Article Text

Abstract
Objective Given the increasing relevance of the ANA assay to classification of SLE and the uncertainty and variation surrounding different ANA assay performance, we compared the human epithelial type 2 (HEp-2) to mouse liver (ML) substrate in our local cohort and provided a review of the evidence for their use in autoimmune rheumatic diseases (ARDs).
Methods Electronic health record data (2003–2008) were used to identify patients who had concurrent HEp-2 and ML ANA, and a diagnosis of SLE or other ARDs. We determined the agreement between HEp-2 and ML ANA regarding positivity, titre and pattern, and their predictors. Sensitivity of HEp-2 ANA, ML ANA, repeating HEp-2 ANA, and combining HEp-2 and ML ANA assays was assessed.
Results There were 961 patients with concurrent HEp-2 and ML ANA samples, including 418 SLEs. There was generally fair to moderate agreement in HEp-2 and ML ANA (kappa (κ)=0.35–0.79), titres (κ=0.34–0.79) and patterns (κ=0.35–0.93). In SLE, the presence of anti-dsDNA antibodies was predictive of ANA agreement between HEp-2 and ML ANA (adjusted OR 6.27, 95% CI 1.45 to 27.20, p=0.01). The ANA sensitivity for most ARDs was highest when the HEp-2 test was repeated, followed by when the HEp-2 and ML ANA were combined and when only the HEp-2 or ML ANAs were used.
Conclusion In keeping with prior studies, we demonstrated that there was fair to moderate agreement between HEp-2 and ML assays in the largest comparison of HEp-2 and ML as substrates for ANA testing in various ARDs. Furthermore, ANA sensitivity was higher when the HEp-2 assay was repeated rather than combining HEp-2 and ML.
- systemic lupus erythematosus
- autoantibodies
- autoimmunity
- autoimmune diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The methodology of ANA tests has changed, yet the ANA indirect immunofluorescence assay (IFA) test remains one of the most important assays to facilitate the diagnosis of autoimmune rheumatic diseases (ARDs). The indications for ANA testing have expanded from SLE to include other ARDs, such as scleroderma, interstitial lung disease, autoimmune liver disease and inflammatory myopathies.1 2 Laboratories attempted originally to use a range of different tissues as sources of intracellular nuclei to improve the indirect IFA, including human gastric parietal cells, cardiac muscle, skeletal muscle, kidney, adrenal gland, colon mucosa,3 mouse and rat kidney,4 human fetal fibroblasts,5 rat liver,6 KB cells7 and mouse liver (ML).8
To standardise the substrate for ANA IFA testing, most, if not all, labs had switched by the early 2000s to a cell line, human epithelial type 2 (HEp-2), to create a uniform source of cell nuclei for the ANA test. Furthermore, the cells and nuclei were much larger in HEp-2 and hence were easier to read for nuclear patterns compared with ML and other differentiated tissues. However, to our knowledge, evidence to assert that HEp-2 is superior to other substrates, including ML for ANA evaluation, had been limited to small cohort studies.7 9–14 Even with the development of solid-phase assays, HEp-2 is still regarded by most as the gold standard ANA test.15
Due to this uncertainty, between 2003 and 2008, the Brigham and Women’s Hospital (BWH) Clinical Immunology Laboratory had a transition period during which both HEp-2 and ML ANA tests were performed on the same sera for all ANA tests ordered clinically. Herein we present a historical review of substrates for ANA testing using a large local dataset to compare ANA IFA on HEp-2 and ML substrates on patients with various ARDs. We also determined whether a combination of the two techniques improves ANA sensitivity for the detection of various ARDs. Combinations of ANA assay platforms have been proposed as a solution to the use of a single method for ANA detection (HEp-2 IFA or an equivalent solid-phase assay) in the new American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria for SLE, where the ANA is the entry criterion.16–18 This has generated great interest and controversy on the role of ANA testing in SLE classification, highlighting the need for more clarity.
Materials and methods
Study population
We used the Partners Research Patient Data Registry (RPDR) to identify patients who had an ANA test by both HEp2 and ML IFA from 2003 to 2008 at the BWH, Boston, Massachusetts. The RPDR is a centralised clinical data warehouse that contains electronic health record information for more than 6.5 million patients seen in the Partners HealthCare Network, providing care for approximately half of the population in the greater Boston, Massachusetts, area.
Among the patients who had ANA testing during the period when both assay substrates were used, we identified those with the following diagnoses using the RPDR query tool: SLE, dermatopolymyositis (DM/PM), rheumatoid arthritis, Sjögren’s syndrome (SS), mixed connective tissue disease (MCTD), systemic sclerosis (SSc), and primary or secondary antiphospholipid syndrome (APS). Diagnoses were recorded in RPDR as International Classification of Diseases, Ninth Revision (ICD-9) or International Classification of Diseases, 10th Revision (ICD-10) codes. Patients were required to have at least two ICD-9 or ICD-10 codes to have the disease. We (PS and MYC) then performed a manual electronic medical record review to identify controls who did not have an underlying autoimmune disease but did have musculoskeletal complaints. We also collected demographic information (age, sex and self-reported race/ethnicity) and other autoantibody test results (anti-double-stranded DNA (dsDNA), anti-La/SS-B, anti-ribonucleoprotein (RNP), anti-Smith (Sm) and anti-Ro/SS-A) from the medical records.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
ANA and autoantibody assays
Sera from patients at BWH had been sent to the BWH Clinical Immunology Lab for ANA testing. Sera were kept at 4°C prior to testing and were generally tested within 4 days after phlebotomy. ANA IFA with HEp-2 cells were performed using kits by one manufacturer, Kallestad kits (Bio-Rad Laboratories, Benicia, California, USA), and the test was performed as per the manufacturer’s specifications on a Bio-Rad PhD machine. Sera were tested starting at a dilution of 1:40 with phosphate-buffered saline (PBS), and if positive at further serial dilutions, the titre was assessed. The cut-off for ANA positivity using HEp-2 cells was 1:40, as recommended by Bio-Rad based on previous studies.19 Slides were read on a Nikon Fl microscope, and the pattern and titre were recorded.
The ML ANA assay was performed using ML sections obtained from Binding Site (San Diego, California, USA). Dilutions of sera were incubated with ML sections that had been fixed with acetone for 30 minutes at room temperature (generally 20°C), then washed with PBS for two 5 min washes and then incubated with fluorescein-tagged rabbit anti-human IgG (Binding Site) for 30 min at room temperature, and then the slides were washed with PBS for two 5 min washes. The cut-off for ANA positivity using ML was a titre of 1:20, as recommended by Binding Site. Both HEp-2 and ML ANA were also evaluated at a dilution of ≥1:80 as recommended by the ACR/EULAR criteria.16 Both HEp-2 and ML assays were reported as a titre and pattern. IFA patterns are linked to the corresponding AC-‘X’ nomenclature proposed by the International Consensus on Autoantibody Patterns (https://anapatterns.org/index.php).20 Patterns that were reported by the laboratory included speckled (AC-2/4/5/29), diffuse (AC-1), nucleolar (8/9/10), discrete speckled (AC-6/7), centromere (AC-3), peripheral (AC-11) and mixed patterns.
Anti-dsDNA, anti-Sm, anti-RNP, anti-Ro/SS-A and anti-La/SS-B assays were performed using kits (Bio-Rad enzyme immunoassay, Bio-Rad Laboratories) as per the manufacturer’s specifications. The cut-off for anti-dsDNA positivity was >25 EU/mL and anti-Sm, anti-RNP, anti-Ro/SS-A and anti-La/SS-B positivity was >20 EU/mL.
The quality assurance of both ANA tests and the autoantibody tests was monitored by subscription to the College of American Pathologists surveys.
Statistical analyses
Statistical analysis was performed using STATA V.15.1. We calculated the proportion of positive tests on each assay and the level of agreement using Cohen’s kappa (κ) for each ARD. Weighted κ was used for comparison of ANA patterns. A cut-off of 1:40 was used for HEp-2 ANA and 1:20 for ML. We also performed a sensitivity analysis using 1:80 as the cut-off for both assays.
We examined the intertest variability of ANA patterns and titres, where a high titre was defined as 1:640 or greater and low titre was between the positive cut-off and 1:320. Univariable and multivariable logistic regression analyses were used to determine whether age when test was performed, sex, race/ethnicity (white vs non-white) and specific autoantibodies (for patients with SLE only: anti-dsDNA, anti-La/SS-B, anti-RNP, anti-Sm and anti-Ro/SS-A) were predictors of HEp-2 positivity, ML positivity and assay agreement. A p value of less than 0.05 was considered statistically significant. We calculated ANA specificity and sensitivity independently and combined. For HEp-2, we also identified patients who had a HEp-2 test repeated on the same assay within 2 years of the baseline test. We recorded any tests that became positive after the second HEp-2 test and then recalculated the sensitivity. For patients who did not have a second test, we assumed that their initial test remained unchanged.
Results
Patients
We identified 961 patients for inclusion with concurrent HEp-2 and ML IFA (table 1). The patients had a mean age at the time of ANA testing of 60.4 years (SD 12.4 years); 90.4% were female; and 77.8% were white. Controls included patients with osteoarthritis, fibromyalgia, osteoporosis, Ehlers-Danlos syndrome, asthma, cancer, tendinitis and bursitis, without a history of an autoimmune disorder. Among the patients with SLE, 338 (80.9%) also had specific SLE antibody testing completed at the time of their ANA tests: 71 (21.0%) were anti-dsDNA positive; 62 (18.3%) were anti-La/SS-B positive; 72 (21.3%) were anti-RNP positive; 41 (12.1%) were anti-Sm positive; and 112 (33.1%) were anti-Ro/SS-A positive.
Intertest agreement for baseline ANA tests (n=961) using HEp-2 (cut-off≥1:40) and ML (cut-off≥1:20) for 961 patients with various autoimmune rheumatic diseases
Intertest variability for ANA IFA using HEp-2 and ML
The frequency of positivity using HEp-2 (titre of ≥1:40) was higher than ML (titre of ≥1:20) for all ARDs. In SLE, 78.0% of patients were ANA positive using HEp-2, and 60.8% were positive using ML. The intertest agreement of positivity/negativity was examined for ANA using HEp-2 and ML (table 1 and online supplemental table 1). The level of agreement between HEp-2 and ML for SLE was moderate (κ=0.48). DM/PM and APS had the strongest level of agreement with κ of 0.79 and 0.75, respectively, while SSc had the lowest level agreement (88.5% positive on HEp-2 vs 61.5% positive on ML) with a κ of 0.35. The agreement between HEp-2 and ML ANA from all diseases was moderate (κ=0.55).
Supplemental material
The sensitivity analysis using a cut-off of 1:80 (online supplemental table 2) also showed that the frequency of positivity using HEp-2 was higher than ML for all ARDs. The level of agreement between HEp-2 and ML for SLE was higher (κ=0.71) compared with the lower agreements at the cut-offs of 1:40 and 1:20, respectively. The agreement between HEp-2 and ML ANA using the higher cut-offs for all diseases was also higher (κ=0.69).
Predictors of HEp-2 and ML IFA ANA positivity and agreement
Multivariable analysis for HEp-2 or ML positivity revealed no significant predictors (age when test was performed, sex, race/ethnicity (white vs non-white) and specific SLE autoantibodies) (online supplemental tables 3 and 4). Patients with SLE who were anti-dsDNA positive were more likely to have agreement between HEp-2 and ML positivity (adjusted OR 6.27, 95% CI 1.45 to 27.20, p=0.01) (online supplemental table 5). There were no significant predictors of agreement in results between the two ANA assay substrates for the other ARDs.
Intertest variability for ANA titres and patterns using HEp-2 and ML
The agreement in ANA titres between HEp-2 and ML are presented in table 2. High-titre ANA was more frequent in HEp-2 ANA compared with ML ANA for all diseases. DM/PM and MCTD had the highest intertest agreement with κ=0.79 and κ=0.60, respectively. SLE had moderate agreement with a κ=0.59. There were 12 different types of ANA patterns, including mixed patterns, that were reported. The most common ANA patterns were AC-1 and AC-2/4/5/29 patterns for both HEp-2 and ML (table 3). Peripheral rim patterns (AC-11) were uncommon but were reported more frequently with ML (3.7%, 19/515) than with HEp-2 (0.78%, 5/637). Most of these peripheral rim patterns were seen in patients with SLE (n=17), and among them, 35.3% (6/17) were also positive for anti-dsDNA. There was moderate to high agreement in ANA patterns for all ARDs between HEp-2 and ML ANA.
Intertest agreement of high and low titres of baseline ANA tests between HEp-2 (cut-off≥1:40) and ML (cut-off≥1:20) for 961 patients
Intertest agreement of baseline ANA patterns between HEp-2 cells and ML for 961 patients
Sensitivity and specificity of ANA IFA on HEp-2 cells and ML
The sensitivity of the HEp-2 and ML IFA among different ARDs is shown in figure 1. In general, the sensitivity of ANA increased from ML as single test, HEp-2 as single test, combination of HEp-2 and ML, to repeating the same HEp-2 assay. The ANA IFA specificity for SLE was 60.8% on HEp-2 and 67.1% on ML.
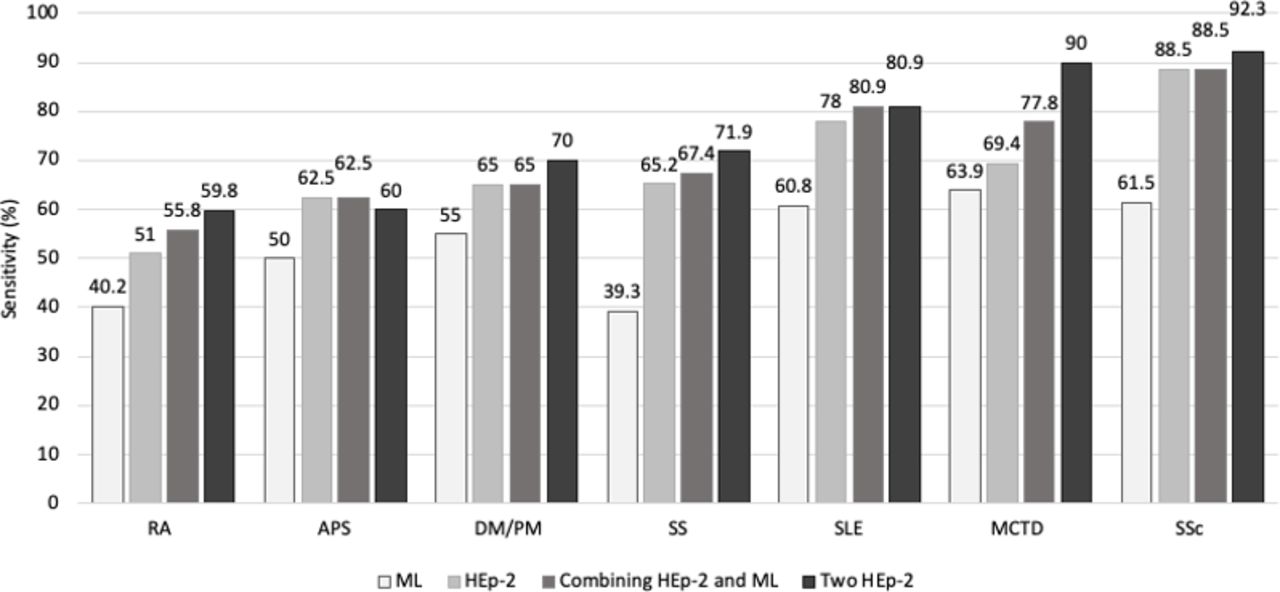
{kind=link}
Sensitivity of ANA on HEp-2 and ML as independent assays, HEp-2 and ML combined and repeating the HEp-2 assay. APS, antiphospholipid syndrome; DM/PM, dermatopolymyositis; HEp-2, human epithelial type 2; MCTD, mixed connective tissue disease; ML, mouse liver; RA, rheumatoid arthritis; SS, Sjögren’s syndrome; SSc, systemic sclerosis.
Discussion
In this study, we performed the largest comparison of HEp-2 and ML using over 1900 ANA tests for seven different ARDs to provide a historical context for the different substrates that have been used for diagnosis of ARDs. The transition for clinical laboratories from using mainly rodent tissue for ANA IFA to HEp-2 cells was based on the idea that a uniform cell line would be more dependable than using different rodent organs from different rodent strains.21 However, there are few papers that actually compared ANA performed on rodent substrate to HEp-2 IFA in small cohorts of a small number of diseases.7 9–14 We showed that there is only fair to moderate agreement with respect to positivity, titres and patterns of HEp-2 and ML in most ARDs. Furthermore, HEp-2 ANA was considerably more sensitive than ML IFA in most diseases, whereas the addition of ML IFA had just a modest incremental effect on the sensitivity already obtained with HEp-2 ANA.
In 1984, Molden et al7 studying sera with defined specificity concluded that HEp-2 was superior to mouse kidney in detecting antibodies to Ro/SS-A, Scl-70, PM-1 and the centromere pattern. Other studies with similar findings were published over the next decade, including Forslid et al,10 who studied 509 sera from healthy adults and children and noted that HEp-2 cells are more sensitive than rat liver sections for the detection of ANA. Hence, in 2000, an ACR committee concluded that HEp-2 was a more sensitive substrate than rodent tissue in detecting ANA at the same dilution and as better at detecting nucleolar patterns, anti-Ro/SS-A (rodent tissue has no immunoreactive Ro) or Ro52, and anticentromere antibodies.22 Some other advantages of HEp-2 over ML include being easier to standardise and to demonstrate commutability, patterns were easier to read because HEp-2 cell nuclei are larger, and it is less expensive to produce for high-throughput labs.13 In addition, ML contains only rare cells in metaphase and hence may miss mitotic patterns like proliferating cell nuclear antigen, nucleolar organising region 90, nuclear mitotic apparatus (NuMA), HSeg5 (NuMA2), RNA PolIII and some cytoplasmic patterns (endosomes, G (glycine) W (tryptophan)-containing bodies (GWB)/processing bodies, Golgi complex, rods and rings).
ANA titres were also thought to be higher on HEp-2 assays than those that used rat liver.9 In our study, we demonstrated that there were more patients with high-titre ANAs in HEp-2 compared with ML, which may account for the higher ANA sensitivity with HEp-2. On the other hand, some have argued that HEp-2 has a lower specificity than ML for SLE because it is inferior to rodent tissue at detecting peripheral rim patterns, which are often associated with the presence of anti-dsDNA, although this remains controversial.23 We showed that frequency of peripheral rim patterns was indeed reported more frequently with ML than with HEp-2.
The wide variability in ANA assay performance was noted by Pisetsky et al, who showed that the frequency of a negative ANA IFA varied from 5% to 23% on 103 sera from patients with SLE using three HEp-2 ANA kits from different companies and two solid-phase assays.24 In our study, we were limited to one manufacturer’s ANA HEp-2 kit, and this particular kit had the lowest frequency of negative ANA (5%) in Pisetsky et al’s study. In 2019, an ACR/EULAR committee SLE suggested that either a HEp-2 IFA or ‘an equivalent solid-phase assay’ can be used to facilitate the classification of SLE.16 At disease onset, over 6% of patients with SLE can be ANA negative as demonstrated in a large inception study of over 1100 patients with SLE.25 Due to the concern that some patients with SLE may screen negative with a single test, combined ANA assays such as a HEp-2 and solid-phase assay have been proposed as a potential solution.17 We did not show that combining HEp-2 with another IFA substrate, ML, substantially improved diagnostic yield.
In this study, ANA seroconversion (negative to positive) occurred even within 2 years of initial testing using the same assay. In 2002, an ACR committee suggested that due to a lack of evidence, ‘serial ANA testing is of unknown value’.26 ANA positivity may change with fluctuations in antibodies such as anti-dsDNA, which in turn correlate with disease activity,27 and it has also been established that autoantibodies start to be detectable and specificities accumulate prior to the onset of SLE.28 One retrospective cohort study of 36 715 ANA tests done in 28 840 patients found that 19% of patients with an initially negative ANA HEp-2 test had a positive result on at least one repeat test on the same ANA kit over a 7-year period (median time to first positive result 1.74 years).29 In addition, patients with SLE may lose ANA positivity with decreasing ANA titres over the disease course, as shown in a small prospective study of 54 recently diagnosed SLE cases followed up to 96 months.30 We recommend that future larger studies should longitudinally examine different ANA, autoantibodies and their assays to maximise the utility of diagnosis and monitoring of SLE and other ARDs.
The limitations of this study include the potential for diagnosis misclassification as we relied on ICD-9 and ICD-10 diagnostic codes and electronic medical record reviews. This could account for the lower frequency of ANA positivity among patients with SLE than reported in the literature.25 The reported percentage of HEp-2 IFA positives among patients with established SLE was lower than generally assumed but is in keeping with what has previously been shown in cross-sectional evaluations.31 32 We were also not able to obtain information on disease characteristics that could affect ANA test results, including disease duration, disease activity or severity, medications and specific autoantibody tests for all ARDs. Since we did not have a cohort of healthy blood donors, a potential bias is that controls were selected on the basis that they had an ANA test ordered by their physician because of symptoms of ARDs. These patients may potentially be at higher risk of developing ARD or already have an ARD that has not been diagnosed. It may also explain why their prevalence of ANA positivity (39.2% on HEp-2% and 32.9% on ML) at ≥1:40 was slightly higher than what has been reported by prior studies (32%) at this dilution.19 We performed a sensitivity analysis (online supplemental table 2) that showed that at a higher dilution (≥1:80), fewer controls were HEp-2 (12.7%) and ML (11.4%) ANA positive. Also, we may have underestimated the change in sensitivity of repeating HEp-2 assay as only a small subset of patients had a repeated HEp-2 test.
In conclusion, the present study of historical and previously unanalysed data demonstrated fair to moderate agreement between HEp-2 and ML ANA IFA and that performing a combined IFA test only has modest incremental impact on sensitivity compared with HEp-2 alone in the diagnosis of SLE and other ARDs. Indeed, repeating the same HEp-2 ANA test within 2 years had the highest ANA sensitivity. These are important considerations under the new ACR/EULAR classification criteria16 and argue for future studies to examine the changes in ANA and autoantibodies over the disease course and for better tests for the diagnosis of ARDs.
Acknowledgments
The authors thank all the technicians in the laboratories who performed the assays.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to this manuscript and approved the final version.
Funding MYC has received research grants from the Lupus Foundation of America Gary S. Gilkeson Career Development Award; JC has received research grants from NIAMS P30-AR072577(VERITY); KC has received research grants from NIH (K24 AR066109); there are no other relationships or activities that could appear to have influenced the submitted work.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Partners Ethics Institutional Review Board approved all aspects of this study (protocol number 1999P001152). They determined that, as a retrospective database study, this project met criteria for exempt status; therefore, informed consent was waived.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. No additional text.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.