Article Text

Abstract
Background African–Americans are historically under-represented in SLE studies and engaging them in behavioural interventions is challenging. The Women Empowered to Live with Lupus (WELL) study is a trial conducted to examine the effectiveness of the Chronic Disease Self-Management Program (CDSMP) among African–American women with SLE. We describe enrolment and retention challenges and successful strategies of the WELL study.
Methods The Georgians Organized Against Lupus (GOAL) cohort, a population-based cohort established in Atlanta, Georgia, was used to enrol a sample of 168 African–American women with SLE into the CDSMP. The CDSMP is a 6-week, group-based programme led by peers to enhance self-management skills in people with chronic conditions. Study performance standards were predefined and close monitoring of recruitment and retention progress was conducted by culturally competent staff members. Continuous contact with participants, research coordinators’ notes and regular research team meetings served to assess barriers and define strategies needed to meet the desired recruitment and retention outcomes.
Results While no substantial barriers were identified to enrol GOAL participants into the WELL study, WELL participants faced difficulties registering for and/or completing (attending ≥4 sessions) a CDSMP workshop. Major barriers were unpredicted personal and health-related issues, misunderstanding of the scope and benefits of the intervention, and transportation problems. Early implementation of tailored strategies (eg, CDSMP scheduled on Saturdays, CDSMP delivered at convenient/familiar facilities, transportation services) helped to reduce participant barriers and achieve a CDSMP registration of 168 participants, with 126 (75%) completers. Frequent contact with participants and compensation helped to reach 92.3% retention for the 6-month survey.
Conclusions Predefined standards and monitoring of participant barriers by a culturally competent research team and proactive solutions were critical to implementing successful strategies and achieving the desired recruitment and retention outcomes of a behavioural trial involving African–American women with SLE.
Trial registration number NCT02988661.
- systemic lupus erythematosus
- patient perspective
- qualitative research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
SLE is a chronic autoimmune condition that disproportionately strikes women and ethnic minorities.1 Incidence and prevalence are 10-fold to 15-fold higher in women compared with men and threefold higher in African–American women compared with their white counterparts.2–5 Mortality is threefold to fourfold higher in SLE than the general population, and African–Americans are more likely to experience poor outcomes than whites.6–8 Proper medical care and patient engagement in self-management play a major role in SLE outcomes.9–11 Yet people of African–American ethnicity and low socioeconomic status face formidable barriers to accessing healthcare and self-management education.9 12–17
Participation of high-risk SLE populations in intervention trials is a public health priority for reducing health disparities.18 However, African–Americans have been historically under-represented and engaging them in research is challenging. Moreover, while clinical trial representation of other racial minorities with SLE has increased over time, the participation of African–Americans has decreased from 2006 to 2011.19
Not only do African–American women represent a health disparities population disproportionately impacted by SLE, but this group is also at high risk for poor outcomes. Nearly 90% of nationwide hospitalised patients with SLE are women, and mortality in this group is the highest.20 21 Under-representation of African–American women limits the generalisability of findings, the provision of effective treatment and the development of tailored behavioural interventions aimed at improving self-care.22 Given the complexity of health problems associated with SLE, education is critical to promoting positive self-management practices.23–25 Although promising self-management interventions specific to SLE are currently being examined,26–28 we still lack widely available evidence-based programmes. Moreover, we are unaware of behavioural trial participation barriers of African–Americans women with SLE.
The Chronic Disease Self-Management Program (CDSMP), a community-based, evidence-based programme designed to enhance self-management skills in people with chronic conditions, may benefit African–American women with SLE.29 Since 2003, the US Administration on Aging has promoted the development of infrastructure to deliver the programme across multiple states.30 Although it is difficult to determine the number of CDSMP sites or programmes at any time, the Evidence-Based Leadership Council programme locator indicates that there is at least one and usually multiple sites offering the CDSMP in every US state.31 Although not SLE-specific, the CDSMP core curriculum addresses many of the self-care challenges faced by women with SLE. Moreover, because its widespread availability, the CDSMP can be leveraged as an accessible option for targeting African–American women with SLE in the community.
The CDSMP has demonstrated to be effective in improving self-management behaviours and outcomes in African–American populations with arthritis and multiple comorbidities.25 Building on a pilot study that reported promising benefits of the CDSMP among low-income African–American women with lupus,32 we are now conducting a 5-year behavioural trial called the Women Empowered to Live with Lupus (WELL) study. The WELL study intends to fill a need for an accessible intervention that can potentially improve outcomes in African–American women with SLE. This report provides an overview of the WELL study design, followed by the recruitment and data collection methods, and the assessment of barriers and strategies implemented to overcome recruitment and retention barriers among African–American women participating in the CDSMP.
Methods
WELL study overview
Sample
We leveraged the population-based Georgians Organized Against Lupus (GOAL) cohort to conduct the WELL study. Primarily derived from one of the five National Lupus Patient Registries supported by the Centers for Disease Control and Prevention,2 GOAL is a cohort with a large number of African–American patients with SLE from Atlanta, Georgia.33 Participants include patients from a broad socioeconomic spectrum served at community practices, and the Emory and Grady Health Systems. By 30 November 2019, GOAL encompassed 1234 adults with a validated diagnosis of SLE.
The intervention
The CDSMP is a globally disseminated, evidence-based programme designed to enhance self-efficacy to manage chronic diseases (eg, heart disease, arthritis).29 34–38 Conducted among small groups (10–16 participants) in the community by two certified peers, the CDSMP workshop consists of 6 weekly classes, each lasting 2.5 hours. Lay leaders are trained and certified according to the Self-Management Resource Center (previously the Stanford Patient Education Center) protocol. Classes are highly participative through weekly action plans, behaviour modelling, vicarious learning, problem solving and peer support. The CDSMP addresses self-management challenges that are universal across chronic conditions, including pain and fatigue, symptom and medication management, communication with family and professionals, managing emotions, exercise, and healthy eating. Participants must attend ≥4 classes to be a ‘CDSMP completer’.
Study design
We implemented a two-group longitudinal cohort study nested within GOAL to examine changes in outcomes between participants enrolled in the CDSMP (hereafter called the WELL cohort) and the remaining GOAL participants not exposed to the intervention (the Usual Care cohort). Given the long-standing (>8 years) relationship between GOAL participants and the research staff, this is a cost-effective approach to recruit and examine an adequate sample size and obtain a representative sample of African–American women with SLE from metropolitan Atlanta (figure 1).

Overview of the study design. AA, African–American; CDSMP, Chronic Disease Self-Management Program; GOAL, Georgians Organized Against Lupus; WELL, Women Empowered to Live with Lupus study.
CDSMP recruitment, data collection and barriers assessment
Research coordination team
Three black/African–American female research coordinators (RC) with experience in research among ethnic minorities with SLE were responsible for recruitment and data collection, and participated in barriers assessment and resolution.
Recruitment
We selected a random sample from GOAL using the following inclusion criteria: (1) self-reported African–American race; (2) female sex; (3) meeting ≥4 American College of Rheumatology (ACR) criteria for the classification of SLE or meeting 3 ACR criteria and having a documented diagnosis of SLE by a board-certified rheumatologist; and (4) residence in metropolitan Atlanta, where community-based CDSMP workshops are provided. Women selected received a phone call by the RC explaining the study. Among those interested, the RC discussed the commitment needed to ensure study integrity and assessed exclusion criteria. Exclusion criteria were participation in the CDSMP in the past 5 years and cognitive impairment, which was screened via telephone using the Six-Item Screener tool.39 Eligible women were mailed a recruitment packet, which included a flyer, the consent, schedule and location of upcoming CDSMP workshops, and staff contact information. A form to enter participants’ preferred contact method, workshop time availability and transportation preferences was also included. The Emory Institutional Review Board approved the informed consent to be conducted via online, telephone or in person. Recruitment was finalised once a consented participant was registered in a specific CDSMP workshop.
The Usual Care cohort encompassed GOAL participants who at baseline met the same inclusion criteria as WELL participants, but were not exposed to the CDSMP (shaded square in figure 1). Using data from our pilot study, we calculated that a sample of 150 WELL and 242 Usual Care participants would provide 80% power to demonstrate a clinically meaningful improvement (2.5 points change) in patient-reported outcomes after the CDSMP.32
CDSMP registration
Most CDSMP workshops delivered in Atlanta are coordinated by the Atlanta Regional Commission (ARC), which is the regional planning and intergovernmental agency that provides community services to residents of metropolitan Atlanta and is licensed to deliver the CDSMP. Workshops schedule and location were coordinated between the RC and the ARC to facilitate the registration of WELL participants into workshops at convenient locations and schedules. The importance of attending all CDSMP classes was emphasised during recruitment. Workshop registration was finalised by the RC via telephone after a participant provided her availability through the paper form or a phone contact. Options for transportation to the CDSMP classes included a $10 subway or gas card, or a round-trip ride (Uber/Lyft). Weekly phone calls were conducted among CDSMP participants to assess classes attendance and provide transportation compensation or the upcoming ride service.
Measures and data collection
Measures were selected to minimise participants’ burden (table 1). We deliver one preintervention and three postintervention (6-month, 12-month, 18-month) surveys in the WELL cohort and four surveys separated by 6 months in the Usual Care group. We have been successfully using the Dillman’s Total Design Method with minor modifications to obtain high survey response rates.40 It is based on the social exchange principle and operational aspects to minimise costs and maximise rewards for responding, and establish trust that rewards will be delivered. Participants have multiple options for completing the surveys, and the average duration for responding the WELL survey is 40 min. Reminders are conducted through emails, text messages or phone calls. WELL participants receive gift cards of $35, $40, $45 and $50 for completing the baseline, 6-month, 12-month and 18-month assessments, respectively.
Summary of self-reported measures
Project management procedures
Performance standards were established by defining specific recruitment, retention and data collection targets. We implemented strategies that have been shown to be successful over the years, including training staff in outreach, recruitment and retention of minority individuals, building trustful interactions, frequent contact with participants, and face-to-face enrolment when possible. A Health Insurance Portability and Accountability Act (HIPAA)-compliant project management system was built to track WELL operational tasks, allowing us to run searches and progress reports of subjects reached, refused, unable to participate, interested, screened, consented and registered into a CDSMP workshop. The system was also configured to report class attendance and completion of postintervention data collection time points, and take text notes.
Assessment of recruitment and retention barriers
The RC conducted phone calls among consented participants to coordinate CDSMP registration and assess CDSMP classes attendance. Individualised notes were taken at each telephone encounter to capture participant barriers related to the different phases of the study, including reasons for missing classes. Monthly meetings were conducted among all research members to discuss progress, barriers and possible solutions. Meetings were also conducted with ARC partners to discuss barriers related to CDSMP workshop scheduling.
Results
Recruitment of the WELL cohort
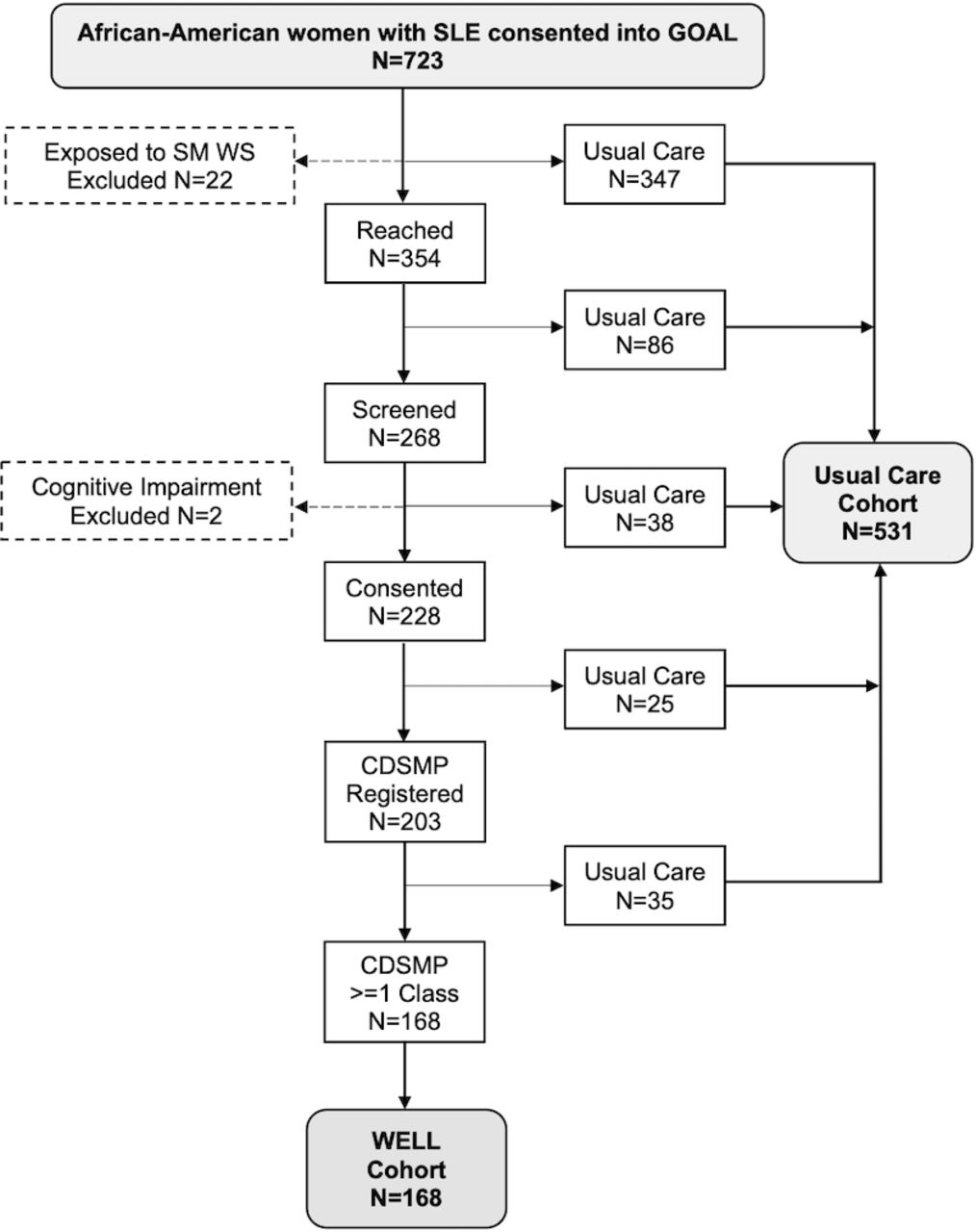
Recruitment from a GOAL sample of 723 African–American women with SLE began in January 2017 (figure 2). Twenty-two participants were excluded because they reported exposure to an inperson self-management workshop in the past 5 years. By April 2019, 354 randomly selected women were reached and 268 (75.7%) who were interested in the CDSMP were further screened for cognitive impairment. We excluded two who tested positive and confirmed that none of the screened participants attended the intervention within the last 5 years. Of 266 eligible women, 228 (85.7%) consented to participate. Of the 228, 203 (89.0%) registered into a CDSMP workshop and 168 of 203 (82.8%) attended at least one CDSMP class by May 2019, comprising the WELL cohort. The Usual Care cohort encompassed 531 GOAL participants not exposed to the intervention. Table 2 describes the baseline characteristics of participants.

Recruitment of the WELL and Usual Care cohorts. CDSMP, Chronic Disease Self-management Program; GOAL, Georgians Organized Against Lupus; SM, self-management; WELL, Women Empowered to Live with Lupus study; WS, workshop.
Baseline characteristics of WELL and Usual Care participants
Expected and achieved recruitment
We projected to consent an average of 10 WELL participants/month to achieve a sample of 150 participants in 2 years (blue line in figure 3). We also expected that 150 WELL participants would attend the CDSMP by 30 May 2019. No substantial barriers were identified to recruit GOAL participants into the WELL cohort (figure 3); however, early in the study we learnt that WELL participants faced barriers to registering for and/or attending the CDSMP classes (see the following section). We revisited our approach by consenting a higher number of participants than the actual sample size needed in the intervention arm, allowing to have a sufficient pool of participants to take part into upcoming CDSMP workshops. Monthly recruitment progress of the WELL cohort is depicted in figure 3.

{kind=link}
{kind=link}
{kind=link}
Monthly recruitment, CDSMP registration and CDSMP attendance. CDSMP, Chronic Disease Self-management Program; WELL, Women Empowered to Live with Lupus.
Participation in the CDSMP and retention in the study
We faced challenges in accommodating WELL participants into existing CDSMP workshops. The most significant ones were (1) workshop cancellation due to low enrolment; (2) frequent no-shows or last-minute cancellations to attend a specific workshop; and (3) low workshop completion rate (table 3). We also identified a relatively low rate of 6-month survey responses (80.9% respondents within the first year). We describe the main challenges and the strategies implemented to overcome these challenges.
Summary of recruitment and retention of African–American women with SLE into the CDSMP: challenges, barriers, strategies and outcomes
CDSMP registration
We encountered difficulties matching participants’ preferences with available CDSMP locations and schedules, causing a relatively low rate of CDSMP registration in relation to the number of participants consented. We implemented several strategies aiming at increasing the number of workshops that would meet the needs of our participants. First, the research staff provided support to the ARC with the coordination and delivery of CDSMP workshops. We constantly assessed the most convenient locations and schedules among WELL participants and informed the ARC coordinator about participants’ preferences. Second, in addition to community centres nearby study participants’ residency, workshops were delivered at facilities located at Grady and Emory campuses, which were found to be very convenient and familiar to many participants. Of the 42 CDSMP workshops delivered in a 2-year period, 28 (66.7%) took place in libraries, community health centres and churches, and the remaining 14 (33.3%) in Grady and Emory facilities. Additional workshops were delivered in the afternoons, and nine (7.1%) were scheduled on Saturdays. We also increased the number of WELL participants registered into each workshop to avoid CDSMP cancellations due to insufficient participants. As a result, among 228 women consented, 203 (89%) registered into a CDSMP. The cumulative proportion of participants registered into the CDSMP in relation to those consented increased from 43.4% by the 12th month to 89.0% by the end of the intervention period. As shown in figure 3, a peak in CDSMP registration and attendance occurred between the 23rd month and the end of the intervention phase, which coincided with the delivery of seven workshops at Emory and Grady facilities, three of which were scheduled on Saturdays (figure 3). Because CDSMP registration not only targeted recently consented participants, but also those who had been waiting to be accommodated, the total number of participants recruited into the CDSMP was 168 (black line in figure 3), slightly surpassing the initial estimate of 150 (blue line in figure 3). Eighty-two participants attended a workshop with other members of the community and the remaining 86 attended workshops exclusively with other participants with SLE.
Participant cancellation or no-shows after being registered into a CDSMP workshop
Additional challenges were last-minute cancellations to attend a specific CDSMP workshop or no-shows without notice. Two major barriers were recognised in relation to these challenges: (1) competing demands (eg, health issues, job schedule changes, childcare needs) and (2) lack of a clear understanding of the purposes and scope of the intervention. To reduce these barriers, we increased the number of workshops delivered on Saturdays and offered opportunities to register in an upcoming workshop to those participants who were still interested in the CDSMP. Additionally, we increased our efforts to better inform participants about the scope, commitment and goals of the CDSMP at multiple points during the recruitment processes. We used feedback from CDSMP completers and secondary data from a qualitative substudy to produce additional recruitment materials, including a short video that provided culturally relevant information about the intervention and a CDSMP participant’s testimony.11 41 Messages from those materials served to align the goals of the intervention with the self-management needs of our population. Additionally, we offered a standardised 1-hour information session prior to class 1, known as ‘Session Zero’, to nearly 200 participants who had not registered into the CDSMP.42 Among 56 participants interested, 28 were able to attend, 11 were unavailable and 17 missed the session. This activity served to demonstrate the interactive nature of the workshop, encouraging enrolment at the end of the session. CDSMP attendance increased from 45 to 123 participants in the first and second half of the recruitment period, respectively.
CDSMP completion rate
In the first 6 months of the intervention phase, 11 of 17 (64.7%) participants completed four or more CDSMP classes, a rate substantially lower than the 75% reported nationwide.42 The weekly phone calls conducted by the RC provided insightful feedback about attendance barriers. Unexpected demands from the underlying disease (eg, lupus flares, hospitalisations, medical appointments) or personal issues (eg, childcare needs, job demands) were identified as major barriers. To overcome these challenges, non-completers were given the opportunity to start another CDSMP workshop if they were motivated to do so. Additional barriers among non-completers included variable transportation needs over the 6-week CDSMP duration and forgetfulness about the next-week class. To address these, each participant was offered flexible weekly transportation options and received reminder messages the day before the upcoming class. To maintain engagement, a non-monetary token (WELL study bag and greeting card) was mailed to those who completed the third class. As a result, the CDSMP completion rate increased from 64.7% to 80.0% in the first and second 6 months of the intervention phase. The overall completion rate reached 75.0%. A slightly higher completion rate was observed for workshops delivered on Saturdays (76.6%) compared with weekdays (74.0%).
WELL cohort 6-month retention
Our project management system allows RC to track survey delivery and completion dates and take centralised notes across studies at each participant’s encounter. These notes facilitated a personalised approach to address participant barriers and preferences to effectively provide data. Evaluation of postintervention data collection rendered an 80.9% rate of 6-month responses within the survey schedule in the first year. Major barriers were competing demands (eg, health and personal life events, participation in other studies) and forgetfulness. To increase retention, we applied a ±3-month window to each time point of data collection and made more frequent contact with participants to send reminders. Moreover, participants seen at our outpatient lupus clinic were offered the opportunity to complete any outstanding survey in a private room. We continued implementing successful retention strategies, such as flexible survey delivery modes (email, mail or by phone) and both monetary and non-monetary incentives. The 6-month response rate increased to 98.9% for surveys scheduled within the second year. Overall, 155 of 168 (92.3%) participants completed the 6-month postintervention survey.
Discussion
This report describes the methods implemented to recruit and retain African–American women with SLE into the CDSMP, a 6-week, group-based, generic self-management education programme. Within a 2-year period, 168 African–American women with SLE attended the CDSMP, 126 (75%) completed ≥4 weekly classes and 155 (92.3%) responded to the 6-month postintervention survey. We encountered, however, various challenges in meeting the desired study goals, which can be grouped into two major categories: (1) CDSMP coordination to accommodate participants’ needs and (2) participant barriers to attending and completing the programme.
CDSMP coordination
CDSMP workshops in Atlanta are primarily delivered by organisations that largely target the chronically ill and elderly population and coordinated by the ARC, which is licensed to deliver CDSMP in metro Atlanta.43 Consequently, it was difficult to match the most common workshop locations (senior centres) and schedules (morning days of the week) with our participants’ preferences. Strategic solutions included a tight coordination between the study staff and the ARC to deliver conveniently located workshops, including healthcare facilities familiar to our participants. Moreover, afternoon and Saturday CDSMP workshops enabled attendance of those who had medical appointments, full-time jobs or caregiver commitments. We also consented a larger number of participants to reduce the likelihood of workshop cancellation associated with insufficient number of participants.
Participant barriers
SLE poses a substantial toll to African–American women, with multiple negative consequences on their lives. With over 80% of the study population reporting some type of organ damage and 60% being unemployed or disabled, unpredicted health-related and personal-related problems were common threats to CDSMP attendance and completion. The average scores of SLE activity, physical health, mental health and depression suggest that many of these patients may not have had adequate control of the disease and comorbidities. Since these factors lead to poor outcomes and higher healthcare utilisation, our participants frequently faced barriers to attending the 6-week CDSMP classes. Other studies have emphasised that demands from family, work and stressful life events are challenges often faced by minorities, which can limit their engagement in interventional studies.44 45 More flexible and additional workshops contributed to increased attendance from 45 to 123 participants in the first and second half of the study period.
Other studies among African–Americans have identified mistrust as a major recruitment barrier.46 Since our team has built a long-standing relationship with GOAL participants, mistrust was not perceived as an issue in our study. However, despite the experience of the research team working with African–Americans, some women showed a poor understanding of the objective and structured nature of the CDSMP. Cultural adaptations of the recruitment materials, frequent communication with participants and the implementation of a demonstration session helped women align their expectations with the objectives of the intervention. These measures have been adopted by others as effective strategies to engage African–American in clinical trials and may have contributed to the reduced number of last-minute cancellations and no-shows in our study.47 Other procedures that helped to overcome retention challenges were weekly class reminders, non-monetary rewards and transportation support. The importance of these strategies in increasing trial retention among minority populations has been emphasised in other studies.42 48–50
Our study has limitations. First, we did not conduct a formal qualitative assessment of barriers and potential solutions. However, experienced RCs took notes and provided ongoing insight that served to successfully modify our recruitment and retention procedures. Second, in order to reduce participants’ barriers to workshops attendance, we implemented procedures (eg, class reminders, non-monetary compensation) that represent deviations from the real-world CDSMP. Third, to achieve the desired sample size within the study timeline, some of the workshops were attended exclusively by study participants. Interestingly, WELL women who also participated in a qualitative substudy did not raise organic concerns about the diverse composition of the CDSMP groups.11 41 A deeper assessment is warranted to determine the influence of demographic and disease-related factors on the programme outcomes. Fourth, findings of this study are best generalised to African–American women in the Southeastern USA and not to other racial/ethnic groups and in other regions or countries. Fifth, the lack of RCs might impact participation of patients with SLE in the real-world CDSMP. However, providers and organisations that advocate for patients with lupus can play a key role by referring patients and providing support to the most vulnerable groups. Alternative community-based strategies that might work for this population include internet-based CDSMP, CDSMP delivered by organisations who target minorities with lupus, and video conference for participants who attended first class but have mobility or transportation challenges at the time of other classes.
The strengths of our study include the intentional focus on identifying recruitment and retention challenges, and a proactive and nimble research team able to implement strategies to reduce barriers. We did not consider altering the 6-week programme delivery protocol since this study is designed to evaluate the effects of a widely available community intervention among our high-need minority population, rather than to develop a new intervention. The overall completion rate (75%) in this sample, however, is relatively high considering that lupus is a complex condition with high prevalence of comorbid conditions and symptoms that wax and wane. Although some solutions to reduce barriers to workshop attendance were facilitated by the research grant (eg, reducing transportation costs), many others could be implemented in the community because they were either free (hold classes at convenient locations, hold Saturday classes, overenrol to avoid workshop cancellations) or low cost (reminder calls/texts, token incentives). In addition, the design enabled recruitment of a large number of participants who have been historically under-represented in research, proving to be a feasible option to save time and costs.
In conclusion, by establishing performance standards and conducting constant assessment of progress and barriers, we were able to adjust our strategies to meet the desired recruitment and retention outcomes. A trustful relationship through culturally competent research members, trial information that aligns participants’ needs and intervention outcomes, transportation support, and flexibility to consider personal and illness-related demands of participants were fundamental strategies to successfully engage and retain a large cohort of African–American women with SLE into a generic, group-based self-management programme. Should further findings support a benefit of the CDSMP among African–American women with SLE, the feasibility of implementing these strategies in the real world may be considered to facilitate the participation of this minority in the CDSMP.
Acknowledgments
The authors acknowledge the research team members, Letheshia Husbands, Aita Akharume and Meaza Girmay, who were fundamental to achieving the successful recruitment and retention outcomes for this trial. The authors also want to thank Lynda Conner and Kristie Sharp from the ARC for their support to our study, and GOAL and WELL participants for their commitment to SLE research.
References
Footnotes
Contributors All authors were involved in drafting the article and/or critically revising it for important intellectual content, and all authors approved the final version to be published. CD, KE, SSL and TB contributed to the study conception and design. CD-T and GB contributed to acquisition of data. All authors contributed to analysis and interpretation of data.
Funding The WELL study is funded by the National Institute on Minority Health and Health Disparities (R01MD010455). The GOAL cohort is supported by the Centers for Disease Control and Prevention (CDC-U01DP005119 and CDC-U01DP006488). The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval The study was approved by the Emory Institutional Review Board and Grady Health System Research Oversight Committee. All study participants signed informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no data sets generated and/or analysed for this study. All data relevant to the study are included in the article or uploaded as supplementary information. The WELL study is an ongoing behavioural trial registered on 7 December 2016. We will share individual de-identified data (and metadata and trial documents) via a data use agreement after the study is completed and primary papers are published. Individual de-identified data provided in this report are available upon reasonable request (or a data use agreement). The assessment of recruitment and retention challenges, as well as strategies to overcome barriers reported in this study, was an organic process that took advantage of ongoing notes by research staff and discussions by the research team (primarily qualitative data). Thus, no individual data are available and data sharing is not applicable to this specific study.
Author note Although the study was performed in the US, this report includes traditional English terms to meet the UK editorial style.