Article Text

Abstract
Objective To report the results of a survey exploring the experience of patients with SLE facing hydroxychloroquine (HCQ) shortage that occurred during the early phases of the COVID-19 pandemic.
Methods A survey was designed by Lupus Europe’s patient advisory network and distributed through its social media, newsflash and members' network. People with lupus were asked about their last HCQ purchases and their level of anxiety (on a 0–10 scale) with regard to not being able to have access to HCQ, once in April 2020 (first wave) and after 11 August (second wave). The results were compared.
Results 2075 patients responded during the first wave; 1001 (48.2%) could get HCQ from the first place they asked, 230 (11.1%) could get the drug by going to more than one pharmacy, 498 (24.0%) obtained HCQ later from their usual pharmacy and 126 (6.1%) from other sources. 188 (9.1%) could not get any; 32 (1.5%) did not respond to this question. All countries showed significant improvement in HCQ availability during the second wave. 562 (27.4%) patients reported an extremely high level of anxiety in wave 1 and 162 (10.3%) patients in wave 2; 589 (28.7%) and 268 (17.1%) patients reported a high level of anxiety in wave 1 and wave 2, respectively.
Conclusions The HCQ shortage had a significant impact on patients with SLE and has been responsible for psychological consequences including anxiety. Indeed, despite an objective improvement in drug availability, the event is leaving significant traces in patients’ mind and behaviours.
- systemic lupus erythematosus
- lupus erythematosus
- systemic
- psychology
Data availability statement
Data are available upon reasonable request. Data from the survey can be made available for research purposes. Request should be made to the board of Lupus Europe by email to secretariat@lupus-europe.org.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
It is already known that speculations on the effect of hydroxychloroquine (HCQ) on COVID-19 led to its shortages at the beginning of the pandemic.
What does this study add?
This study identifies that 51.8% of patients experienced supply issues in the heat of the speculations (April 2020).
The study also shows that the unavailability of HCQ generated high or very high anxiety in 56.1% of patients, and even when supply resumed normally 27.4% were still anxious about the ongoing HCQ supply.
How might this impact on clinical practice or future developments?
The study highlights the need to quickly take corrective measures in case of drug shortage to avoid that the impact of drug unavailability is further aggravated by the impact of anxiety.
Introduction
Hydroxychloroquine (HCQ) is widely used in the treatment of patients with SLE due to its well-established efficacy in controlling disease activity and preventing flare. Moreover, several adjunctive beneficial effects have been reported in patients with SLE, including prevention of damage accrual and improving survival. Thus, HCQ is considered a cornerstone in the treatment armamentarium of SLE, and according to the recent recommendations of the European League Against Rheumatism it should be prescribed to all patients with SLE unless contraindicated.1 2
Based on its antiviral effects in vitro and its effect on SARS-CoV-2 viral load, as demonstrated in a small non-randomised study, in the early days of the COVID-19 pandemic HCQ was largely used worldwide to treat patients with COVID-19.3 4 This caused shortage of the drug and access issues for patients with SLE in multiple countries, raising concerns among patients on the possible impact on disease control and outcomes.5
This study aims to describe the results of a large European survey launched by Lupus Europe through its member network to gather patients’ experience on the recent shortage of HCQ.
Methods
A survey was designed by Lupus Europe’s patient advisory network, initially in English, then translated into 12 additional languages (Bulgarian, Danish, Dutch, Finnish, French, German, Italian, Lithuanian, Polish, Portuguese, Slovak and Spanish). The questionnaire consisted of 7–10 questions depending on the answers provided (table 1).
Answers per country and comparison of the two waves
The survey was distributed through Lupus Europe’s social media, newsflash and its member network on 3 April and remained open on an ongoing basis. Through Lupus Europe’s member organisation’s network, people with lupus were asked to provide their input on their last HCQ purchases once in early April 2020 and another time after 11 August 2020, when speculations on the possible benefit of HCQ in the treatment of COVID-19 ended and after remediation plans had been established with the help of the pharmaceutical industry and health authorities.
Answers were divided into two parts based on the date of filling in the questionnaire, 3–21 April (first wave) and after 11 August (second wave), and the results were compared.
Participants were also asked about their level of anxiety with regard to not being able to have access to HCQ on a Likert scale from 0 (‘not at all’) to 10 (‘extremely’).
Statistical analysis
Continuous variables are reported as mean and SD or median and IQR as appropriate, while categorical variables are reported as percentages. For the purposes of the analysis, data on level of anxiety were categorised as follows: 0–2, no anxiety; 3–4, mild anxiety; 5–6, moderate anxiety; 7–8, high anxiety; and 9–10, extremely high anxiety.
Student’s t-test was used to test differences in mean values between groups for continuous variables. P<0.05 was considered statistically significant and all statistical analyses were performed using STATA V.13 software.
Results
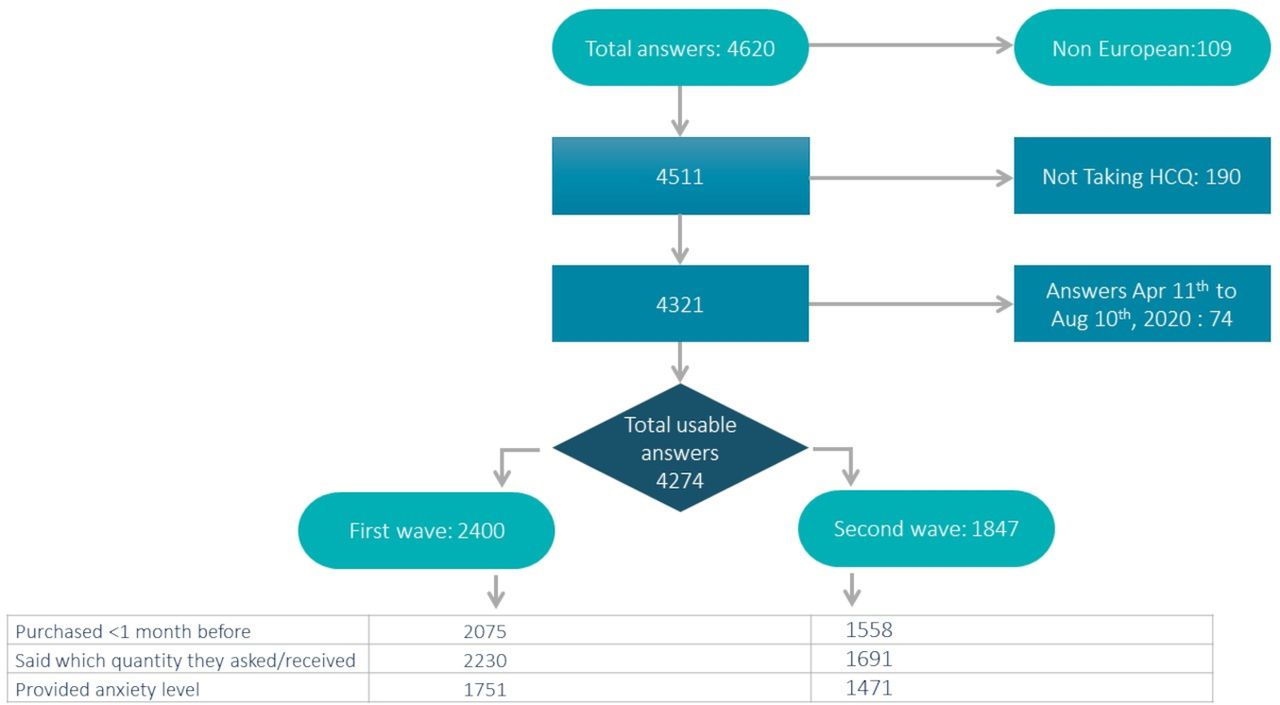
A total of 4620 answers were collected; from this total, 109 were eliminated as they came from non-European countries and 190 declared they did not use HCQ. Seventy-four responded between 22 April and 10 August. The remaining 4247 answers from patients coming from 27 European countries were used in the present analysis. In the analysis on availability, 688 respondents who did not indicate a purchase time or who indicated their last purchase was more than 1 month ago were excluded. Data availability is summarised in a flow chart (figure 1).
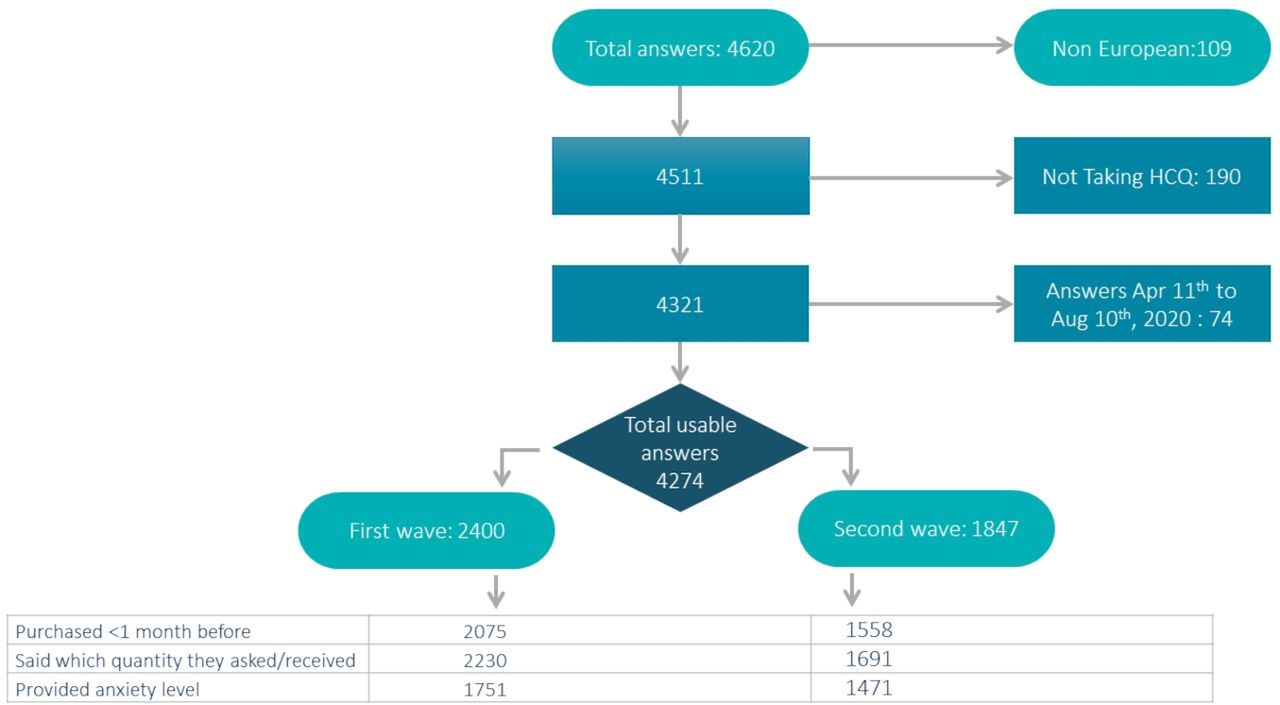
Flow chart of answers/data availability. HCQ, hydroxychloroquine.
Of 2075 patients responding between 3 April and 21 April (first wave), 1001 (48.2%) could get HCQ directly from the first place they asked; 230 (11.1%) could get some, but by going to more than one pharmacy; 498 (24.0%) could not get any HCQ immediately, but obtained some later (next day, few days later, a week later, etc) from their usual pharmacy; lastly, 126 (6.1%) could not get any HCQ, but obtained some later from another source (family, doctor, friends, etc) and 188 (9.1%) could not get any and were still without HCQ at the time of filling in the questionnaire. Thirty-two (1.5%) did not respond to this question.
After 11 August (second wave), 1558 responses were collected. In the second phase, 1297 patients (83.2%) could obtain HCQ directly from the first place they asked; 83 (12.3%) could get it, but had to go to more than one pharmacy; 98 (20.0%) could not get any HCQ immediately, but obtained some later from their usual pharmacy; and 46 (3.1%) could not get any HCQ immediately, but obtained some later from another source (family, doctor, friends, etc). Only 12 (0.8%) patients could not get any and were still without HCQ at the time of filling in the questionnaire. Twenty-two (1.4%) did not respond to this question.
Because several measures to enhance the availability of HCQ to patients with SLE have been taken on a national basis, the situation has evolved differently on a country-by-country basis. Table 1 summarises the key results for each country where more than 15 answers have been obtained in each of the two waves.
All countries showed significant improvement in HCQ availability from April to August and, with the exception of Bulgaria, the proportion of patients without their medication is back to very low level (typically 0%) everywhere. The situation in Bulgaria, where HCQ has typically been absent from the market for several years, is not COVID-19-related.
Participants were also asked to define the number of boxes they requested and the quantities they actually received.
From those responding in wave 1 (n=1751), 851 (48.6%) asked for one box only and received it. Another 74 (4.2%) asked for one box and received a smaller one than expected. 826 (47.2%) asked for more than one box and the majority (593 or 33.9% of all) received them while 233 (13.3%) only received one box. In wave 2, 1475 patients answered this question, among them 660 (44.7%) asked for one box only and received it, while 11 (0.7%) received a smaller box than expected. Interestingly, 804 (54.5%) asked for more than one box and the vast majority (733 or 49.7% of all) received them while 71 (4.8%) only received one box.
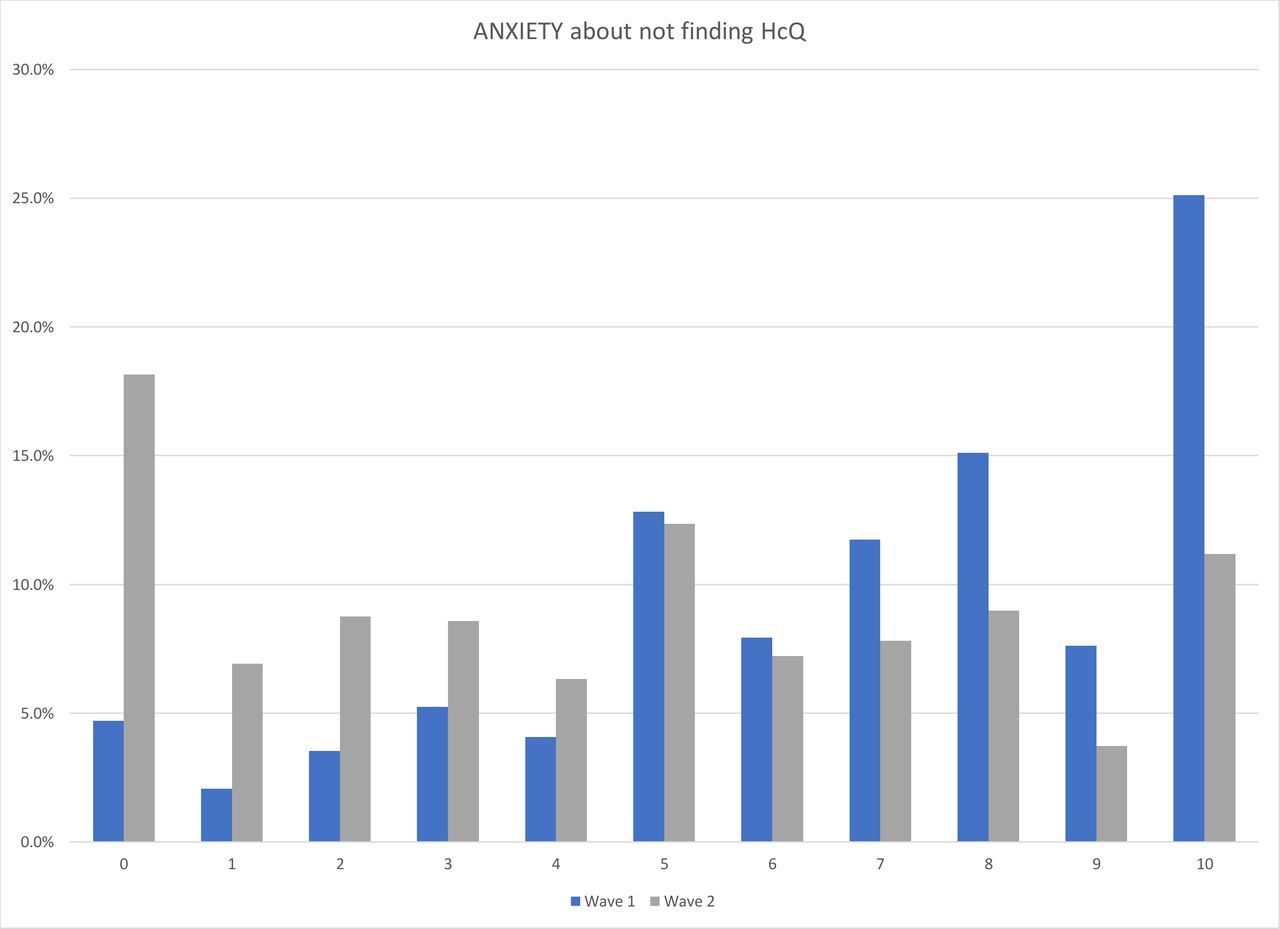
In wave 1 and wave 2, 2230 and 1691 patients (92.9% and 91.6%), respectively, provided answers about their level of anxiety. In wave 1 the median level of anxiety was 7 (IQR 5–9), while in wave 2 the level of anxiety was 5 (IQR 1–7); the difference in the level of anxiety was statistically significant (p<0.001) (figure 2).
{kind=link}
{kind=link}
Level of anxiety of patients in waves 1 and 2. HCQ, hydroxychloroquine.
Excluding Bulgaria, where the issue was still ongoing in August, 562 (27.4%) patients reported an extremely high level of anxiety (9 or 10) in wave 1 and still 162 (10.3%) in wave 2; a high level of anxiety (7 or 8) was reported by 589 (28.7%) and 268 (17.1%) patients in wave 1 and wave 2, respectively.
Discussion
In this study we report the results of a survey exploring the experience of patients with SLE facing HCQ shortage that occurred during the early phases of the COVID-19 pandemic.
The practical difficulties the patients encountered and the subjective discomfort due to this unpredictable situation were analysed by comparing early (April) and late (August) answers.
In the first period, with the exception of Finland where the patients reported that HCQ was available in the majority of cases in the first pharmacy they went to, the vast majority of patients experienced some difficulties in HCQ supply across several European countries and 9.1% of patients have not been able to obtain any.
The situation significantly improved during the second wave of the survey, but 100% availability in the first pharmacy was never reached (with the exception of Finland). Indeed, even excluding Bulgaria, a significant proportion of patients still have to face difficulties in HCQ supply in Lithuania, Poland and Slovakia.
The psychological impact on patients of the crisis in HCQ availability was also analysed with very interesting results. As expected, anxiety about this situation was very common in the first wave of answers, but interestingly this persisted in the second wave in a third of patients despite an objective improvement in drug availability. For these patients the worry that access to treatment could be limited again in the future probably represents a persistent source of anxiety and concern.
Another reflection can be raised on the strategies adopted to overcome the shortage crisis. It appears that pharmacists have more frequently applied limitation tactics (smaller boxes, limitation to one box) in the heat of the crisis (17.5% of cases) than later (5.6% only), while in the post-HCQ crisis the proportion of patients seeking to ‘stock’ HCQ has (further) increased from 47.2% to 54.5%, reflecting a continued discomfort with the guaranteed availability of their drug. We do not have data on the ‘pre-crisis’ level of ‘hoarding’ attempts, but social media comments suggest that 47.2% of patients asking for more than one box at the time was already a substantial increase versus stocking at home precrisis.
This is the first report on patients’ experience of HCQ shortage during the COVID-19 pandemic. The focus on patients’ perspective, the methodology adopted that directly captured patients’ voices and the large participation from several European countries are other undoubted strengths of this work.
On the other hand, we acknowledge that the survey probably lost some country-specific issues in HCQ availability that are not related to the COVID-19 pandemic and in some cases pre-existing.
Also, we note that, as the survey was conducted through Lupus Europe’s network, the participation rate varies by country and the responses might reflect bias as members of patient groups might differ from the total population. Also, the analysis relies on patient declarations; that is, the diagnosis of SLE has not been medically ascertained and the time of (attempted) purchase was as declared by the participants.
In conclusion, the HCQ shortage that happened during the first months of the COVID-19 outbreak had a significant impact on patients with SLE. Even without considering possible clinical effects related to HCQ discontinuation, it has been responsible for psychological consequences including anxiety, concern, and probably a sense of uncertainty about the future. Indeed, while the situation has now been resolved in most countries, the event is leaving significant traces in patients’ mind and behaviours.
Data availability statement
Data are available upon reasonable request. Data from the survey can be made available for research purposes. Request should be made to the board of Lupus Europe by email to secretariat@lupus-europe.org.
Ethics statements
Ethics approval
The study was conducted among Lupus Europe members through an anonymous online survey. As such, no ethics committee approval was required (nor could one be obtained as patient organisations do not have ethics committees).
Acknowledgments
Lupus Europe is very thankful to the patient organisations and individuals that have contributed to the success of this survey through translation, dissemination or providing their input.
Footnotes
Contributors AC and JA (Lupus Europe) were responsible for study ideation and design, data collection and analyses, and manuscript draft preparation. CT and MM participated in the data analysis and manuscript preparation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests LUPUS EUROPE is funded mostly by grants or donations from Pharmaceutical Companies (GSK, UCB, Idorsia, Janssen, Boehringer-Ingelheim, Roche, BMS, Merck), none of which exceeds 25% of total funds collected, and none having a say on the content of our studies.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.