Article Text

Abstract
Objective SLE is a chronic multisystem autoimmune inflammatory disease impacting a number of organs, including the central nervous system (CNS). The pathophysiology of CNS lupus is multifactorial, making diagnosis problematic. Neurocognitive (NC) testing and specific biomarkers to identify the development of neuropsychiatric (NP) symptoms in lupus are needed. Paediatric patients with SLE have high incidence of NP disease . While serum anti-N-methyl-D-aspartate receptor (NMDAR) antibodies have shown promise as a biomarker of NP in adults with SLE, much less is known with regard to paediatric patients with SLE.
Methods We performed a cross-sectional study in paediatric patients with SLE. Serum NMDAR antibodies were measured and compared with levels in patients with juvenile idiopathic arthritis (JIA). Formal NC testing was performed in accordance with the Childhood Arthritis & Rheumatology Research Alliance neuropsychological core test battery. NC functioning was compared in the two groups and with NMDAR antibody levels.
Results Serum NMDAR antibody levels were significantly higher in paediatric patients with SLE compared with patients with JIA. There were no significant correlations between NMDAR antibody levels and any measure of NC functioning. In an exploratory examination of anti-ribosomal P (RibP) antibody and NC functioning in a subset of patients with SLE, RibP antibody-positive patients exhibited worse scores for Verbal Memory Index and Design Fluency Test Switching compared with RibP antibody-negative patients. A globally significant association between disease status and NC functioning was observed. Specifically, patients with SLE had lower scores compared with patients with JIA for full-scale IQ, letter–word recognition, reading fluency and calculation skills after adjusting for multiple comparisons.
Conclusion These collective results suggest that although serum NMDAR may serve as a biomarker, formal NC testing is superior in identifying paediatric patients with SLE with NP manifestations. RibP also may potentially serve as a biomarker of NP manifestations in paediatric patients with SLE. Additional and longitudinal studies are needed.
- lupus erythematosus
- systemic
- autoantibodies
- autoimmunity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Neurocognitive dysfunction is prevalent in childhood-onset lupus.
What does this study add?
The diagnosis of neuropsychiatric syndromes in SLE remains difficult, and this study highlights the significant difficulties that scientists continue to face when studying the effects of lupus on the central nervous system (CNS).
A single biomarker such as N-methyl-D-aspartate receptor or anti-ribosomal P antibodies is not adequate to make a diagnosis of CNS lupus.
How might this impact on clinical practice or future developments?
A multicentre approach with a large sample size and the development of a biomarker panel associated with innovative neuroimaging will be necessary to better understand the neuropsychiatric syndromes in SLE and improve the diagnosis of CNS lupus.
Introduction
SLE is a complex, chronic multisystem autoimmune inflammatory disease that targets predominantly young women. Disease course varies from patient to patient impacting many organs, including skin, heart, kidney and brain, and is complicated by acute disease exacerbations. Central nervous system (CNS) involvement with neuropsychiatric (NP) symptoms are common in patients with SLE.1 2 Approximately 21%–47% of patients with SLE show recurrence or onset of new NP syndromes, and 10% die of SLE-related CNS involvement.3 CNS involvement was the major factor contributing to mortality in cohorts where 5% of patients die during the first 5 years after SLE diagnosis4 and a major cause of morbidity and mortality in SLE.5 The signs and symptoms of lupus in the nervous system are diverse and include: encephalopathies, headaches, mood disorders, psychosis, movement disorders, stroke, neurovascular diseases, myelopathies, cranial neuropathies, peripheral neuropathies, myasthenia gravis and neurocognitive dysfunction (NCD). Both neurological and psychiatric abnormalities appear in forms that may be subtle, but sufficient to change a person’s lifestyle and lead to disability.4
In order to identify patients with SLE with NCD, the American College of Rheumatology (ACR) recommends a standard battery of tests for use in individuals with SLE6 (ACR 1999). This led to the use of formal neurocognitive (NC) testing as the gold standard when measuring cognitive functions in SLE. Almost all studies use a standardised battery of traditional psychometric tests when measuring NC functioning in SLE. These tests assess the validity of other tools thought to be useful in measuring NC functioning in SLE. Although the use of formal NC testing is useful in identifying patients at risk of CNS disease, there are significant drawbacks in using traditional testing in clinical practice. For instance, the tests require specialised training to administer and the battery can be time consuming and cost prohibitive. A meta-analysis of neuropsychological testing methods reinforced the necessity for establishing effective diagnostic metrics for identifying patients with NCD.2 Identifying biomarkers specific for detecting patients at risk of CNS manifestations of lupus is of utmost importance and would help physicians identify patients at risk.
The pathogenesis of NCD remains somewhat elusive and is likely multifactorial, including autoantibody production specific for brain structures, immune complex deposition, microangiopathy and intrathecal production of proinflammatory cytokines. Many studies investigated a potential association between specific autoantibodies and NP syndromes. Most notably, antibodies to the N-methyl-D-aspartate receptors (NMDARs).7–24 NMDARs, consisting of subunit 1 and subunit 2 (NR2), are important for excitatory synaptic transmission as a fundamental mechanism of synaptic plasticity underlying learning and memory. Under physiological conditions, NMDAR NR2 is expressed on neurons throughout the hippocampus and cortex, and binds the neurotransmitter glutamate. Anti-NR2 antibodies are a subset of pathogenic murine anti-dsDNA antibodies that cross-react with a consensus peptide sequence of the extracellular, ligand-binding domain of mouse and human NR2a and NR2b.25
In healthy mice, introduction of cerebral spinal fluid (CSF) or serum containing anti-NMDAR NR2 antibodies directly into the CNS intravenously or induction of anti-NMDAR antibodies caused neuronal death, specifically hippocampal damage, and led to impaired spatial memory.20 25–28 These data suggest anti-NMDAR antibodies may be associated with various manifestations of NP lupus, including cognitive dysfunction. In adults, many studies investigating a potential association of serum anti-NMDAR antibodies in patients with NP manifestations of SLE reported mixed results. Several studies demonstrated elevated levels of serum anti-NMDAR antibodies in patients with SLE compared with controls.7 8 12 14 16 20 However, studies comparing patients with SLE diagnosed without or with NP symptoms failed to observe a significant difference in serum anti-NMDAR antibody levels between the two groups.12–14 29 Of those studies that included formal NC testing, a few reported significant associations of anti-NMDAR antibodies with deficits in specific domains or with depressive symptoms,7 11 20 23 while others reported no associations.9 10 Collectively, these results suggest serum anti-NMDAR is unlikely to serve as a useful biomarker for adults with NP syndromes.
Up to 20% of patients with SLE receive a diagnosis during childhood.30 31 Paediatric patients with SLE show more severe organ involvement and a more persistently active disease course compared with adults.32–35 Notably, there is a high incidence of NP disease in paediatric patients with SLE.36 Few studies have included paediatric patients with SLE; hence, a potential association of anti-NMDAR antibodies with NCD specifically in paediatric patients with SLE is unclear. To our knowledge, only one study focused on NP symptoms in lupus in children to investigate a potential association of serum autoantibody measures with NCD. This was a longitudinal study of paediatric patients with SLE that reported ~16% of their cohort exhibited NCD and serum anti-NMDAR antibody levels failed to distinguish between paediatric patients with SLE without and with NCD.19 However, serum anti-NMDAR antibody levels were elevated in patients exhibiting NC decline at follow-up. In this cross-sectional study, we measured serum levels of anti-NMDAR and performed formal NC testing in paediatric patients with SLE and patients with juvenile idiopathic arthritis (JIA) to determine if anti-NMDAR, as well as anti-ribosomal P (RibP), antibodies may serve as biomarkers of CNS manifestations.
Methods
Study design and population
This was a cross-sectional study approved by the local Institutional Review Board. Twenty-four patients diagnosed with SLE, and 12 patients with JIA as a comparison group, were included. Children diagnosed according to the ACR Classification Criteria with SLE (paediatric patients with SLE) prior to the age of 18 years were recruited from an outpatient paediatric rheumatology clinic. A cross-sectional representative sample of patients with JIA (any subtype) matched ±2 years of age of paediatric patients with SLE was included. To be included in the study, participants had to lack a diagnosis of pre-existing disease other than SLE or JIA that might affect cognitive functioning. Patients with SLE diagnosed with prior CNS lupus were not excluded. Patients with JIA who had a parent diagnosed with SLE were not excluded. The medical records of the participants were reviewed for age at the time of the study, race and sex. Clinical disease measures available, including anti-dsDNA antibodies, C3 and C4, as well as disease duration, were obtained from clinic records for the paediatric participants with SLE. Only paediatric patients with SLE suspected of having CNS involvement had RibP antibodies measured. Although prednisone was prescribed for most of the patients with SLE at some point during the course of illness, medication usage was not readily available for all patients with SLE and JIA. SLE Disease Activity Index disease activity scores were calculated and presence of CNS lupus was determined by the treating physician. Patients with dsDNA antibodies >30 IU/mL or RibP antibodies >0.9 were considered positive for those antibodies. Patient demographics and clinical disease measures/assessments available are provided in table 1.
Participant demographics by disease type
Formal NC testing
A battery of NC measures was selected in accordance with the Childhood Arthritis & Rheumatology Research Alliance neuropsychological core test battery.37 Specifically, an estimate of intellectual functioning (Full Scale IQ, FSIQ) was obtained with a two-subtest battery of the Wechsler Abbreviated Scale of Intelligence (WASI),38 including Vocabulary and Matrix Reasoning. Assessment of working memory (Working Memory Index, WMI) and processing speed (Processing Speed Index) was obtained using subtests of the Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV)39 for patients aged 6–16 years or the Wechsler Adult Intelligence Scale, Fourth Edition (WAIS-IV)40 for patients aged over 16 years of age. The Digit Span and Letter–Number Sequencing subtests of the WISC-IV and the WAIS-IV combine to form a Working Memory Composite. The Coding and Symbol Search subtests of the WISC-IV and the WAIS-IV combine to form the Processing Speed Composite. These four subtests are equivalent in the WISC-IV and WAIS-IV, so that the respective subtests and composite scores are comparable for the WISC-IV and the WAIS-IV. Composite scores were used in the statistical analyses. Memory was assessed with the Wide Range Assessment of Memory and Learning, Second Edition (WRAML-2).41 The Story Memory and Verbal Learning Memory subtests were administered to assess auditory/verbal memory and the Design Memory and Picture Memory subtests were administered to assess visual memory. Visual attention and speed of response were assessed via the Conners’ Continuous Performance Test, Second Edition (CPT-II)42 (continuous response test (cpt) for reaction time (cptRT), omission errors (cptOM) or commission errors (cptCOM)), a 15-minute computerised task in which examinees must signal when target alphabet letters appear within a sequence of target and non-target letters. Fine motor control and speed were assessed with the Grooved Pegboard Test (2002). Fine motor dexterity for the preferred and non-preferred hand was assessed. Executive functions were assessed with the Delis-Kaplan Executive Function System (D-KEFS).43 The Verbal Fluency Test and the Design Fluency Test assess verbal and visual fluency, respectively, as well as cognitive flexibility. The Color–Word Interference Test assessed the ability to shift cognitive sets and response inhibition. Finally, select subtests of the Woodcock-Johnson Tests of Achievement, Third Edition (WJ-III)44 assessed single-word reading skills (letter–word identification), speed and accuracy of reading (reading fluency), numerical math calculation skills (calculation), and speed and accuracy of mathematical calculation (math fluency). The NC battery of tests was administered to all study participants beginning at 08:00 in the following order during one testing session: WASI, WISC-IV/WAIS, WRAML-2, D-KEFS, Grooved Pegboard Test, WJ-III and CPT-II. Breaks from testing were provided as needed. The results of NC testing are reported as standard scores, the metric used by test developers to report performance for the NC measures in this battery. Standard scores enable comparisons across measures and between participants, and have a mean of 100 and an SD of 15.
NMDAR antibody measures
NMDAR-NR2 subunit antibody testing was measured in patient serum by ELISA essentially as previously described.45 Briefly, wells on 96-well plates were coated with NMDAR peptide DWEYSVWLSN acetylated on the N-terminus (AnaSpec, Fremont, California, USA) diluted to 15 μg/mL in 0.1M NaHCO3 then blocked with 1% bovine serum albumin (BSA) in phosphate-buffered saline (PBS). Serum samples were diluted with 0.2% BSA in PBS and incubated with the peptide for 1 hour at 37°C. Wells were washed, incubated with a secondary antibody conjugated to alkaline phosphatase, washed and incubated with phosphatase substrate. Reactions were developed at 37°C for 45 min and OD was read at 405 nm. Samples were run at least two times independently using dilutions of 1:100–1:800 to ensure specificity and reproducibility. SLE and JIA samples were run deidentified (blinded to the individual performing the assay) and randomly assigned to a plate. Human monoclonal antibodies B1, which is not reactive with NMDAR, and G11, which is reactive to NMDAR, were kind gifts from Dr Betty Diamond and used as negative and positive controls, respectively.46 Final OD values presented are from the 1:100 dilutions normalised to the OD of the positive control antibody G11 on each plate to adjust for plate to plate variations.
Statistical analyses
Descriptive statistics were calculated for all study participants by disease status. Differences in patient characteristics by disease status were examined using Fisher’s exact test for categorical variables and a two-sample t-test or Wilcoxon rank-sum test, when appropriate, for continuous characteristics. The primary goal was to examine the association between anti-NMDAR antibody levels with NC functioning in this paediatric rheumatology population. Associations between measures of NC functioning and anti-NMDAR antibody across all patients were evaluated initially using a multivariate regression approach with the 15 measures of cognitive function as correlated dependent variables and anti-NMDAR antibody level as the independent variable. The model included disease status, anti-NMDAR antibody level and the interaction between them as dependent variables. Ten subjects per variable in the models are necessary for valid statistical inference47; thus, although additional patient characteristics may impact cognitive function, only these three variables were considered. The 95% CIs for the correlation between anti-NMDAR antibody levels and each measure of cognitive function by disease status were estimated using the Fisher’s Z transformation.
A secondary goal of the study included evaluation of differences in NC functioning by disease status using a multivariate regression approach with the 15 measures of NC functioning as correlated dependent variables and disease status as the independent variable. Given a significant global Wilk’s lambda for the association between NC functioning and disease status, differences in each measure of NC functioning by disease status were examined to identify where differences exist. Due to limited sample size, we considered both unadjusted and adjusted p values for individual tests of association between each measure of NC functioning with disease status. We also conducted an exploratory examination of differences in NC functioning by RibP antibody status (positive/negative) among paediatric patients with SLE; however, due to limited sample size, no formal hypothesis testing was conducted. All analyses were performed in SAS V.9.4 and R V.4.0.
Results
Correlation between NMDAR antibody level and NC functioning
The study population included 24 patients with juvenile onset SLE and 12 patients with JIA. Patients with JIA were chosen as a comparator group since they were also coping with a chronic disease and taking medications that suppress the immune system. The population was predominantly female (77.8%) and 45.7% of the participants were white. Only one subject was reported to have CNS involvement, which was diagnosed as acute psychosis and was inactive at the time of testing. Patient demographics and characteristics by disease status are shown in table 1. Patients with SLE had a higher median NMDAR antibody level compared with children with JIA (figure 1A, p=0.026). Seven of the 24 patients with SLE had levels higher than the mean plus two SDs of the JIA group, emphasising the significance of the elevated NMDAR antibody levels in those subjects. In the multivariate regression model including disease status, NMDAR antibody level, and the interaction between status and NMDAR level, disease status showed global significance with p<0.05 and the interaction was significant at p<0.1 (disease status: Wilk’s Λ=0.288, F14,16=2.82, p=0.025; NMDAR: Wilk’s Λ=0.410, F14,16=1.66, p=0.165; interaction: Wilk’s Λ=0.357, F14,16=0.357, p=0.087). Evaluation of the correlation between NMDAR antibody level with the different measures of NC functioning by disease status found a significant positive correlation between NMDAR antibody levels and processing speed in children with JIA (unadjusted p=0.017). However, after adjusting for multiple comparisons, no significant associations were noted. Figure 1B shows the estimated Spearman rank correlation and 95% CI for the correlation between NMDAR antibody levels with the 15 measures of NC functioning across all patients (black), and for patients with SLE (green) or JIA (red).
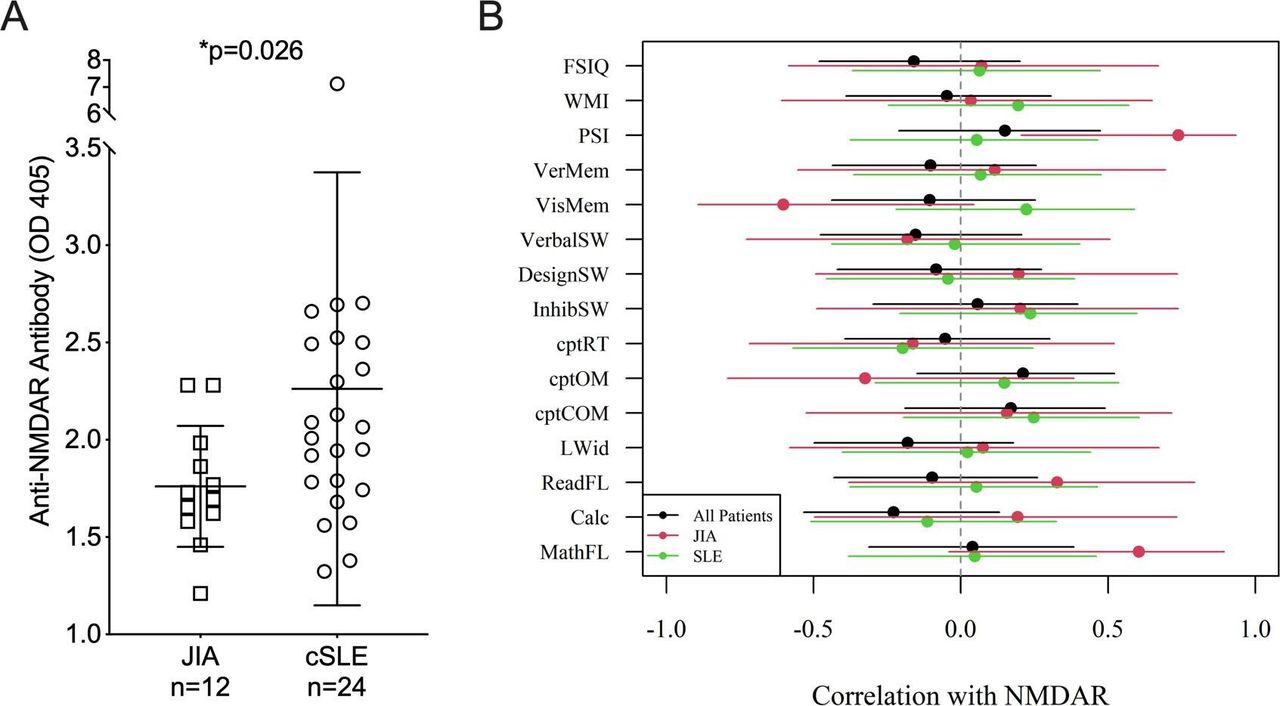
Anti-NMDAR antibody levels are significantly higher but are not associated with any measures of cognitive function in paediatric patients with SLE compared with patients with JIA. (A) Serum NMDAR antibodies were measured in paediatric patients with SLE and patients with JIA by ELISA. Means+SD are presented graphically. Adjusted p value is provided on the graph. (B) Cognitive function was assessed for correlation with NMDAR antibody levels as described in the Materials and Methods sections. Scores for the 15 individual cognitive tests listed in table 2 were evaluated for correlation with NMDAR antibody levels for all patients (black), patients with JIA only (red) or paediatric patients with SLE only (green). Calc, calculation; cptCOM, continuous response test for commission errors; cptOM, continuous response test for omission errors; cptRT, continuous response test for reaction time; cSLE, children with SLE (paediatric patients with SLE); DesignSW, Design Fluency Test; FSIQ, Full Scale IQ; InhibSW, Color–Word Interference Test; JIA, juvenile idiopathic arthritis; LWid, Letter–Word Identification; MathFL, math fluency; NMDAR, N-methyl-D-aspartate receptor; PSI, Processing Speed Index; ReadFL, reading fluency; VerbalSW, Verbal Fluency Test; VerMem, auditory/verbal memory; VisMem, visual memory; WMI, Working Memory Index.
NC functioning and disease status
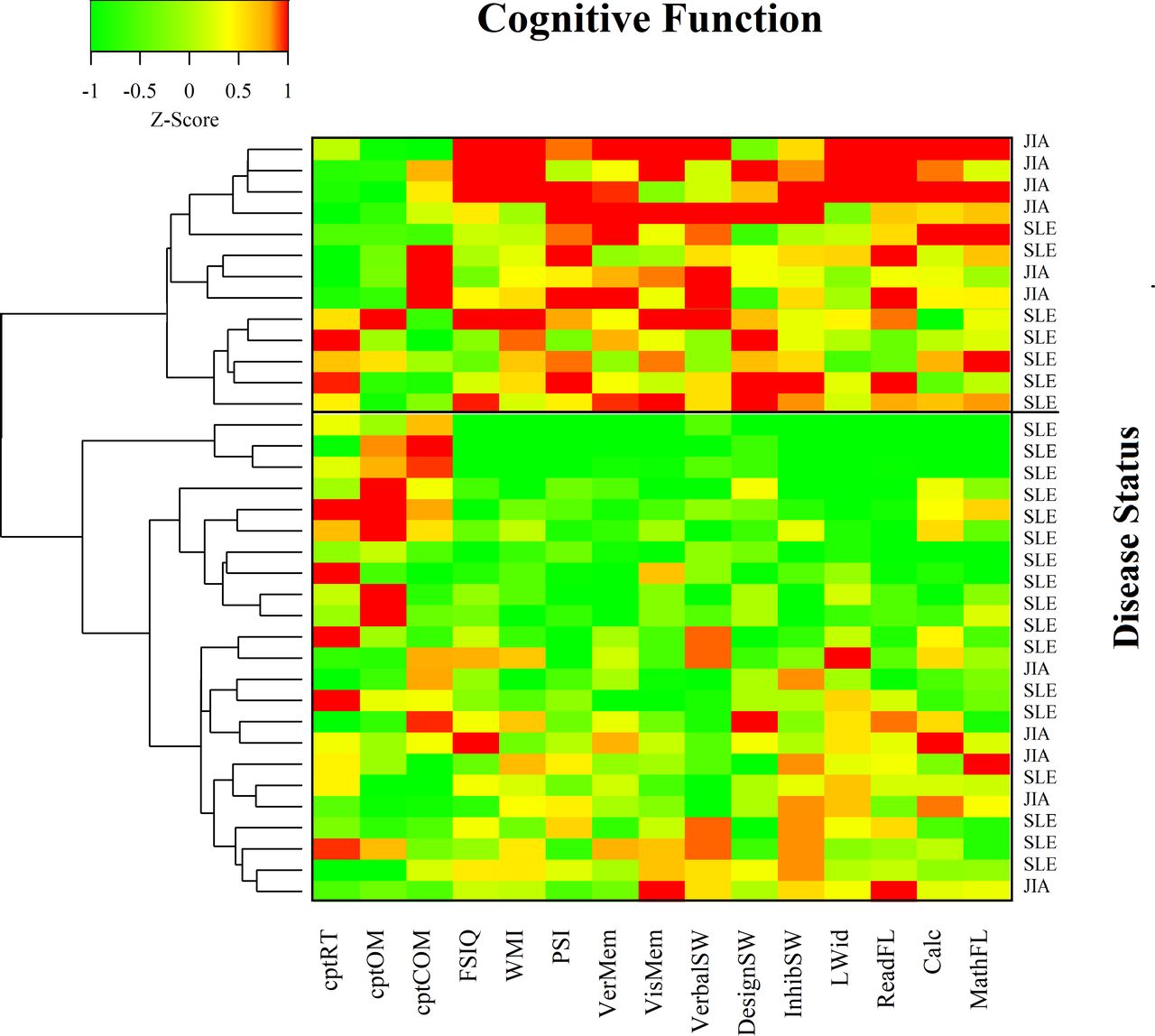
The association between disease status with NC functioning was examined. The multivariable model of NC functioning regressed on disease status yielded a globally significant association (Wilk’s Λ=0.316, F14,21=3.24, p=0.008). Thus, associations of each measure of NC function with disease status were examined. Differences in NC performance by disease status are shown in table 2. Before adjusting for multiple comparisons, there was a significant association between disease status with FSIQ, WMI, Verbal Memory Index, Color–Word Inference Test, omissions, letter–word recognition, reading fluency and calculation skills. Specifically, patients with SLE had lower scores for FSIQ, WMI, Verbal Memory Index, Color–Word Inference Test, letter–word recognition, reading fluency and calculation skills, and a higher score for omissions relative to patients with JIA. FSIQ, letter–word recognition, reading fluency and calculation skills retained significance even after adjusting for multiple comparisons. A heat map demonstrates clustering of patients by the 15 measures of NC functioning, with patient disease status shown beside each row in the heat map (figure 2).

{kind=link}
{kind=link}
Heat map of standardised cognitive test performance using hierarchical clustering. Green indicates values below the mean observed values and red indicates values higher than the observed mean values. The two largest clusters of patients are indicated by the black box in the diagram and patient disease status is reported to the right of the heat map. Calc, calculation; cptCOM, continuous response test for commission errors; cptOM, continuous response test for omission errors; cptRT, continuous response test for reaction time; DesignSW, Design Fluency Test; FSIQ, Full Scale IQ; InhibSW, Color–Word Interference Test; JIA, juvenile idiopathic arthritis; LWid, Letter–Word Identification; MathFL, math fluency; PSI, Processing Speed Index; ReadFL, reading fluency; VerbalSW, Verbal Fluency Test; VerMem, auditory/verbal memory; VisMem, visual memory; WMI, Working Memory Index.
Cognitive test performance by disease type reported as standard scores (mean±SD)
Exploratory examination of anti-RibP antibody status and NC function
Serum RibP antibody status was evaluated in 16 of the 24 paediatric patients with SLE by the treating physician when CNS involvement was suspected. Four of those 16 patients were positive for RibP antibodies. Mean NC performance for each of the metrics by RibP antibody status is reported in table 3. Although no formal hypothesis testing was conducted, the average performance for RibP antibody-positive patients was worse on a majority of the NC tests. RibP antibody-positive patients exhibited the largest difference for the Verbal Memory Index and the Design Fluency Test Switching showing a greater than 10% lower average score compared with RibP antibody-negative patients. There were no other notable patterns in NC performance by anti-dsDNA antibody status, lupus nephritis status, duration of disease, C3 or C4. In the heat map, red represents scores that are greater than the mean and green represents values lower than the mean within each cognitive performance metric. Higher scores indicate better performance for all measures except cptRT, cptOM and cptCOM for which lower scores are better. The heat map suggests there is a cluster of 13 patients with strong cognitive performance on all or a majority of tasks, and a second cluster of 23 patients that shows more modest cognitive performance. Fifty-four per cent (7 of 13) of the patients in the cluster with stronger cognitive performance are patients with SLE compared with 74% (17 of 23) of the patients in the cluster with more modest performance.
Cognitive test performance by RibP positivity reported as standard scores (mean±SD)
Discussion
NCD in SLE is difficult to diagnose due to often subtle symptoms requiring formal NC testing. Formal neuropsychological testing as noted in our study remains the gold standard. However, the tests require specialised training to administer. The battery can be time consuming and cost prohibitive. Traditional testing is sensitive to patient fatigue, patients have exhibited practice effects on repeated testing, and traditional testing is limited in detecting subtle impairment.48–50 There has been considerable work focused on alternatives to the use of formal NC testing including the Automated Neuropsychological Assessment Metrics (ANAM) for which there is now a paediatric version.51 However, finding a biomarker that is specific for detecting patients at risk of the CNS manifestations of lupus is of utmost importance and would help the physician in clinical practice to identify those patients at risk.
In this study, we compared paediatric patients with SLE with age-matched patients with another autoimmune disease JIA, which is not known to be associated with NC impairment.52 Serum NMDAR antibody levels were significantly higher in paediatric patients with SLE compared with patients with JIA in our cohort. These results are similar to those observed in previous studies of adult patients with SLE (diagnosed without or with NP manifestations/NCD) as compared with healthy controls.7 8 12 14 16 Gono et al16 also showed significant differences in NMDAR antibody levels in patients with SLE compared with patients with either rheumatoid arthritis or systemic sclerosis. The only other study of which we are aware that specifically focused on paediatric patients with SLE compared NMDAR antibody levels among patients and did not include controls.19 Although there has been variability among the percentage of patients testing positive (~25%–44%) depending on the cohort and method of determining positivity, serum NMDAR antibodies are clearly present in many patients with SLE.
Results of NC testing in our cross-sectional study participants showed patients with JIA significantly outperformed paediatric patients with SLE in the domains of intellectual functioning, auditory working memory, single-word reading skills and math calculation skills. There were trends toward significant group differences in verbal memory, inattention and reading fluency. Our study observed similar deficits in paediatric patients with SLE as in a previous study.53 Specifically, participants with NC dysfunction demonstrated deficits in math calculation skills and reaction time on a continuous performance test. Although NMDAR antibodies were elevated on average in the paediatric patients with SLE group in our study, these levels did not differentiate between paediatric patients with SLE identified to have NC deficits and those without. Serum NMDAR levels also were not significantly correlated with global NC decline. However, we observed a significant inverse correlation between NMDAR antibody levels and the CPT-II reaction time among all participants (both paediatric patients with SLE and patients with JIA). Thus, formal NC testing was better at detecting group differences than serum NMDAR antibody levels. In general, the large number of studies in this area largely supports this conclusion. Of those studies that included formal NC testing,7 9–11 20 only two studies reported correlations between serum NMDAR and specific domains of NC dysfunction,7 20 all in adult patients. More informal NC testing was performed in two studies21 22 with one reporting a correlation between NMDAR antibodies and specific domains of NC dysfunction.21
Several mouse studies demonstrated NMDAR antibodies cause neuronal injury or NC impairment only when they have direct access to the brain (ie, blood–brain barrier breach).20 25–28 Hippocampal atrophy was demonstrated in the brains of patients with SLE or primary Sjogren’s syndrome who were positive for NMDAR antibodies in their CSF compared with patients who were negative for NMDAR antibodies.18 Several studies demonstrated antibodies in the CSF were significantly elevated in patients with SLE with NP symptoms compared with patients without NP symptoms,14 17 29 or were associated with diffuse CNS disease among patients with SLE.14 29 Hirohata et al observed that NMDAR antibodies in CSF correlated with severity of NP syndromes in SLE.17 Together these studies suggest that while NMDAR antibody levels in the serum are present in many patients with SLE, the levels in CSF are more likely to distinguish between patients without and with NC impairment. Repeated collections of CSF to monitor for development of NP are not ideal, especially in children. If circulating NMDAR antibodies are playing a causative role in the development of NP manifestations in SLE once they breach the blood–brain barrier, damage may have already occurred by the time they are detected in the CSF. Results from a mouse study demonstrated NC changes occurred after the antibodies were no longer detectable.20 Thus, circulating NMDAR antibodies may serve as a potential biomarker to predict which patients may eventually develop NP manifestations.
In addition to NMDAR antibodies, we also assessed potential associations of RibP antibodies with NCD in the subset of paediatric patients with SLE suspected to have CNS involvement. RibP antibodies recognise different ribosomal proteins and are thought to play a role in the pathogenesis of NP symptoms in SLE by impairing neuronal function or inducing apoptosis in neurons. As with NMDAR antibody studies, an association of RibP antibodies with neuropsychological manifestations in patients with lupus has not been consistently demonstrated and we identified only two studies in which RibP antibodies were measured in paediatric patients with SLE with NP symptoms.19 54 In both paediatric studies, serum RibP antibodies were more common in patients with, compared with patients without, NP symptoms. These antibodies were negatively associated with working memory, psychomotor speed and visuoconstructional ability,19 or shown to have potential predictive value for patients with SLE with NCD.54 Our study showed that RibP antibody-positive patients performed worse on many of the NC tests compared with antibody-negative patients. However, due to the small sample size, we were unable to determine if this association was significant. While individually NMDAR and RibP antibodies show promise as potential serum biomarkers, a panel of serum autoantibodies may serve as a more specific and accurate means of identifying patients who have, or are at risk of, developing NP manifestations or NCD. In a previous study analysing paediatric patients with SLE,19 the levels of five autoantibodies, including NMDAR and RibP antibodies, were measured in sera with respect to NCD using a battery of tests similar to our study. Although no differences in the levels of any one individual antibody showed significant predictive or diagnostic value, the five autoantibodies together accurately predicted and identified patients with NC impairment in their paediatric patients with SLE cohort.
The results of our study should be interpreted within the context of several study limitations. The most significant limitation in our study was sample size. Many variables such as socioeconomic status and education, which we did not collect on these patients, in addition to clinical disease parameters (disease activity, medication use and so on) may impact cognition. Another limitation is the cross-sectional design. Thus, a longitudinal study with a large number of patients would better determine if specific biomarkers in the sera can identify patients with NCD or other NP syndromes, or even to predict which patients have the potential for developing NP syndromes if the blood–brain barrier is damaged or compromised. Although we chose patients with JIA as a comparator group because they are of similar age as the paediatric patients with SLE group and also coping with a chronic disease, there are some limitations to choosing this group. Patients with JIA may also have NCD in the form of anxiety and depression due to disease status or effects of medication usage.
Perhaps the most important outcome of this study and others like it, is that it highlights the significant difficulties that scientists continue to face when studying the effects of lupus on the CNS. Our observations in this study demonstrate the NCD is prevalent in paediatric patients with SLE. Clinicians who take care of patients with lupus know the diagnosis of NP syndromes in lupus is tremendously difficult for many reasons. Many times, imaging studies and laboratory tests are normal even in the context of significant disease. Our observations in this study demonstrate that NCD is prevalent in paediatric patients with SLE; however, a single biomarker such as NMDAR or anti-RibP antibodies will not likely be informative to make a diagnosis of CNS lupus. In order to truly discover a biomarker for NP syndromes in lupus, a multicentre approach with a large sample and the development of a biomarker panel will be necessary. This will allow a model to include the many variables that can affect cognition. Furthermore, patients will need to be followed prospectively over time and analysed at numerous time points. These time points will need to include neuroimaging, biomarker studies on both blood and CSF, as well as NC testing using either formal NC testing methods or an automated test such as the paediatric ANAM. As authors, we realise the significant limitations of this study yet we feel this investigation demonstrates the importance of a multicentre collaboration. As a scientific community, we will not obtain robust results unless we have a large sample size. This study also supports the importance of continued research and discovery in this field since CNS lupus remains the second leading cause of morbidity and mortality in paediatric patients with SLE.
Conclusions
The disease pathogenesis of CNS lupus in children remains poorly understood and yet can have devastating consequences. This study, like many others, demonstrates the need for good biomarkers of CNS lupus, which remains a challenge and emphasises further research is needed. Advances in neuroimaging55 are also important to assess disease in a non-invasive way, and the paediatric ANAM shows promise in following a patient’s NC function over time. However, we still do not have an accurate way to diagnose this disease. Due to the complexity of the pathophysiology of CNS lupus, the identification of a single biomarker or the utilisation of a single test is impractical. A combination of clinical parameters, neuroimaging data, and a biomarker panel to accurately diagnose CNS lupus and monitor the disease over time will likely be required.
Acknowledgments
The authors thank Dr Betty Diamond for the human monoclonal antibodies B1 and G11.
References
Footnotes
Contributors NMR, TKN and GG contributed to study design, data collection, interpretation of results and preparation of the manuscript. MK contributed to data collection, interpretation of results and preparation of the manuscript. BW contributed to interpretation of results and preparation of the manuscript.
Funding NMR is a recipient of a Building Interdisciplinary Research Careers in Women’s Health (BIRCWH) K12 career development program co-funded by the Office of Research on Women’s Health (ORWH) and the National Institute of Child Health and Human Development (NIHCD) of the National Institutes of Health (NIH). Additional support for this project was provided in part by the National Center for Advancing Translational Sciences of the NIH under grant number UL1 TR001450, and by the Core Center for Clinical Research, Improving Minority Health in Rheumatic Diseases (CCCR) at MUSC through NIH grant number P30 AR072582-01.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Institutional Review Board, Medical University of South Carolina.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplemental information.