunological pathway and are able to modulate the Fas/FasL system.21 The use of this ratio may better reflect the Fas/FasL system biological activity as a whole, where sFas and sFasL may have divergent biological functions.21 31 While the ratio has been investigated in other conditions,32–35 only one prior study in a small cohort of 15 patients assessed this ratio in relation to SLE disease activity.21
B cell-activating factor from the TNF family (BAFF) is a key pathogenic cytokine in SLE.36 The Fas/FasL disrupted MRL-lpr/lpr lupus-prone mouse model is characterised by high serum BAFF concentrations,37 38 and our group previously described an interaction between the BAFF system and Fas/FasL system-mediated marginal zone B cell apoptosis in mice.39 Since BAFF potentially plays a role in the regulation of the Fas/FasL apoptotic pathway,39 measuring the key components of both BAFF and Fas/FasL systems is an interest in human SLE. To date, only one study has measured both BAFF and components of the Fas/FasL system in their soluble forms, within a larger pool of 52 soluble factors.40
Here, we aimed to investigate the clinical associations of serum sFas and sFasL as well as the ratio of these molecules in an SLE cohort larger and better characterised than any previously described, and investigate whether associations with SLE are independent of serum BAFF concentrations. We also assessed the associations of baseline measurements of these factors with clinical progression over time.
Materials and methods
Participants and clinical assessments
Adult patients fulfilling the 1997 American College of Rheumatology revised criteria for SLE classification were enrolled at the Monash Lupus Clinic (Clayton, Victoria, Australia) between December 2009 and July 2014, as previously described.41 Demographic and clinical data, including disease duration, activity and damage, routine laboratory markers, and treatment, were recorded at baseline and routine visits. Overall disease activity was assessed using a hybrid Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K).42 Disease activity at a given visit/sample date was classified as inactive if SLEDAI-2K was ≤4, using the SLEDAI-2K threshold used in the definition of the lupus low disease activity state43; an SLEDAI-2K >4 was thus classified as active. To assess individual organ-specific disease activity, components of the SLEDAI-2K scoring system were grouped into nine organ domains. Organ-specific disease activity was defined as activity in at least one component of the SLEDAI-2K that pertains to an organ domain.44 Average disease activity over time was assessed using the time-adjusted mean SLEDAI-2K (AMS),45 46 and active disease over time defined as AMS >4.47 Flare was assessed using the Safety of Estrogens in Lupus Erythematosus National Assessment Flare Index.48 Patients were classified as having irreversible organ damage using the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index, as previously described.49 Cut-off values for routine laboratory markers analysis were as follows: high C reactive protein (CRP) (>3 mg/L), high erythrocyte sedimentation rate (ESR) (≥25 mm/hour), proteinuria (urine protein to creatinine ratio (UPCR) >0.05 g/mmol), low C3 (<0.79 g/L) and low C4 (<0.16 g/L). All patients received standard-of-care therapy. Between June and August 2014, healthy individuals were enrolled as an HC group. All individuals gave written informed consent.
Serum cytokines and soluble receptor quantification
Whole blood was collected by venepuncture in association with routine clinical visits. Serum was isolated using serum-separating collection tube, as previously described,50 and stored at −80°C, until further use. Serum sFas and sFasL concentrations were quantified using a commercial Luminex screening assay (polystyrene beads; Cat #LXSAH, R&D Systems, Minneapolis, Minneapolis, USA), using a Bio-Rad Bio-Plex 200 system, following the manufacturer’s protocol. Serum BAFF concentrations were quantified using a commercial ELISA kit (Quantikine, Cat #SBLYS0B, R&D Systems), following the manufacturer’s protocol. Analysis of serum BAFF in a smaller cohort of patients (n=87) that are included in this larger sample has been reported separately.51
Statistical analysis
Statistical analysis was performed using Stata V.14.2 (StataCorp, College Station, Texas, USA) software. Continuous data were described as median (IQR) or mean (SD) according to data distribution. Categorical data were summarised as number (frequency). Correlations between variables were examined using Spearman’s rank or Pearson’s correlation test, depending on data distribution. We compared some demographics between patients with SLE and HC using t-test to compare means, and Pearson’s χ2 test or Fisher’s exact test to compare proportions. Linear regression was used to examine associations of serum sFas and sFasL concentrations, and their ratio, with clinical outcomes in cross-sectional analysis. Serum BAFF, sFas and sFasL concentrations were log10-transformed before including in the linear regression models. In the occurrence of non-normal distribution after data transformation, a bootstrap method with 50-sample derivation was incorporated to derive robust CI. Results were shown as geometric mean (GM) (antilogs of the means derived from linear regressions) and the ratios of GM (antilogs of regression coefficient) with corresponding 95% CI. Logistic regression analysis was used to examine the associations of baseline serum cytokines and soluble receptor concentrations with longitudinal clinical outcomes. Based on the medians, serum BAFF, Fas and sFasL concentrations were grouped as low (≤median) and high (>median) subsets to perform logistic regression analysis. Variables which demonstrated univariable associations with p<0.1 with both independent (exposure) and dependent (outcome) factors were included in multivariable linear and logistic regression models as potential confounders. P<0.05 was considered statistically significant.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Participant characteristics
One hundred and eighteen patients with SLE were included in this study. Patients’ characteristics are summarised in table 1. Briefly, the mean (SD) age was 45.4 (14.2) years and the median (IQR) disease duration was 7.2 (3.9–14.7) years. Of the patients, 85% were female, 48% were of Asian ethnicity, 33% had active disease and 57% were receiving glucocorticoids. Follow-up clinical data were available for a median (IQR) of 2.1 (1.8–2.6) years after serum sampling. The HC cohort comprised 17 individuals, among whom 88% were female and nearly 30% were of Asian ethnicity. The median (IQR) age was 41 (28–44) years. The HC cohort was gender-matched and ethnicity-matched to the SLE cohort, but was significantly younger (mean (SD) 37.4 (10.2) vs 45.4 (14.2) years; p=0.03). Hence, age was included as a potential confounder in the multivariable regression analysis models when comparing SLE with HC cohorts.
Demographic, clinical and biological characteristics of the SLE cohort
Cytokine and soluble receptor concentrations in SLE and HC
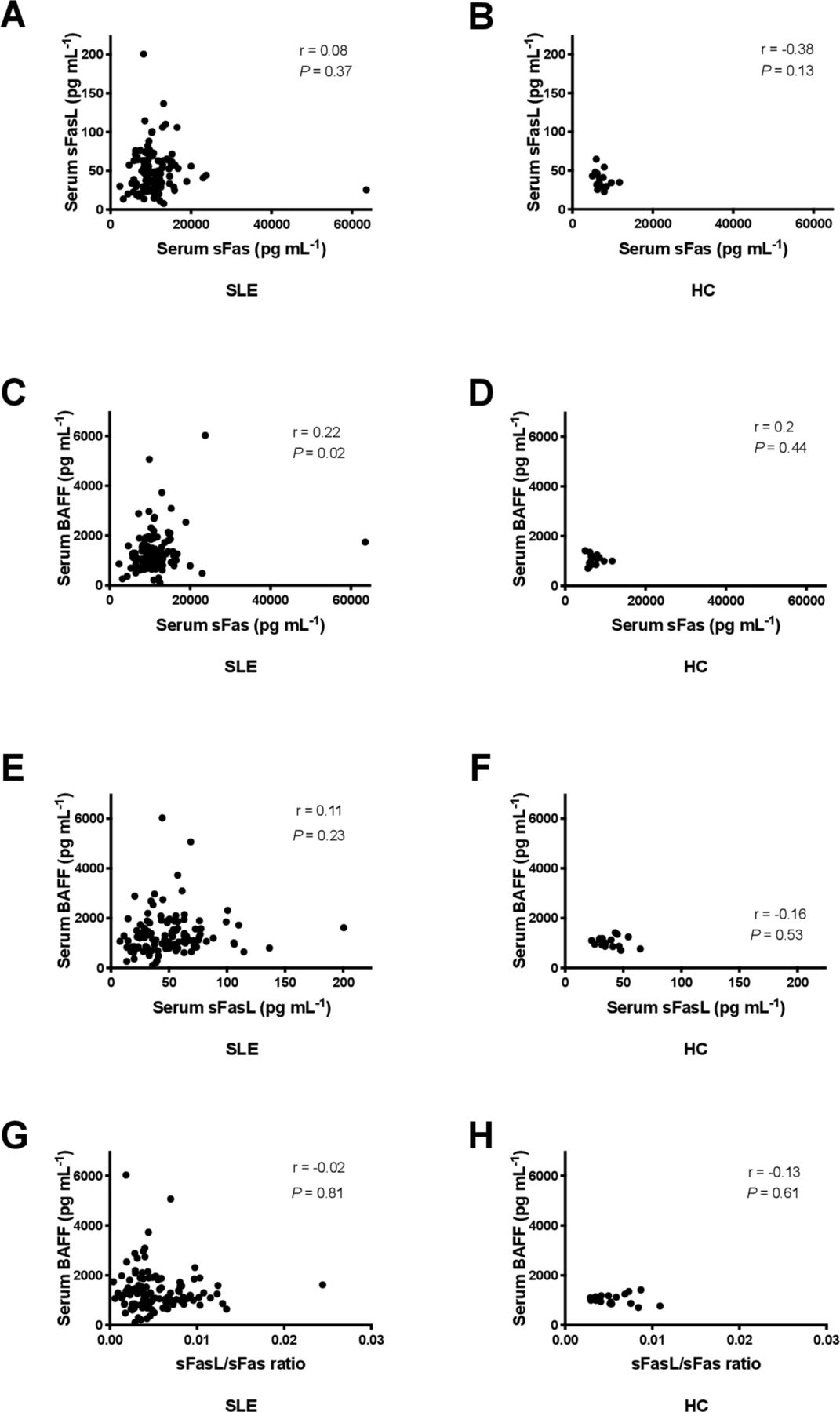
sFas and sFasL were detectable in all serum SLE and HC samples. Serum sFas concentration was significantly increased in SLE compared with HC (ratio of GM 1.44; 95% CI 1.19 to 1.74; p<0.01), and after adjusting for age (ratio of GM 1.4; 95% CI 1.15 to 1.7; p<0.01) (figure 1A). Serum sFasL concentrations were also significantly increased in SLE when compared with HC (ratio of GM 1.18; 95% CI 1.01 to 1.37; p=0.04), confirmed after adjusting for age (ratio of GM 1.2; 95% CI 1.01 to 1.42; p=0.04) (figure 1B). Serum sFasL/sFas ratio was significantly decreased in SLE (ratio of GM 0.82; 95% CI 0.68 to 0.99; p=0.04); however, this association was not confirmed after adjusting for age (ratio of GM 0.86; 95% CI 0.64 to 1.15; p=0.31) (figure 1C). Serum sFas and sFasL concentrations were not correlated with each other in either the SLE or HC cohort (figure 2A,B).
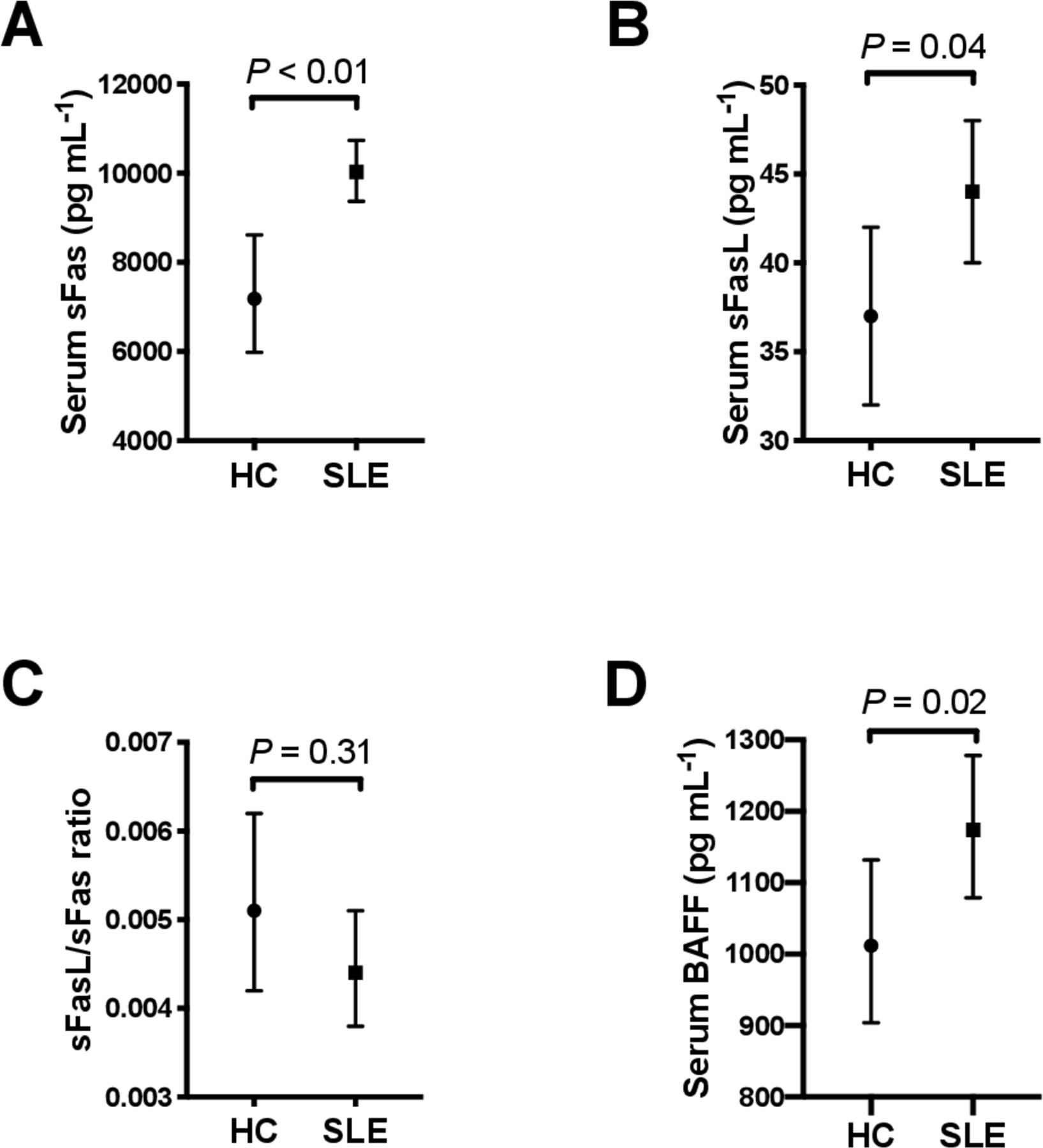
Serum sFas, sFasL, sFasL/sFas ratio and BAFF in SLE. Age-adjusted geometric mean derived using multivariable linear regression analysis of serum sFas concentrations (A), sFasL concentrations (B), sFasL/sFas ratio (C), and BAFF concentrations (D) in HC (n=17) and in patients with SLE (n=118). BAFF, B cell-activating factor from the tumour necrosis factor family; HC, healthy control; sFas, soluble Fas; sFasL, soluble Fas ligand; SLE, systemic lupus erythematosus.
{kind=link}
{kind=link}
Correlation between serum sFas, sFasL, sFasL/sFas ratio, and BAFF concentrations in SLE and HC. (A–B) Correlation between serum sFas and sFasL concentrations in (A) SLE (n=118) and (B) HC (n=17). (C–D) Correlation between serum sFas and BAFF concentrations in (C) SLE (n=118) and (D) HC (n=17). (E–F) Correlation between serum sFasL and BAFF concentrations in (E) SLE (n=118) and (F) HC (n=17). (G–H) Correlation between serum sFasL/sFas ratio and BAFF concentrations in (G) SLE (n=118) and (H) HC (n=17). In A–H, correlations were examined using Spearman’s correlation rank test. BAFF, B cell-activating factor from the tumour necrosis factor family; HC, healthy control; sFas, soluble Fas; sFasL, soluble Fas ligand; SLE, systemic lupus erythematosus.
Serum BAFF was detectable in all SLE and HC serum samples. Serum BAFF was significantly increased in SLE compared with HC (ratio of GM 1.15; 95% CI 1.02 to 1.3; p=0.03), and after adjusting for age (ratio of GM 1.16; 95% CI 1.02 to 1.3; p=0.02) (figure 1D). Serum sFas was weakly positively correlated with BAFF concentration in SLE (r=0.22; p=0.02), but not in HC (figure 2C,D). Linear regression analysis confirmed a positive association between sFas and BAFF (ratio of GM 1.2; 95% CI 1.04 to 1.38; p=0.01). No significant correlation was observed between serum concentrations of BAFF and sFasL or sFasL/sFas ratio in SLE or HC samples (figure 2E–H).
Clinical associations: cross-sectional analysis at time of sampling
We investigated whether serum concentrations were associated with clinical parameters at the time of sampling, using linear regression, adjusting for potential confounders including serum BAFF. Serum sFas was significantly higher in patients with active renal disease, defined as renal SLEDAI-2K >0 or by the presence of proteinuria (table 2). Similarly, serum sFas was significantly higher in patients with flare (table 2). The association between serum sFas and active renal SLE was confirmed after adjusting for serum BAFF (ratio of GM 1.35; 95% CI 1.13 to 1.62; p<0.01), but the association with flare attenuated (ratio of GM 1.13; 95% CI 0.96 to 1.33; p=0.15). We did not observe any association between serum sFas and overall disease activity or other organ-specific SLE disease activity, organ damage or laboratory markers (table 2).
Univariable associations of serum sFas, sFasL, and sFasL/sFas ratio with SLE clinical parameters at baseline
In contrast, serum sFasL levels were reduced in patients with flare (table 2). This association was, however, attenuated after adjusting for use of immunosuppressants (ratio of GM 0.86; 95% CI 0.68 to 1.09; p=0.21). Serum sFasL was also significantly decreased in patients with high ESR and in those receiving glucocorticoids (table 2). No statistically significant association emerged of sFasL with disease activity, organ damage or other laboratory markers (table 2).
The sFasL/sFas ratio was negatively associated with active overall disease activity, and with renal and mucocutaneous disease activity, in univariable analysis (table 2). The association between sFasL/sFas ratio and overall disease activity was confirmed after adjusting for use of immunosuppressants (ratio of GM 0.79; 95% CI 0.65 to 0.96; p=0.02), but the association between sFasL/sFas ratio and active renal and mucocutaneous disease was attenuated (renal: adjusted for use of immunosuppressants, ratio of GM 0.79, 95% CI 0.58 to 1.07, p=0.13; mucocutaneous: adjusted for use of glucocorticoids and immunosuppressants: ratio of GM 0.89, 95% CI 0.7 to 1.13, p=0.35). The sFasL/sFas ratio was also negatively associated with flare, confirmed after adjusting for use of immunosuppressants (ratio of GM 0.73; 95% CI 0.54 to 1; p=0.05), and with high ESR (table 2). We did not observe any significant association between sFasL/sFas ratio and the presence of organ damage or other laboratory markers (table 2).
Clinical associations: longitudinal analysis
We next examined whether baseline serum concentrations were associated with clinical outcomes over time. Patients with high baseline serum sFas were more than three times more likely to have active disease over time (AMS >4) (table 3), confirmed after adjusting for BAFF, patients’ age and use of glucocorticoids and immunosuppressants (OR 3.43; 95% CI 1.32 to 8.9; p=0.01). Patients with high baseline serum sFas were also more than four times likely to have flare of disease over time (table 3), confirmed after adjusting for use of glucocorticoids and immunosuppressants (OR 3.52; 95% CI 1.4 to 8.86; p<0.01). No significant association was observed between serum sFas and damage accrual (table 3).
Univariable associations of baseline serum sFas, sFasL, and sFasL/sFas ratio with SLE clinical outcomes over time
In contrast, patients with high baseline sFasL had a 60% reduction in flares over time and 70% reduction in risk of organ damage at the last visit (table 3). The association between sFasL and organ damage at the last visit remained significant after adjusting for ethnicity (OR 0.35; 95% CI 0.15 to 0.82; p=0.02), but the association with flare over time attenuated after adjusting for use of glucocorticoids and immunosuppressants (OR 0.57; 95% CI 0.23 to 1.37; p=0.21). Increased baseline sFasL was also negatively associated with damage accrual, with borderline significance (table 3). No significant association was observed between serum sFasL and AMS (table 3).
Examining serum sFasL/sFas ratio, univariable analysis revealed strong negative associations with flares over time and damage accrual (table 3). The association between sFasL/sFas ratio and organ damage at the last visit remained significant after adjusting for ethnicity (OR 0.41; 95% CI 0.17 to 0.94; p=0.04). The association between sFasL/sFas ratio and damage accrual remained significant after adjusting for use of glucocorticoids, a major driver of damage accrual in SLE (OR 0.35; 95% CI 0.13 to 0.89; p=0.03). However, the association with flare over time attenuated after adjusting for use of glucocorticoids and immunosuppressants (OR 0.58; 95% CI 0.24 to 1.4; p=0.23). No significant association was observed between sFasL/sFas ratio and AMS (table 3). Including baseline organ damage in this multivariable model did not impact on the magnitude or significance of the association of sFasL/Fas ratio with damage accrual (OR 0.37; 95% CI 0.14 to 0.97; p=0.04).
Discussion
The Fas/FasL system has a potential role in SLE pathogenesis. Here, we examined the clinical associations of sFas and sFasL in human SLE, and investigated whether their associations with SLE are dependent on any relationship with BAFF. We found that serum sFas was associated with active renal SLE, independent of serum BAFF. We also observed that serum sFasL was associated with organ damage accrual, also independent of serum BAFF. Serum sFasL/sFas ratio was associated with disease outcomes including disease activity, flare and organ damage accrual.
In this study, we confirmed previous reports of increased levels of serum sFas and sFasL in SLE compared with HC.10 17–26 29 The sFasL/sFas ratio was not significantly different between SLE and HC after adjusting for age, in contrast to the findings of the sole previous study which investigated the use of this ratio in SLE.21 We report for the first time a positive relationship between serum BAFF and sFas in human SLE. The absence of statistically significant correlation between serum BAFF and sFas in HC may be explained by the modest HC sample size. Recent evidence in the lupus-prone BAFF-transgenic mouse model suggests a role for BAFF, a key SLE pathogenic cytokine,36 in the regulation of the Fas/FasL apoptotic pathway,39 characterised by a defect in membrane-bound form of FasL upregulation.39 The positive relationship between serum BAFF and sFas underlines the relationship of the Fas/FasL and BAFF systems, and the requirement for BAFF to be adjusted for in clinical studies of the Fas/FasL system, which should also be undertaken in autoimmune diseases other than SLE, such as primary Sjögren’s syndrome.
We found a positive relationship between serum sFas and active SLE renal disease, in line with previous smaller studies.16 18 20 52 We show that the association between serum sFas and renal disease activity was independent of BAFF, another renal SLE biomarker.53 Serum sFas may reflect not only its systemic production, but also local production in various organs, such as in situ kidney production,17 as well as being affected by kidney function.54 Although the present study cannot demonstrate any causal link, increased sFas decoy function could lead to increased immune cell survival.10 In the high serum sFas environment of autoimmune disease, the presence of oligomeric sFas15 16 could lead to proapoptotic effects on mFasL-bearing resident renal cells. The assay used in the present study did not discriminate between monomeric and oligomeric sFas forms.
Serum sFas was also associated with flare and was a predictive biomarker for overall disease activity and flare over time, also independent of BAFF. This is in line with previous studies reporting sFas as a potential predictive marker for SLE relapse.40 55 We found no association of serum sFas with organ damage, in contrast to prior smaller cross-sectional studies17 25 and one which reported an association between serum sFas and organ damage longitudinally.19 While serum levels of BAFF and sFas were correlated, associations of sFas with clinical parameters were independent of BAFF. This suggests that, while an interplay between the BAFF/a proliferation-inducing ligand (APRIL) and Fas/FasL systems has been described in a lupus-prone mouse model,39 BAFF may not be relevant to the association of sFas with SLE clinical outcomes.
Few published studies report on the relationship between serum sFasL and SLE disease activity, with most focusing on the relationship with overall activity, not phenotypic manifestations.26 30 We report for the first time a negative relationship between serum sFasL and organ damage, where high baseline sFasL was associated with lower odds of organ damage. This suggests potential for sFasL as a protective biomarker. Serum BAFF was not a confounder for this association.
The use of a ratio between sFas and sFasL has been investigated in various conditions32–35; however, only one small study has assessed its clinical relevance in SLE.21 We observed clinical associations of serum sFasL/sFas ratio with overall SLE disease activity, as well as flare of disease. We also found an association between baseline sFasL/sFas ratio and damage accrual over time. Overall, this study is the first showing significant clinical associations of sFasL/sFas ratio in SLE, particularly with organ damage accrual.
Caveats to the interpretation of the present data apply. First, although this study was conducted on a well-characterised SLE cohort, it was monocentric. Second, the HC cohort was of modest sample size, although large enough to demonstrate a significant difference in sFas and sFasL between SLE and HC. Third, the HC cohort was not age-matched to the SLE cohort; however, age was included in multivariable regression to account for this difference. Finally, in common with many such studies, the number of SLE patients suffering from manifestations such as neurological, serosal or musculoskeletal disease was small, precluding any meaningful statistical analysis in these phenotypic subsets.
In conclusion, identifying relationships with organ disease may help understanding of the Fas/FasL system as targets for therapeutic intervention. We showed that sFas, sFasL and the ratio between them were associated with SLE disease outcomes. Serum sFas was particularly associated with active renal SLE, independently of BAFF, and may be a predictive biomarker for active disease and flare. In contrast, serum sFasL and the ratio between sFasL and sFas may be new biomarkers for protection from organ damage. Further research is needed to determine whether these soluble components may be valuable therapeutic targets in SLE, particularly in lupus nephritis and damage prevention.
Acknowledgments
The authors wish to warmly thank the patients and healthy subjects for their participation in this study. They also thank the clinical staff of the Lupus Clinic at Monash Medical Centre, particularly Ms Sue Morton and Andrew Toh. The authors also thank the 360biolabs for assistance with the multiplex assays, in particular Ms Devy Santoso, and the French Society of Rheumatology for its support.
References
Footnotes
Contributors All authors contributed to experimental design, analysis and drafting of the paper. FV performed the ELISA and multiplex assays. Both FV and RK-R analysed the data. FV drafted the manuscript. All authors read and gave final approval of the version to be published.
Funding FV is a recipient of a Fellowship from Arthritis Australia. FM is a recipient of Fellowships from the NHMRC of Australia. EM was supported by the Kim Jolly Lupus Research Trust. The Monash Lupus database has received support from Arthritis and Osteoporosis Victoria, and unrestricted educational grants from GlaxoSmithKline, UCB, AstraZeneca and Eli Lilly Australia.
Competing interests EM has been a consultant to GSK and Eli Lilly. Other authors have no conflict of interest to declare.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This study was approved by the Human Research Ethics Committee, Monash Health. The study was carried out in accordance with the National Statement on Ethical Conduct in Human Research (2007).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Reasonable requests to view the data set used in this manuscript can be made in writing to FV (fabien.vincent@monash.edu).