Article Text

Abstract
Objective To scope and summarise available literature on the outcomes of pregnancy and associated factors in sub-Saharan African women with SLE.
Methods Electronic databases and reference lists of retrieved articles were searched to identify relevant studies published from 1 January 2000 to 28 October 2019. Data were combined through narrative synthesis.
Results We included four studies retrospectively reporting a total of 137 pregnancies in 102 women over a 26-year period. Mean age at conception ranged from 27.2 to 39.9 years. Kidney damage, the predominant organ manifestation before conception, was reported in 43 (42.2%) patients. Ninety-seven (70.8%) pregnancies resulted in 98 live births. SLE flares occurred in 44 (32.2%) pregnancies, mainly skin (20.4%) and renal (18.2%) flares. Major adverse pregnancy outcomes (APOs) were preterm birth 38.8%, low birth weight 29.8%, pregnancy loss 29.2% and pre-eclampsia 24.8%. The main factors associated with APOs were nephritis and SLE flares.
Conclusion Over two-thirds of pregnancies resulted in live birth in this cohort of sub-Saharan African women with SLE. The main APOs and associated factors described in other parts of the world are also seen in this region, but with high rates of APOs. A large prospective multinational study is warranted for more compelling evidence.
- lupus erythematosus
- systemic and outcome assessment
- qualitative research
- health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Extensive research on SLE pregnancies has dispelled the myth that SLE is incompatible with pregnancy, and led to the development of recommendations on planning and management of pregnancy in women with SLE.1–12 As a result, the overall outcome of SLE pregnancies has markedly improved in developed countries over the last decades.13 14
SLE predominantly affects young women in sub-Saharan Africa as well.15 However, there is limited knowledge on pregnancy in sub-Saharan African women with SLE. Relevant data are needed to fill this knowledge gap and inform treatment and preventive strategies within the region. We therefore conducted a review to map and collate available evidence on the outcomes of pregnancy and associated factors in sub-Saharan African women with SLE.
Methods
This review is written according to standards for reporting scoping reviews.16 17
Data sources and search strategy
MEDLINE (PubMed), ExcerptaMedica database (EMBASE) and African Journals Online (AJOL) were searched to select pertinent articles released from 1 January 2000 to 28 October 2019. The search strategy used in PubMed (online supplementary table S1) combined MeSH terms referring to SLE, pregnancy as well as the names of sub-Saharan African countries,18 and was adapted to fit with search requirements in EMBASE and AJOL. These electronic searches were supplemented by hand searches.
Supplemental material
Study selection
Only longitudinal studies published in English or French language were included. Participants were pregnant sub-Saharan African women with SLE (according to the 1997 American College of Rheumatology classification criteria19) residing in sub-Saharan Africa. Parameters of interest were outcomes of pregnancy and associated factors.
Study selection was independently run by two investigators (ME and JRN), and discrepancies between both of them were resolved with the arbitrage of a third investigator (JJB). After initial screening of titles and abstracts, the full texts of papers deemed potentially eligible were further assessed before final inclusion.
Data charting
The following data were independently extracted by two investigators (ME and KM): study characteristics, year of publication, baseline demographics, SLE characteristics and parameters of interest. We performed a narrative synthesis due to small study sample sizes and high heterogeneity across studies.
Results
Study selection
Of 2693 papers, four20–23 were included in this review as described in figure 1.

PRISMA flow chart of the study selection process.
Characteristics of included studies
The four studies retrospectively reported a total of 137 pregnancies in 102 women who had a joint follow-up in Rheumatology/Internal Medicine and Obstetrics urban centres during 1992–2018. Details on study characteristics are found in table 1.
Characteristics of studies reporting the outcomes of pregnancy in sub-Saharan African women with SLE during 2000–2019
Baseline demographics and SLE features
Patients’ demographics are summarised in table 1. The mean age at conception ranged from 27.2 to 39.9 years. Before conception, 43 (42.2%) women had kidney damage, the most common organ manifestation. Of these, 40 had biopsy-proven lupus nephritis (LN): eight class IV, one class II, two class III and 29 unclassified.
SLE activity in pregnancy
Flares were observed in 44 (32.2%) pregnancies: 28 (20.4%) cutaneous, 25 (18.2%) renal and 28/90 (31.1%) joint flares. Anti-Ro/La, antiphospholipid (aPL), antinuclear antibodies and anti-deoxyribonucleic acid (anti-DNA) autoantibodies were found in 15/48, 7/50, 6/7 and 5/6 pregnancies, respectively, while low complement levels were detected in 14/51 pregnancies.
Pregnancy outcomes
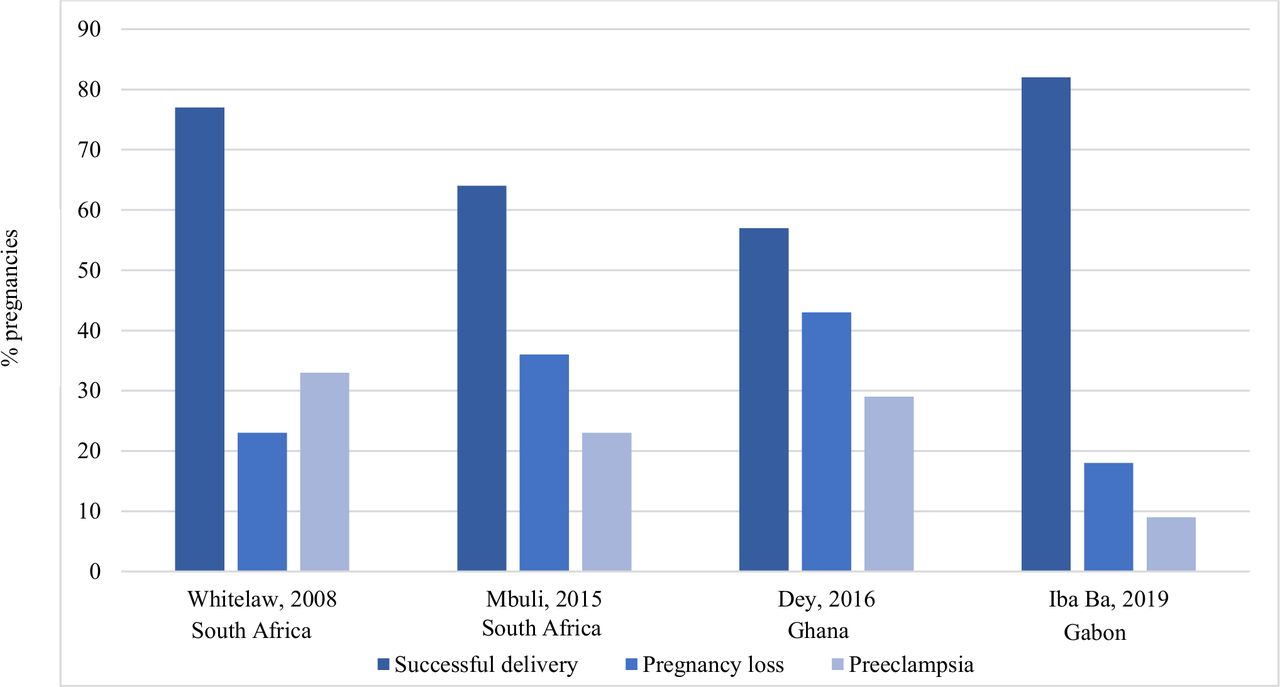
In mothers, there were overall 97 (70.8%) successful deliveries with live birth, 40 pregnancy losses (29.2%) and 34 (24.8%) pregnancies with pre-eclampsia. Of 40 pregnancy losses, 27 were miscarriages, nine stillbirths and four therapeutic abortions. No maternal deaths were recorded. Figure 2 highlights the main obstetric outcomes.

Main obstetric outcomes in sub-Saharan African women with SLE.
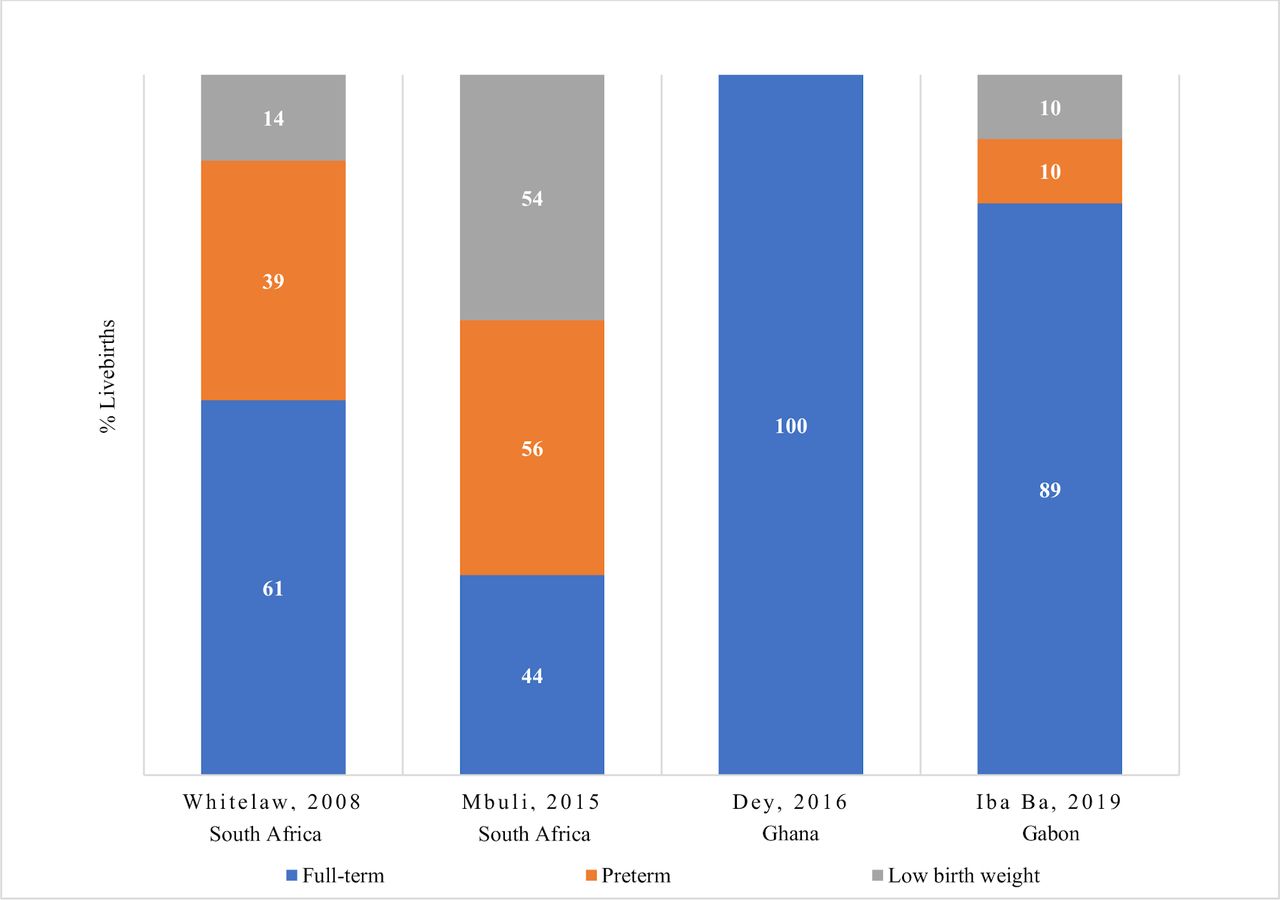
Of 98 live births, 60 (61.2%) were full term and 38 (38.8%) preterm. Other adverse neonatal outcomes were neonatal lupus 3 (3.1%), low birth weight 28/94 (29.8%) and neonatal death 16/39. The main neonatal outcomes are depicted in figure 3.
{kind=link}
{kind=link}
{kind=link}
Main outcomes in neonates born to sub-Saharan African women with SLE.
Factors potentially associated with adverse pregnancy outcomes (APOs)
Preterm delivery, fetal loss, pre-eclampsia and neonatal death respectively occurred in 18, 17, 11 and three of 49 pregnancies in which (history of/active) LN was documented. Preterm delivery and intrauterine growth restriction respectively occurred in six and three of 19 pregnancies in which Raynaud’s phenomenon was observed. Fetal loss, preterm delivery and hypertensive disorders respectively occurred in seven, six and three of 17 pregnancies in which SLE flares were observed. Of 15 pregnancies in which hypertensive disorders were diagnosed, five and four ended with preterm birth and fetal loss respectively. Of 15 anti-Ro/La-exposed fetuses, three developed neonatal lupus and one was lost. Preterm delivery, low birth weight and LN occurred in nine, two and one of 15 pregnancies in which low complement levels were detected. Of 11 aPL-exposed pregnancies, five and three ended with fetal loss and preterm delivery.
Medications and APOs
Drugs used during pregnancy (evaluated on 90 pregnancies) were glucocorticoids 77.8%, antimalarials (hydroxychloroquine/chloroquine) 63.3%, antihypertensives 35.5%, azathioprine 25.8%, ciclosporin 6.7% and low-dose aspirin 8.9%. Of 29 pregnancies with drug exposure-outcome data, seven pregnancies were lost. All of these had been exposed to hydroxychloroquine and prednisone, add-on drugs being used in five (aspirin), four (azathioprine) and two (antihypertensives) pregnancies, respectively. No special drug safety issue was raised.
Discussion
In this largest cohort of SLE pregnancies from sub-Saharan Africa, the overall rate of live birth was 70.8%. SLE flares occurred in 32.2% of pregnancies and the main APOs were pregnancy loss (29.2%), pre-eclampsia (24.8%), preterm birth (38.8%) and low birth weight (29.8%). The major factors associated with APOs were (history of/active) LN and SLE flares.
Our estimate of SLE flare during pregnancy is consistent with previous rates of 13% to 75%,4 24–27 but higher than those found in two large cohorts including mostly women with stable or mild/moderate SLE at conception.4 27 Beyond the influence of discrepancies in the definition of flare across studies, the difference observed may also be due to the inclusion of a substantial proportion of women with severe SLE at conception in our population.10 28 The high prevalence of kidney disease prior to conception and the substantial use of glucocorticoids during pregnancy further support this assumption,14 29 although SLE activity measures are lacking.
The APOs described here are the main APOs in women with SLE.2 14 The rate of pregnancy loss is similar to that of a recent Malaysian cohort which included mostly women with unplanned pregnancies and severe SLE.29 It is lower than that of a Chinese cohort which also reported a higher rate of flare than that found here.30 Our rate of preterm birth is comparable with those of the aforementioned Malaysian cohort29 and a Scandinavian group with severe SLE.11 It is higher than the rate found in another Malaysian cohort including mostly women with stable SLE at conception.31 These observations, together with knowledge that SLE activity is a major risk factor for APOs,1 4 11 29 30 support the association between flare and APOs that we observed. Since LN is the most deleterious organ activity and even a history of LN heightens the risk of APOs,1 2 29 our finding that LN was the main factor associated with APOs is not surprising. The most common LN-related APO is pre-eclampsia.2 14 Accordingly, the high rate of pre-eclampsia likely ensued from that of LN. Indeed, the prevalence of pre-eclampsia is substantially higher than that found in most studies from other regions of the world,2 11 27 29 31 although prevalence rates of up to 35% have been reported.14 32 The increased rate of low birth weight may also be due to the high prevalence of pre-eclampsia which is one of its major risk factors.14
Taken collectively, our results suggest that advances in SLE management over the last decades6 33 34 may not have greatly influenced the overall outcome of SLE pregnancies in sub-Saharan Africa, as lower proportions of APOs were expected based on contemporary data from other parts of the world.2 4 10 11 31 To reach optimum rates of successful pregnancies4 10 11 in sub-Saharan Africa, strengthening of preconception counselling, risk stratification and monitoring of pregnancies are therefore paramount. In counselling women, a history of LN should engender apprehension, similarly as active SLE. Patient adherence to preconception counselling is likely with timely achievement of disease quiescence (eg, using the ‘treat-to-target’ strategy),34 as young sub-Saharan African patients face societal expectations to give birth. Accurate risk stratification and close monitoring of pregnancies entail early identification of at-risk patients8 12 14 and optimal assessment of maternal SLE activity35 36 as well as fetal health throughout pregnancy. All these tasks can be well accomplished if more caring physicians (eg, rheumatologists, gynaecologists) are trained and relevant paraclinical examinations8 12 14 (eg, autoantibodies, serum complement level, kidney biopsy and ultrasonography) are made available and affordable in sub-Saharan Africa. As SLE is not a priority for limited health budgets of sub-Saharan African states, we need a support from lupus funding bodies for capacity building in our laboratories, so as to make these tests locally available at affordable costs.
Limitations of this review reflect the low to moderate quality of included studies. First, their retrospective nature and aforementioned resource constraints have introduced selection and reporting biases in our results. For instance, information on drug adherence (an unresolved issue in SLE37 38) was missing, which precludes clear conclusions about drug safety on fetus. Furthermore, we did not assess the influence of ethnicity on our results due to incomplete data on ethnic distribution. Nevertheless, black women were majority, and other groups were still of African ancestry. The predominance of black women may notably explain the high rate of kidney involvement in this population, as SLE-related renal damage is highly prevalent in black Africans.15 39 Second, no causal link was demonstrated between observed outcomes and associated factors. Notwithstanding these shortcomings, we provide a snapshot of the outcomes of SLE pregnancy and associated factors in sub-Saharan Africa. More compelling evidence is needed from a large multinational prospective cohort.
Conclusion
A considerable proportion of pregnancies in women with SLE result in live births in sub-Saharan Africa. The main APOs are the same that have been reported in the other regions, but with high rates. The major factors associated with APOs are SLE flare and LN. High-quality evidence is needed for definite conclusions.
References
Footnotes
Presented at the 12th European Lupus Meeting, March 2020 Poster presentation P78, published in Lupus Science and Medicine, March 2020, Vol 7, suppl 1, doi: 10.1136/lupus-2020-eurolupus.123
Contributors Conception and design: ME, JJB. Search strategy conception and application: ME, JJB. Study selection: ME, JRN. Data extraction: ME, KM, PT. Data synthesis and analysis: ME. Manuscript drafting: ME. Manuscript revision: GAN, SR, EH, JJB, JRN, KM, PT. All authors approved this document. ME is the guarantor of the review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.