Article Text

Abstract
Background Remission and low disease activity (LDA) have been proposed as the treatment goals for patients with systemic lupus erythematosus (SLE). Several definitions for each have been proposed in the literature.
Objective To assess the impact of remission/LDA according to various definitions on relevant outcomes in patients with SLE.
Methods This systematic literature review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses using PubMed (1946–week 2, April 2021), Cochrane library (1985–week 2, week 2, April 2021) and EMBASE (1974–week 2, April 2021). We included longitudinal and cross-sectional studies in patients with SLE reporting the impact of remission and LDA (regardless their definition) on mortality, damage accrual, flares, health-related quality of life and other outcomes (cardiovascular risk, hospitalisation and direct costs). The quality of evidence was evaluated using the Newcastle-Ottawa Scale.
Results We identified 7497 articles; of them, 31 studies met the inclusion criteria and were evaluated. Some articles reported a positive association with survival, although this was not confirmed in all of them. Organ damage accrual was the most frequently reported outcome, and remission and LDA were reported as protective of this outcome (risk measures varying from 0.04 to 0.95 depending on the definition). Similarly, both states were associated with a lower probability of SLE flares, hospitalisations and a better health-related quality of life, in particular the physical domain.
Conclusion Remission and LDA are associated with improvement in multiple outcomes in patients with SLE, thus reinforcing their relevance in clinical practice.
PROSPERO registration number CRD42020162724.
- systemic lupus erythematosus
- outcome assessment
- health care
- quality of life
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Remission and low disease activity (LDA) have been reported as potential targets in the systemic lupus erythematosus (SLE) treatment.
What does this study add?
Remission and LDA (regardless of the definitions used) are associated with better outcomes.
How might this impact on clinical practice or future developments?
Remission and LDA should be considered as the target for the management of patients with SLE.
However, it is important to have a uniform definition of both.
Introduction
A treat-to-target (T2T) strategy has been proposed for several chronic diseases in order to improve the affected patients’ treatment, and thus, their outcome; in systemic lupus erythematosus (SLE), however, a uniform definition of treatment goals is lacking.
The ideal goal is remission, which was defined in 2015 and modified in 2021 by the DORIS (Definition Of Remission In SLE) group as the absence of clinical disease activity (Clinical Systemic Lupus Erythematosus Disease Activity Index (SLEDAI)=0 and Physician Global Assessment (PGA)<0.5), with no or minimal intake of glucocorticoids (prednisone daily dose not higher than 5 mg/day) and/or immunosuppressive drugs on stable maintenance dose.1 2 However, some modifications of this definition have been reported in the literature.
Nevertheless, as remission state is not achieved frequently,3–5 low disease activity (LDA) has been proposed as an alternative target. To this end, there are several definitions about LDA in the literature; for example, the Asia Pacific Lupus Consortium (APLC) has introduced the lupus low disease activity state (LLDAS): SLEDAI≤4, which allows a low level of disease activity, without activity in major organ systems or new disease activity, PGA≤1, prednisone daily dose not higher than 7.5 mg/day and/or immunosuppressive drugs on maintenance dose.6 The Toronto Lupus Cohort investigators have proposed using the term low disease activity (LDA by Toronto Lupus Cohort): SLEDAI (excluding serology)≤2, without prednisone and immunosuppressive drugs.7
All these definitions allow the use of antimalarials.
The probability of patients achieving these states seems to vary according to a number of factors including race/ethnicity, in particular African ancestry,8 9 age at diagnosis,10 previous disease activity,8 10 11 major organ involvement10 12 and treatment.8–10 Furthermore, the clinical impact of achieving such states in several clinical outcomes has been examined.13 The outcome most frequently evaluated has been organ damage accrual; in fact, in several cohorts, remission and/or LDA have been found to prevent damage, but the exact definitions used for these states have not been uniform.3 6 7 11 14–20
One of the main challenges is to validate whether all these definitions are indeed predictive of outcomes such as organ damage, death, recurrent flares, number of hospitalisations and quality of life (QoL), and which of them would be the better option. Therefore, our aim was to perform a systematic review of the current literature to assess the impact of the existing definitions of remission/LDA on relevant outcomes of patients with SLE.
Methods
Search strategies
A systematic review according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines21 was carried out. The protocol was registered with PROSPERO (CRD42020162724).
We used the electronic databases PubMed (1946-week 2, April 2021), Cochrane library (1985-week 2, week 2, April 2021) and EMBASE (1974-week 2, April 2021) were searched. We used the Medical Subject Heading (MeSH) terms and Key words in all possible combinations using Boolean operators with the following search strategy: ‘systemic lupus erythematosus’, ‘lupus’, ‘SLE’, ‘remission’, ‘low disease activity status’, ‘low lupus disease activity status’, ‘minimal disease activity’. References of all included full-text articles were hand-searched in order to find additional references from the articles that seem to be relevant for the review. Details of the full search strategy are listed in online supplemental table 1.
Supplemental material
These articles were downloaded into EndNote software (V.9.3.2); duplicates were deleted. Two independent teams examined each selected article and performed data extraction independently (MFU-G and CR-S or CM-P and GP-E). In case of disagreement, a third investigator was consulted. Discrepancies were resolved by consensus. The literature review team also made every effort to identify multiple publications from a single cohort.
Criteria for the selection of studies
We included both observational studies (case–control, cross-sectional or cohort) and clinical trials on adults or children with SLE in LDA (using a validated definition) or remission (as defined by available criteria) and reporting different disease outcomes in the follow-up (mortality, damage, flare, health-related QoL (HRQoL), risk of cardiovascular disease, hospitalisations and direct healthcare cost). A minimum sample size of 100 patients was required for an article to be included. Patients needed to have similar duration of follow-up in studies that reported flare rates (using a validated definition) as percentages; alternatively, reported flares per person-years was used in cases where patients had unequal follow-up duration. Damage data, as assessed by the validated instrument (the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SDI)), were considered.
Studies published only as abstracts were excluded.
Articles written in English or Spanish were included. Case reports, case series, editorials, comments, letters and reviews were excluded.
Data extraction
Two reviewers independently screened all articles and applied the eligibility criteria to identify appropriate studies for inclusion; the selected articles were then abstracted, also independently, using a predetermined form. Information was collected on the study characteristics (study design, country, sample size), the number of participants, gender, age, major clinical variables (damage), definition of LDA/remission used, flare rates or flares per person-years, HRQoL scores, HRQoL instruments, hospitalisation rates, mortality rates, direct healthcare cost, definitions of cardiovascular disease and rates or risk of cardiovascular disease. If the same article reported more than one definition of the states or more than one outcome, all of them were included in the respective analyses.
Evaluation of the quality of the studies
The quality of the studies identified was assessed using the Newcastle-Ottawa Scale (NOS) for cohort and case–control studies a tool specifically developed to assess the quality of observational studies.15 The scoring system covers three major domains: selection of cohorts or cases and controls (maximum four points), comparability of selected groups (maximum two points) and ascertainment of either the exposure or the outcome of interest (maximum three points): the resulting score ranges from 0 to 9; a higher score represents a better methodological quality. While there is no validated cut-off value to discern between studies of good or poor quality, studies with a score of ≥7 were arbitrarily defined as being of high quality.22
Strategy for analysis synthesis
Due to the diversity of remission and LDA definitions, outcomes, heterogeneity of the results and of the different statistical tests performed in the selected articles, a meta-analysis was felt not to be feasible for most of the outcome variables; therefore, the studies selected were summarised using a narrative synthesis approach. A description and rationale were provided for grouping studies for synthesis (eg, according to outcomes type). Established metrics were used to measure the direction and magnitude effect of association between remission/LDA and outcomes (eg, OR, risk ratio (RR), HR, among others) when they were available. Summary tables and structured narrative were employed to descriptively summarise and compare each included study and to examine the heterogeneity across studies.23
Results
Study selection and characteristics of studies included
Our search identified 7497 articles, of which 31 studies met the inclusion criteria.3–5 7 11 14–18 20 24–43 The study selection process and reasons for exclusion are shown in figure 1. Four studies were cross sectional, 27 were longitudinal, 12 (38.7%) were from Europe, 10 (32.3%) from Asia and Australia, 5 (16.1%) from Latin America and 4 (12.9%) from the USA and Canada. The large majority of studies were of high quality according to NOS (table 1).

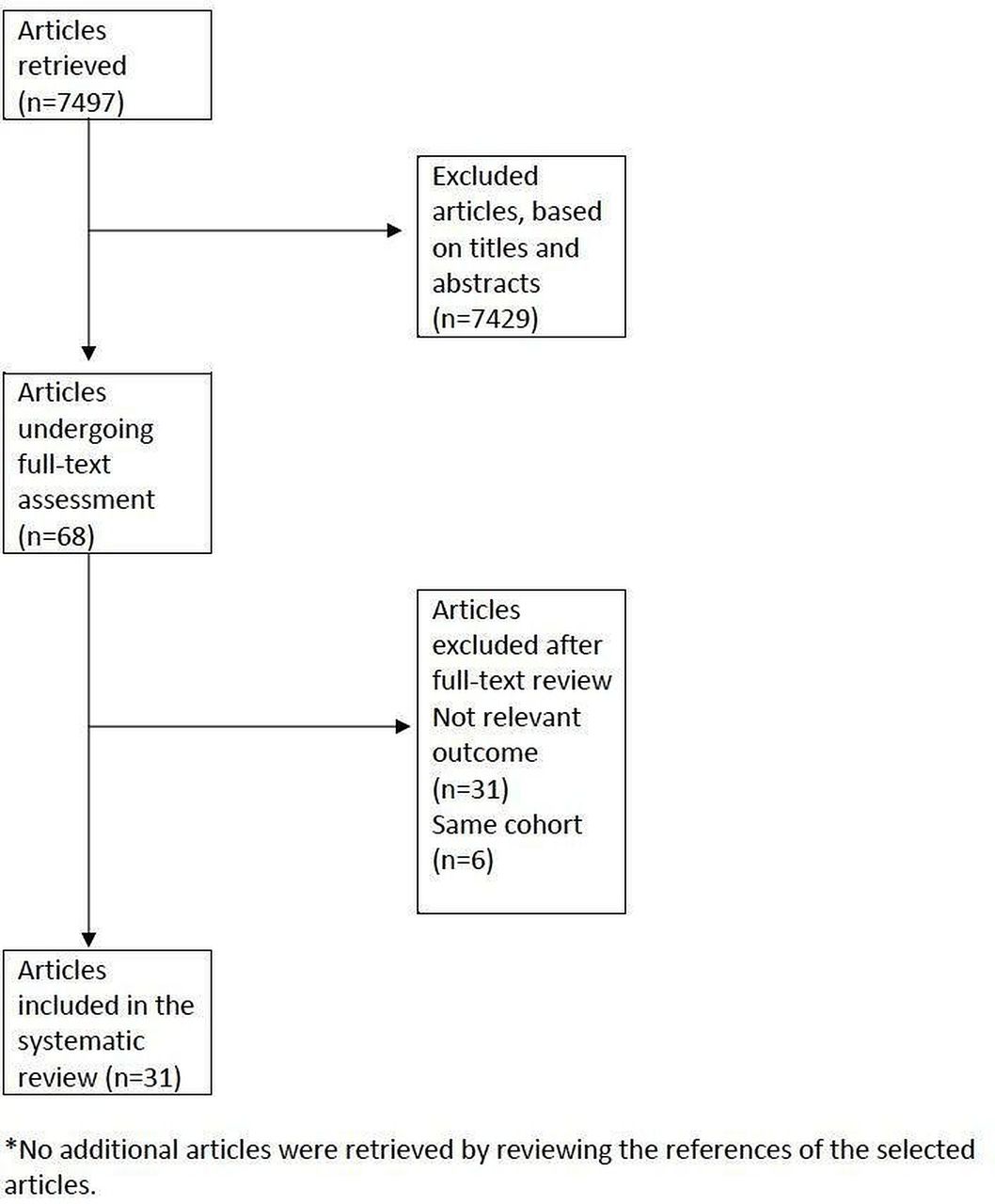{kind=link}
PRISMA flowchart.
Characteristics of the articles included in this systematic review
Remission and LDA rates
The rates of remission and LDA varied depending on both the definition used and the population studied. Remission was more frequent in European populations being as high as 88.1% in one study, but it was as low as 3.5% when the definition excluded patients under treatment and a duration of the remission of at least 7 years. LDA was also more frequent in European populations; however, the rate depended on the definition used; as expected, the less stringent the definition, the more frequently this outcome was achieved. These data are depicted in online supplemental table 2.
Supplemental material
Mortality
Six studies including 3933 patients evaluated mortality as an outcome, two evaluated the impact of remission and LDA on mortality, two only LDA, one only remission and one compared remission and LDA. Among the four studies reporting the impact of LDA on mortality, two of them reported a reduction on mortality (HR 0.3% and 1.4% in those in LDA and 6.9% in those active) and two did not, although the trend was similar (HR 0.30 and 0.81, p: not significant). Among the three studies evaluating the impact of remission (compared with those not on remission) on mortality; two of them reported a reduction on mortality (HR 0.08% and 5% in those in remission and 17.7% in those not in remission), whereas the other did not (HR 0.56, p value not significant). In another report, remission was not statistically different from LDA in terms of the mortality rate. These data are depicted in table 2.
Impact of remission and LDA on mortality*
Damage accrual
Sixteen studies including 8288 patients evaluated damage accrual. In the majority of studies, both remission and LDA prevented damage accrual when compared with patients who did not attain these states (risk measures between 0.04 and 0.95 for remission and between 0.07 and 0.90 for LDA, depending on the definition). In most of the studies, LDA also included those patients who were on remission; however, depending on the definition used, there could be a difference between those in remission and those in LDA, being better to be on remission. These data are depicted in tables 3 and 4.
Impact of remission on damage
Impact of LDA on damage
Flare
Five studies including 3033 patients evaluated longitudinally the occurrence of flares after achieving these states. Remission and LDA reduced the probability of flares in all studies included, regardless of the definition used (HR between 0.26 and 0.70 for remission and between 0.41 and 0.74 for LDA); however, the longer the duration of the state, the lower the risk. Only one study compare remission versus LDA and it did not find a statistically significant difference. These data are depicted in table 5.
Impact of remission and LDA on flare*
Health-related quality of life (HRQoL)
Ten manuscripts including 4480 patients evaluated HRQoL. Remission and LDA were associated with a better HRQoL being this impact more consistent on the physical components of HRQoL, and less so on the mental components of HRQoL. These data are depicted in tables 6 and 7.
Impact of remission on HRQoL*
Other outcomes
Three manuscripts including 802 patients evaluated other outcomes. Being on remission and LDA was associated with a lower hospitalisation rate; LDA was associated with lower medical cost and prolonged remission with lower cardiovascular risk. These data are depicted in table 8.
Impact of remission and LDA on HRQoL*
Impact of remission and LDA on other outcomes*
Discussion
Our systematic literature search showed that being in remission or LDA, regardless of the definitions used, was associated with better outcomes in patients with SLE, the most commonly reported outcomes being lower damage accrual, fewer flares and a better HRQoL. The association with a lower mortality rate was less consistently reported.
In terms of mortality, LDA was associated with lower mortality in two studies, one from the Toronto Lupus Cohort,7 which had a more stringent definition of LDA (SLEDAI ≤2 without treatment) and the other from Norway40 (which allowed a SLEDAI ≤4, excluding new activity and major organ activity, and allowing prednisone ≤7.5 mg/day and immunosuppressive drugs on maintenance dose); similarly, remission was associated with lower mortality in a study from Mexico4 and in one from the UK.5 However, in the GLADEL14 and the LUMINA20 cohorts, the association between remission and LDA and mortality was not statistically significant, although the trend was in the protective direction. This lack of association between achieving these outcomes and mortality could be due to a relatively short follow-up time in these cohorts. The Toronto Lupus Cohort compared remission and LDA and found no statistically significant difference between the two states in terms of mortality.7
Remission was associated with a lower risk of damage accrual in several cohorts from Asia, Europe, North America (USA-Canada) and Latin America3 7 14–16 18 27 34–37 ; however, the minimum time on remission needed to prevent damage accrual has yet to be determined. According to the Padua cohort, being in remission for less than 1 year was not protective against damage,16 whereas according to the Hopkins cohort, being in remission even less than 25% of the follow-up time prevented the accrual of damage.18,18 According to the GLADEL cohort, being in remission prevented not only the accrual of any damage but also the accrual of severe damage (an increase in the SDI of at least 3 points) and from non-glucocorticoid (GC)-related damage and severe damage.14 Additionally, the longer the duration of remission, the lower the probability of damage accrual.16 Similarly, LDA (regardless of how it was defined) has been associated with less damage accrual7 11 14 15 17 18 20 34 38 40 43; however, in the Padua cohort, being on LDA for less than 1 year did not prevent the accrual of damage.17 In the Hopkins cohort, being in LDA for less than 25% of the follow-up did not prevent the accrual of damage.18 Being in LDA prevented also severe damage accrual, non-GC and GC-related damage14; furthermore, the longer the duration of LDAS, the less the damage accrued.20 In the Toronto cohort, being on remission and LDA (SLEDAI ≤2 without treatment) did not differ in terms of the risk of damage accrual7; however, in the Padua cohort, being in remission was associated with a lower risk of damage that being on LLDAS (which allowed a SLEDAI ≤4, excluding new activity and major organ activity, and allowing prednisone ≤7.5 mg/day and immunosuppressive drugs on maintenance dose).17 Probably, the difference in the definitions used in both cohorts could explain these results. Consistent with these results, prolonged remission was associated with a lower probability of cardiovascular events.30
Being in remission or LDA reduced the risk of any flares, being those mild-moderate or severe.7 26 27 38 43 Only in the Toronto cohort remission and LDA (SLEDAI ≤2 without treatment) were compared, but no differences were found.7
Patient perspective is important in defining the optimal treatment target. In previous reports, the association between disease activity and HRQoL has been low or absent.44 Notably, remission and LDA have been found to be associated with a better HRQoL in cross-sectional and longitudinal studies regardless of whether generic or lupus-specific measures were used.3 24 25 29 31–33 39 42 43 These associations were more consistently reported in the physical than in the mental domains, probably because the mental domains are affected also by comorbid conditions such as depression, fibromyalgia and anxiety. It has been suggested that specific measures may ascertain better QoL dimensions specific to patients with SLE.44
Finally, remission and LDA could reduce hospitalisation rate; this has been reported in the Peruvian Almenara Lupus cohort28; LDA could also reduce annual medical cost as reported in a study from an Australian cohort.41 It is important to point out that this information needs to be confirmed in other populations.
Taking together, being on remission or on LDA, regardless of the definitions used, is associated with better outcomes, including mortality, damage, flares, HRQoL, hospitalisation and cost. It is important, however, to point out that a uniform definition of both states is desirable in order to make these results comparable. The current definition of remission, as proposed by the DORIS group, takes into account two physician disease activity measures (clinical SLEDAI=0 and PGA<0.5) as well as treatment (prednisone daily dose not higher than 5 mg/day and/or immunosuppressive drugs on maintenance dose),1 and, even not all the studies used this definition, the large majority used 2015 or 2021 DORIS definitions1 2 or a very similar definition. LDA should be different enough from remission in order to define a group of patients with a better prognosis than those with active disease, but, not as good as the prognosis of those on remission; in this context, the definition proposed by APLC is a good option as it allows a higher level of disease activity (SLEDAI ≤4 and PGA≤1), excludes activity in major organs and new activity, and also allows a higher dose of prednisone (7.5 mg/day) and keeping the immunosuppressive drugs on maintenance dose.6 Additionally, in the KORNET cohort from Korea, LLDAS, but not LDA (SLEDAI ≤2 without treatment) or MDA (minimal disease activity) were predictive of good outcomes.43 However, more information is needed in order to determine if being on remission is better than being on LDA. About the duration of these states, it seems that achieving these states even for a short period of time is associated with better outcomes, but the longer the patient remains on these states, the better the outcomes will be.
These analyses have some limitations; first, as the studies included used different definitions for remission and LDA, a meta-analysis could not be performed. Second, the duration of follow-up in some studies reviewed was not long enough for the assessment of mortality. Third, there are only a few studies for some of the outcomes assessed; this precludes us from making stronger conclusions.
The main strength of this report is the inclusion of several different populations from across the world and several outcomes, allowing us to evaluate the real impact of remission and LDA in the prognosis of patients with SLE.
In conclusion, being in remission or LDA (regardless of the definition) is associated with improved outcomes in patients with SLE. These results reinforce the relevance of these outcomes for the management of patients with SLE.
In order to facilitate the implementation of a T2T strategy in SLE, it is important to have an uniform definition of remission1 and LDA.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @mugartegil, @gponsestel
Contributors All authors were involved in drafting or revising this article critically for important intellectual content, and all authors approved the final version to be published. MFU-G has full access to all of the data from the study and takes responsibility for their integrity and the accuracy of the analyses performed.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MFU-G: Grant/research support from Jannsen, Pfizer, not related to this article. CM-P declared no conflict of interest. CR-S: Grant/research support from Jannsen, not related to this article. GP-E: Grant/research support from JANSSEN and GSK; consultant of JANNSEN, GSK and SANOFI; speakers bureau: Pfizer, JANNSEN and GSK, not related to this article. RFvV: Grant/research support from AbbVie, Arthrogen, Bristol-Myers Squibb, GlaxoSmithKline, Lilly, Pfizer and UCB; consultant of AbbVie, AstraZeneca, Biotest, Bristol-Myers Squibb, Celgene, GSK, Janssen, Lilly, Medac, Merck, Novartis, Pfizer, Roche and UCB, not related to this article. GB: Grant/research support from GSK, Pfizer; consultant of Novartis, SOBI, not related to this article. GA declared no conflict of interest. BAP-E: Grant/research support from GSK, Jannsen; consultant of GSK, Janssen; speakers bureau: GSK, Janssen, not related to this article.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.