Article Text

Abstract
Objective Antiphospholipid syndrome (APS) is characterised by increased cardiovascular morbidity and mortality, related to thrombo-inflammatory and atherogenic mechanisms. We examined the achievement of traditional cardiovascular risk factor (CVRF) therapeutic goals in APS versus other high cardiovascular risk disorders such as rheumatoid arthritis (RA) and diabetes mellitus (DM), and trends over time.
Methods 122 patients with APS (74 primary APS, female 68%, mean age 44.5±11.3) were classified according to their first visit (2011–2015 and 2016–2020 APS subgroups, 61 patients in each subgroup) and matched 1:1 for age/sex with patients with RA and DM. Cardiovascular risk was estimated by the Systemic Coronary Risk Evaluation, and the CVRF therapeutic targets were defined according to the European Society of Cardiology (ESC) guidelines. Individual and multiple CVRF control was compared between APS subgroups, and in APS versus RA and DM.
Results We found a comparable or higher prevalence of CVRFs between APS and age-matched/sex-matched patients with RA and DM but low CVRF target attainment in APS according to the ESC guidelines. Despite improving trends between 2011–2015 and 2016–2020, CVRF control in high/very high-risk patients with APS was 12%, 18%, 24% and 35% for low-density lipoprotein, waist circumference, exercise and body mass index, respectively, and 59%–65% for triglycerides, high-density lipoprotein (HDL) and blood pressure, in 2016–2020 subgroup. CVRF control was worse in APS versus RA for smoking (p=0.014), HDL (p<0.001), waist circumference (p=0.042) and five CVRFs (p=0.030), and versus DM for exercise (p=0.077). Similar results were found in the sensitivity analysis.
Conclusions Comparable prevalence of modifiable CVRFs to RA and DM but suboptimal CVRF target achievement was observed in APS, especially in high/very high-risk patients, highlighting the need for CVRF management strategies.
- antibodies
- antiphospholipid
- antiphospholipid syndrome
- atherosclerosis
- cardiovascular diseases
Data availability statement
The data that support the findings of this study are available by the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Cardiovascular disease, especially stroke and coronary artery disease, is a leading cause of morbidity and mortality in antiphospholipid syndrome (APS).
Little is known about the prevalence and management of traditional cardiovascular risk factors (CVRFs) in APS.
No previous study evaluated the attainment of therapeutic targets of modifiable CVRFs according to established general population guidelines in patients with APS.
What does this study add?
Patients with APS have a high prevalence of traditional CVRFs, comparable or higher to other disorders of high cardiovascular risk such as rheumatoid arthritis (RA) and diabetes mellitus (DM), a cardiovascular disease risk-equivalent.
Despite improving trends between 2011–2015 and 2016–2020, CVRF target achievement according to general population guidelines is suboptimal in APS, especially in high/very high-risk patients.
CVRF target attainment is worse in APS versus RA for smoking, waist circumference, high-density lipoprotein and multiple CVRFs, and in APS versus DM for exercise.
How might this impact on clinical practice or future developments?
Better awareness of the need for regular assessment and strict control of traditional CVRFs following strategies used in other chronic diseases of high cardiovascular disease (CVD) risk can help in better prevention and management of the frequent, and often fatal, CVD in APS.
Development of disease-specific CVD risk prediction tools and management guidelines based on the evidence from large, prospective studies in APS is needed.
Introduction
Antiphospholipid syndrome (APS) is a rare and complex systemic autoimmune disorder characterised by a wide range of macrovascular and microvascular manifestations ranging from single to recurrent, or multiple simultaneous events in the case of catastrophic APS.1 2 Cardiovascular events, mainly stroke and myocardial infarction, are the most common causes of morbidity and mortality in APS, affecting mostly young adults.2 Cardiovascular disease (CVD) in APS is derived by immunothrombotic and atherogenic mechanisms including antiphospholipid antibodies (aPL)-mediated endothelial dysfunction, platelet cell activation and aggregation, pro-inflammatory cytokines, complement system and neutrophils activation, endothelial cell proliferation, intimal hyperplasia and oxidised low-density lipoprotein (LDL)-beta2-glycoprotein I complexes induced differentiation of macrophages to foam cells.3–7
A high prevalence of traditional cardiovascular risk factors (CVRFs)8–13 and metabolic syndrome13 14 has been demonstrated by a few previous studies examining their presence in patients with APS. We recently observed a comparable or even higher prevalence of CVRFs in 326 patients from the Greek APS registry vs 652 age-matched/sex-matched patients from the Greek rheumatoid arthritis (RA) registry. Specifically, a significantly higher prevalence of arterial hypertension (29.8% vs 20.9%) and ever-smoking (53.7% vs 40.5%) was noted in patients with APS than age-matched/sex-matched patients with RA, while hyperlipidaemia (24.2% vs 20.7%) and obesity (21% vs 19.6%) were comparable between the two groups.15 Interestingly, a prospective study of asymptomatic aPL carriers showed that 50% of patients who developed APS manifestations had coincident CVRFs at the time of their first thrombotic event,16 while hypertension and dyslipidaemia have been recognised as independent risk factors for arterial thrombosis in large APS cohorts.9 11 12 17 18
Guidelines for the prevention and management of CVD in the general population such as those of the European Society of Cardiology (ESC) have highlighted the importance of modifiable CVRF control.19 20 Moreover, attainment of multiple versus individual CVRF targets is recommended, as it has been associated with >50% lower risk of atherosclerotic cardiovascular events in disorders with very high CVD risk such as diabetes mellitus (DM).21 Despite a high CVD burden in rheumatic and musculoskeletal disorders (RMDs), the assessment and management of CVD risk remains inadequate. This is mostly related to insufficient knowledge and implementation of CVD prevention guidelines in the general population and lack of RMD-specific recommendations for CVD risk management.22–26 In the recent European League Against Rheumatism (EULAR) recommendations for the management of APS, the screening and strict control of traditional CVRFs was highlighted in the overarching principles,27 however, there is no evidence about the CVRF target achievement in patients with APS according to established guidelines.19 20
Our goal was to assess the attainment of therapeutic targets of modifiable CVRFs in patients with APS based on their CVD risk category, as defined by ESC guidelines, and whether individual and multiple CVRF control has changed over time in the past decade. We also compared the individual and multiple CVRF target achievement in patients with APS versus other rheumatic and non-rheumatic conditions of high CVD risk, such as RA and DM.
Patients and methods
Study population
We assessed for eligibility all adult patients (≥18 years) who fulfilled the classification criteria for APS (1) and followed at the Rheumatology Unit of the First Propaedeutic and Internal Medicine Department, Laiko Hospital. All patients fulfilled at least one of the clinical updated Sapporo APS classification criteria and the following laboratory criteria, present on two or more occasions at least 12 weeks apart: Lupus anticoagulant (LA) tested according to the International Society on Thrombosis and Haemostasis guidelines, anticardiolipin antibodies (aCL) and/or anti-beta2glycoprotein I (anti-β2GPI) antibodies of IgG and/or IgM isotype at medium or high titres measured by a standardised ELISA.1
This is a cross-sectional study including eligible patients with primary or SLE-related APS (SLE-APS), classified in two subgroups according to the date of their first visit at our unit: between 2011 and 2015 (2011–2015 APS group) and between 2016 and 2020 (2016–2020 APS group). Patients with APS were matched in a 1:1 ratio for age and sex with eligible patients with RA and DM (type I or type II) followed in the Rheumatology and Diabetes Unit of our Department, respectively. Given the well-known high prevalence of atherosclerotic CVD events in patients with DM compared with the other groups, we also excluded patients with a history of atherosclerotic CVD events in all groups for reasons of comparability. Other exclusion criteria were age ≥70 years because Systemic Coronary Risk Evaluation (SCORE) could not apply in this age group, as well as the presence of concomitant DM (or RA, for patients with DM), active malignancy, pregnancy and acute illness.
Patients in the 2016–2020 APS group were not matched with patients with RA because according to the updated 2015/2016 EULAR recommendations for CVD risk management in patients with RA and other forms of inflammatory joint disorders, a 1.5 multiplier in SCORE should be applied for all patients with RA,28 not applicable to patients with APS. The aforementioned recommendations included a modification of the previous ones published in 2010, which suggested the application of a 1.5 multiplication factor in patients with RA with at least two of the following three criteria: (a) disease duration of >10 years; (b) Rheumatoid factor (RF) or anti-cyclic citrullinated peptides (anti-CCP) antibody positivity; (c) presence of severe extra-articular manifestations.29
Recorded parameters
The following parameters were retrieved from the patients’ medical files at the time of their first visit at our department: (a) demographic data: age, sex, ethnicity; (b) disease-related parameters: year of diagnosis, disease duration, APS classification (primary or SLE-APS) and the DM type for patients with DM; (c) traditional CVRFs: systolic and diastolic blood pressure (BP) after at least 10 min of rest, as the average of three sequential readings taken 1 min apart, (Microlife WatchBP Office, Microlife, Widnau, Switzerland), fasting total, LDL and high-density (HDL) lipoprotein cholesterol levels, fasting triglycerides levels, current smoking status and pack-years of smoking, physical activity level (measured in minutes of exercise per week), body mass index (BMI) (calculated as weight/height2), waist circumference (measured in cm), chronic kidney disease (CKD) (glomerular filtration rate (GFR) <60 mL/min/1.73 m²) and haemoglobin A1c (HbA1c) levels for patients with DM and (d) use of hydroxychloroquine, antihypertensives and lipid-lowering medication at the time of patients’ first visit.
Hypertension was defined as the average of three sequential office BP measurement >139/89 or use of antihypertensives. Obesity was defined as a BMI of at least 30 kg/m2. Dyslipidaemia in patients with APS and RA was defined as fasting LDL >160 mg/dL or use of lipid-lowering medication. The definition of dyslipidaemia used for patients with DM is mentioned in the ‘Definition of CVD risk target control’ section.
Definition of CVD risk target control
For CVD risk stratification in patients with APS and RA, we used SCORE prediction of 10-year risk of fatal CVD for low-risk European countries calculated with the online calculator provided by u-prevent.com. SCORE is a validated instrument recommended by the ESC that includes age, gender, office measurements of systolic BP and fasting total and high-density lipoprotein cholesterol.30 We used the first edition of SCORE,30 and not the 2021 SCORE2, because all patients in the study were enrolled between 2011 and 2020. The low-risk SCORE chart dedicated to Greek population was used for all patients.
Based on the individual SCORE estimation, each of the patients with APS and RA was assigned to one of the following CVD risk categories: low, moderate, high and very high risk. Depending on each patient’s risk category, target levels for major CVRFs, such as BP, LDL, HDL, triglycerides levels, smoking status, physical activity level and body weight were defined according to the ESC guidelines. The 2012 and 2016 ESC guidelines for CVD prevention19 20 were used to determine CVD risk targets for patients with APS, as the corresponding guidelines for the 2011–2015 and 2016–2020 time periods, respectively, examined in the study (table 1). The therapeutic targets for major CVRFs based on 2021 ESC guidelines for CVD prevention31 are also mentioned in table 1, for reasons of comparability. We classified patients with APS with arterial thrombotic events (stroke, myocardial infarction and peripheral arterial thrombosis) as very high-risk patients because the 2012 and 2016 ESC guidelines classified these manifestations in the very high-risk category without defining their origin (atherosclerotic and/or thrombotic).
Therapeutic targets for traditional CVRFs based on the corresponding two time periods of the study 2012 and 2016 ESC guidelines for CVD prevention in the general population and on 2013 ESC guidelines on diabetes, prediabetes and CVDs in collaboration with the EASD for patients with DM
Total CVD risk estimation, using a risk estimation system such as SCORE, is recommended for adults >40 years of age, unless they are automatically categorised as being at high risk or very high risk based on documented CVD, kidney disease or highly elevated single risk factor.19 20 Consequently, patients with APS and RA under 40 years of age were assigned to a low-risk category, unless a specific modifier was present, while patients with APS and RA >40 years of age were assigned to a risk category based on SCORE.
According to 2013 ESC guidelines for diabetes, prediabetes and CVDs, developed in collaboration with the European Association for the Study of Diabetes (EASD),32 patients with DM with at least one other CVRF or target organ damage should be considered as very high risk and all other patients with DM as high risk. The CVRFs that were taken into consideration to classify patients with DM are: hypertension (use of antihypertensives or office BP measurement ≥140/≥90 mm Hg); obesity (BMI ≥30 kg/m2); dyslipidaemia (fasting total cholesterol ≥200 mg/dL, LDL ≥130 mg/dL, HDL <40/dL for men/<45 mg/dL for women or use of lipid-lowering medication); smoking status (current) and CKD (GFR <60 mL/min/1.73 m²). The CVRF targets for patients with DM are shown in table 1. It should be noted that the HDL target was not assessed in patients with DM because it is not mentioned explicitly as a therapeutic target for DM in the ESC/EASD guidelines.
Statistical analysis
Data are presented as mean±SD (when normally distributed), as median and IQR (when there is deviation from normality), or when indicated, as absolute number and percentage (relative frequency). To compare the participant groups’ characteristics, we used Student’s t-test (in normally distributed data) and Mann-Whitney U test (in not normally distributed data) for quantitative variables and Pearson’s χ2 or Fisher’s exact tests for qualitative variables. To assess differences between patient groups concerning the CVRF target attainment, we used Pearson’s χ2 or Fisher’s exact tests.
We also examined composite CVRF control, including fulfilment of any of three, four or five CVD risk targets out of seven (smoking status, BP, LDL cholesterol, HDL cholesterol, triglycerides, BMI, physical activity) for patients with APS and RA, and out of six therapeutic targets (smoking status, BP, LDL cholesterol, triglycerides, BMI, physical activity) for patients with DM.
We performed a sensitivity analysis as follows: (1) patients with arterial thrombotic APS were not a priori classified in the very high-risk CVD category (as we did in the main analysis according to the 2012 and 2016 ESC guidelines where the atherosclerotic vs thrombotic origin of stroke, MI or peripheral artery disease was not clarified) because in the newer 2019 ESC guidelines, only atherosclerotic events are included; (2) patients with APS were re-matched for age and sex with patients with RA without excluding those with atherosclerotic CVD as we did in the main analysis for reasons of comparability (higher prevalence of atherosclerotic CVD events in patients with DM vs the other groups) but following the other exclusion criteria reported in the ‘Methods’ section (age ≥70 years, DM, active malignancy, pregnancy and acute illness).
A p value <0.050 was considered statistically significant. STATA (V.13.0, College Station, Texas, USA) was used for all statistical analyses.
Results
From 133 patients with APS assessed for eligibility, 5 were excluded due to concomitant DM, 3 due to prior atherosclerotic CVD events, 1 because of concomitant DM and atherosclerotic CVD and 2 were aged ≥70 years. A total of 122 patients with APS (female 68%, mean age 44.5±11.3 years, 74 with primary APS, 48 with SLE-APS, all Caucasian) were included in the study. Sixty-one were allocated in the 2011–2015 APS subgroup and 61 in the 2016–2020 subgroup, based on the date of their first visit at our unit. Patients in the first subgroup were age-matched/sex-matched with 61 patients with RA, and the patients with APS of each subgroup were matched in a 1:1 ratio for age and sex with patients with DM.
Characteristics of the entire APS group and two APS subgroups are shown in online supplemental table S1. The comparison of major CVRFs (hypertension, dyslipidaemia and smoking) between the disease groups is shown in figures 1–4A, and that for all modifiable CVRFs is presented in online supplemental tables S1-4. The differences in CVRF therapeutic target attainment are presented in figures 1–4B and in more detail in online supplemental tables S1-4 (eg, BP or lipid goal attainment, with or without antihypertensive or lipid-lowering treatment, respectively). The CVD risk classification according to SCORE prediction tool for all patient groups is presented in online supplemental figure 1. There were missing data in some CVRFs; the denominator is the total number of available values for each CVRF in online supplemental tables S1-4. In 1 of 61 patients of the 2011–2015 APS subgroup, and in 4 of 61 patients of the 2016–2020 subgroup, there were missing data for at least 1 of 7 required CVRFs for CVD risk classifications according to SCORE.
Supplemental material
Supplemental material
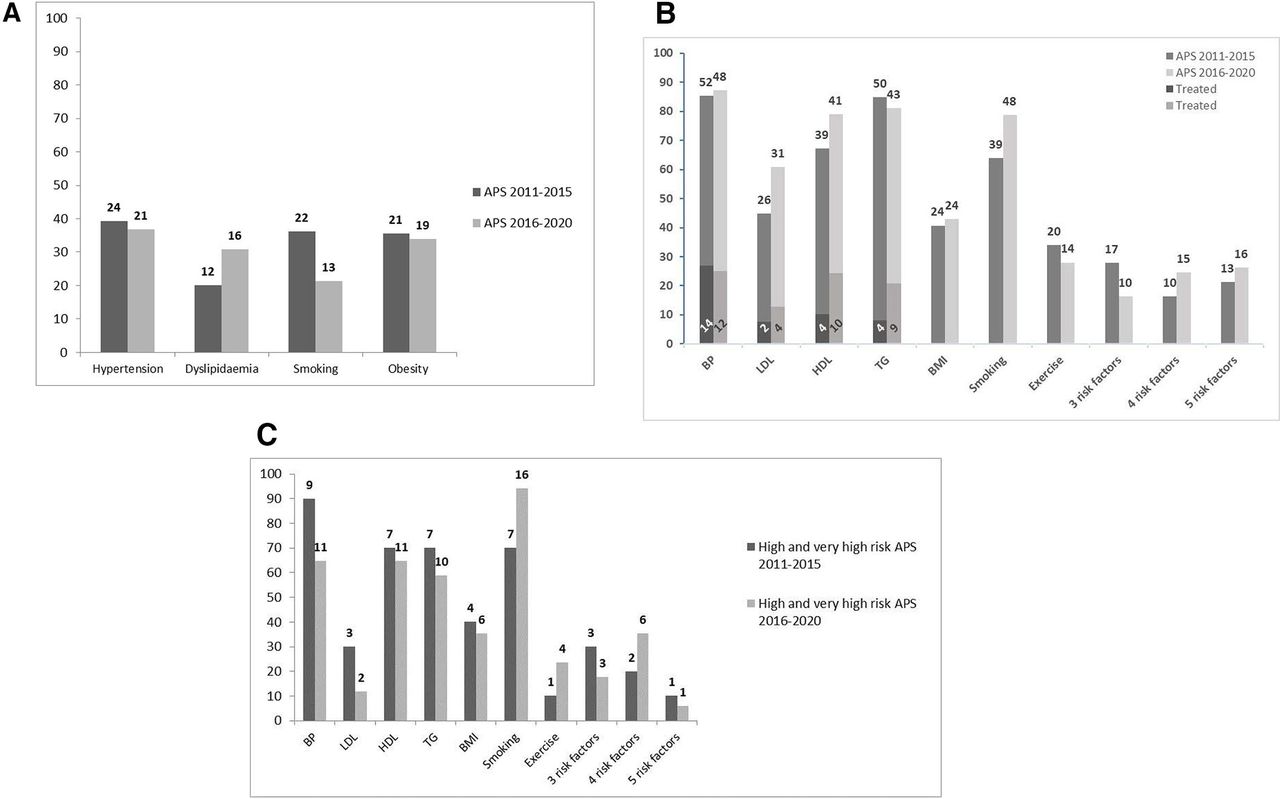
(Α) Prevalence of major CVRFs (hypertension, dyslipidaemia, current smoking, obesity) in the 2011–2015 APS group versus the 2016–2020 APS group. (Β) CVRF target attainment in the 2011–2015 APS group versus the 2016–2020 APS group. (C) CVRF target attainment in the 2011–2015 APS group versus the 2016–2020 APS group for high and very high CVD risk patients. Three risk factors: any of three CVRFs; four risk factors: any of four CVRFs; five risk factors: any of five CVRFs. BP target: <140/90 mm Hg; LDL target: <115 mg/dL, <100 mg/dL, <70 mg/dL in low/moderate, high and very high-risk patients, respectively; HDL >40 mg/dL in men and >45 mg/dL in women indicate lower risk; TG <150 mg/dL shows lower risk, BMI target: 20–25 kg/m2; smoking target: no current smoking; exercise target: at least 150 min/week of moderate aerobic physical activity or 75 min/week of vigorous aerobic physical activity. Absolute numbers are presented. There are missing data for some CVRFs. CVRFs, cardiovascular risk factors; BMI, body mass index; BP, blood pressure; HDL, high density lipoprotein; LDL, low-density lipoprotein; TG, triglycerides.

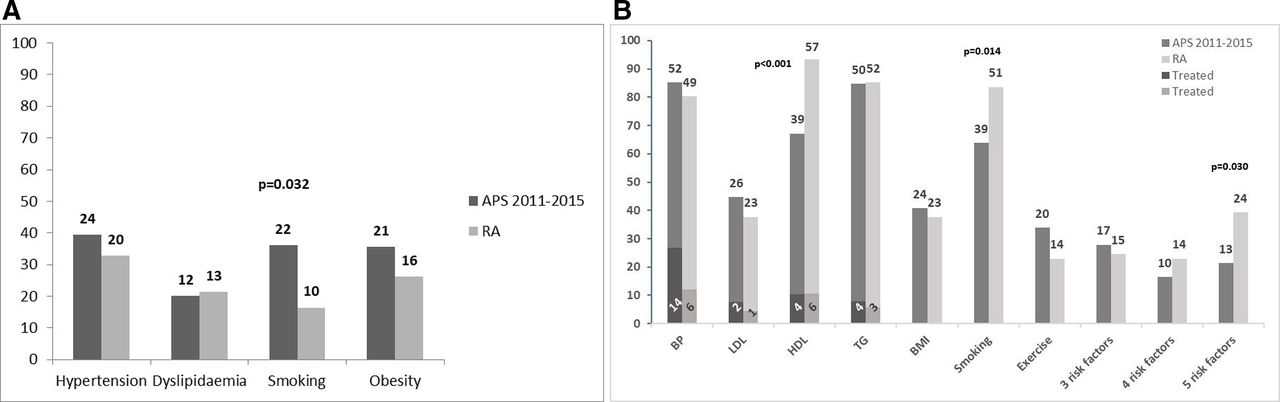
(Α) Prevalence of major CVRFs (hypertension, dyslipidaemia, current smoking, obesity) in the 2011–2015 APS group versus age-matched and sex-matched patients with RA. (Β) CVRF target attainment in the 2011–2015 APS group versus age-matched and sex-matched patients with RA. Three risk factors: any of three CVRFs; four risk factors: any of four CVRFs; five risk factors: any of five CVRFs BP target: <140/90 mm Hg; LDL target: <115 mg/dL, <100 mg/dL, <70 mg/dL in low/moderate, high and very high-risk patients, respectively; HDL >40 mg/dL in men and >4 5 mg/dL in women indicate lower risk; TG <150 mg/dL shows lower risk, BMI target: 20–25 kg/m2; smoking target: no current smoking; exercise target: at least 150 min/week of moderate aerobic physical activity or 75 min/week of vigorous aerobic physical activity. Absolute numbers are presented. There are missing data for some CVRFs. CVRFs, cardiovascular risk factors; BP, blood pressure; LDL, low-density lipoprotein; HDL, high-density lipoprotein; TG, triglycerides; BMI, body mass index.

(A) Prevalence of major CVRFs (hypertension, dyslipidaemia, current smoking, obesity) in 2011–2015 APS group versus age-matched and sex-matched patients with DM. (B) CVRF target attainment in the 2011–2015 APS group versus age-matched and sex-matched patients with DM. Three risk factors: any of three CVRFs; four risk factors: any of four CVRFs; five risk factors: any of five CVRFs. BP target: <140/90 mm Hg; LDL target: <115 mg/dL, <100 mg/dL, <70 mg/dL in low/moderate, high and very high-risk patients, respectively; TG <150 mg/dL shows lower risk, BMI target: 20–25 kg/m2; smoking target: no current smoking; exercise target: at least 150 min/week of moderate aerobic physical activity or 75 min/week of vigorous aerobic physical activity. Absolute numbers are presented. There are missing data for some CVRFs. CVRFs. CVRFs, cardiovascular risk factors; BP, blood pressure; LDL, low-density lipoprotein; TG, triglycerides; BMI, body mass index.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Prevalence of major CVRFs (hypertension, dyslipidaemia, current smoking, obesity) in the 2016–2020 APS group versus age-matched and sex-matched patients with DM. (B) CVD risk targets attainment in the 2016–2020 APS group versus age-matched and sex-matched patients with DM. Three risk factors: any of three CVRFs; four risk factors: any of four CVRFs; five risk factors: any of five CVRFs BP target: <140/90 mm Hg; LDL target: <115 mg/dL, <100 mg/dL, <70 mg/dL in low/moderate, high and very high-risk patients, respectively; TG <150 mg/dL shows lower risk, BMI target: 20–25 kg/m2; smoking target: no current smoking; exercise target: at least 150 min/week of moderate aerobic physical activity or 75 min/week of vigorous aerobic physical activity. Absolute numbers are presented. There are missing data for some CVRFs. CVRFs. CVRFs, cardiovascular risk factors; BP, blood pressure; LDL, low-density lipoprotein; TG, triglycerides; BMI, body mass index.
No statistically significant difference was observed in the characteristics of two APS subgroups except the higher prevalence of primary APS and shorter disease duration, and most importantly, in the prevalence of CVRFs or their treatments (antihypertensives, lipid-lowering agents), except the lower LDL levels in the 2016–2020 APS group (online supplemental table S1). The majority of patients with APS were classified as low/moderate risk, 83.3% in the 2011–2015 and 70.18% in the 2016–2020 subgroup. A percentage of 1.67% in the first subgroup was assigned to high risk, while 15% in the 2011–2015 vs 29.8% in 2016–2020 subgroup in the very high-risk category (online supplemental table S5, online supplemental figure 1). High-risk patients with APS were classified as such because of markedly elevated CVRF (very high BP, marked hypercholesterolaemia) or moderate CKD. Patients with APS with atherosclerotic CVD were excluded from the study, however, patients with thrombotic events (stroke, myocardial infarction, peripheral arterial thrombotic disease) were eligible for the study and were subsequently classified as very high-risk patients, according to the ESC guidelines. More specifically, one patient in the 2011–2015 APS subgroup was assigned to high risk due to very high BP (>180 mm Hg) and moderate CKD, 8 patients were classified as very high risk due to thrombotic events, and one patient as very high risk due to thrombotic CVD event and the presence of CKD; no patient in the 2016–2020 subgroup classified in the high-risk category, while one patient was assigned to very high risk due to severe CKD, 14 were classified as very high risk because of thrombotic CVD events and two as very high risk due to thrombotic CVD events and the presence of CKD. The results of the sensitivity analysis by not excluding patients with atherosclerotic CVD events and not a priori classifying thrombotic patients with APS in the very high-risk category showed: (a) in the APS 2011–2015 group (62 patients in total, 1 patient added with atherosclerotic CVD), 57 patients were classified in the low-risk to moderate-risk category and 4 patients in the high/very high-risk category (1 patient with very high BP and moderate CKD; 1 with severe CKD, 1 with SCORE 5% (a SCORE ≥5% and <10% is classified in the high-risk category according to the ESC guidelines), 1 with atherosclerotic CVD); (b) in the APS 2016–2020 group (63 patients in total, 2 patients added with atherosclerotic CVD), 54 patients classified in the low-risk to moderate-risk category and 5 patients in the high/very high- risk category (3 patients with severe CKD, 2 with atherosclerotic CVD).
Regarding the CVRF target attainment, a significantly higher level of attainment of the waist circumference and the LDL targets was observed in the 2016–2020 subgroup, the latter only when patients currently on lipid-lowering medication were excluded (online supplemental table S1). There was also a better smoking target control in the 2016–2020 APS group, but without statistical significance (78.7% vs 63.9%, p=0.072). Concerning multiple CVRF control, there were no significant differences between the two APS subgroups (figure 1B, online supplemental table S1). Among patients with APS classified as high risk and very high risk specifically, 70%, 10%, 40%, 10%, 90%, 30%, 70%, 70% and 10% achieved the smoking, exercise, BMI, waist circumference, BP, LDL, HDL, triglycerides and five CVRFs goal, respectively in the 2011–2015 group, and 94%, 24%, 35%, 18%, 65%, 12%, 65%, 59% and 6%, respectively in the 2016–2020 subgroup (figure 1C). The results of the sensitivity analysis did not significantly differ from those in the main analysis in the entire APS group (online supplemental table S6). For example, CVRF control in the entire APS group was 72%, 32%, 42%, 30%, 86%, 60%, 72%, 83% for smoking, exercise, BMI, waist circumference, BP, LDL, HDL and triglycerides target, respectively. CVRF control in the high-risk/very high-risk group remained suboptimal: in the 2016–2020 group, it was 20%, 20%, 40% and 40% for LDL, waist circumference, exercise and BMI, respectively, and 60% for triglycerides and HDL and 80% for BP.
Comparing the 2011–2015 APS group with the age-matched and sex-matched RA group, a higher prevalence of current smoking (p=0.032) and pack-years of smoking (p=0.005) but lower diastolic BP, median cholesterol and median HDL levels were detected in patients with APS versus patients with RA (online supplemental table S2). The percentages of patients on antihypertensives and lipid-lowering treatment were comparable. All patients with RA were classified as low/moderate CVD risk vs 83% in the 2011–2015 APS group (p=0.001) (online supplemental table S5). This may be partly explained by the fact that patients with RA with a history of atherosclerotic CVD were excluded, as well as patients with RA aged ≥70 years because SCORE could not apply in this patient group. In addition, none of the patients with RA had moderate or severe CKD or markedly elevated single CVD risk factors, for example, very high BP, probably due to our increased awareness of the high CVD risk in these patients due to EULAR recommendations for CVD management in APS. Furthermore, the 2015/2016 update of the recommendations for CVD management suggesting the use of 1.5 multiplication factor for all patients with RA was published later than the first visit of our matched patients with RA and therefore the 1.5 multiplication factor was adopted only for patients who fulfilled at least two criteria (>10 years disease duration, RF and/or anti-CCP positivity, presence of severe extra-articular manifestations), according to the previous 2010 version, and not for all patients. Regarding CVRF target attainment, patients with APS had significantly worse smoking, waist circumference and HDL target control than patients with RA (online supplemental table S2). Patients with APS had a significantly higher proportion of BP target fulfilment, when taking into consideration only the patients currently on antihypertensives. Concerning the composite risk factor control, the results were comparable between the APS and RA groups, except the five CVRF target attainment that was worse in patients with APS versus patients with RA (p=0.030) (figure 2B). In the sensitivity analysis, one patient with history of atherosclerotic CVD was added in the 2011–2015 group and the entire APS group (n=62) was re-matched for age and sex with patients with RA, as described in the ‘Statistical analysis’ section. From 62 matched patients with RA, 4 patients had prior atherosclerotic CVD and were classified in the high/very high CVD risk category, and 58 classified in the low-risk/moderate-risk category. CVRF control was worse in the APS group 2011–2015 (n=62) vs the matched RA group (n=62) for smoking (p=0.007), HDL (p<0.001), waist circumference (p=0.004) and five CVRFs (p=0.019), in accordance with the results of the main analysis (online supplemental table S7). CVRF target of the APS 2011–2015 (n=4) vs patients with RA (n=4) in the high/very high-risk category was as follows: 75% vs 100% for smoking, 25% vs 25% for BMI, 0% vs 25% for waist circumference, 25% vs 0% for exercise, 50% vs 50% for BP, 75% vs 0% for LDL, 50% vs 100% for HDL, 50% vs 75% for triglycerides, but the very small sample size does not allow to draw any conclusions.
First visit characteristics in the 2011–2015 APS subgroup did not differ significantly from those in the age-matched and sex-matched DM group, except a higher prevalence of dyslipidaemia in patients with DM (figure 3A). However, a significantly higher percentage of patients with DM versus patients with APS was classified as high and very high risk (online supplemental table S5), given that DM is classified by definition as high risk and as very high risk when at least one CVRF is present according to the ESC/EASD guidelines. The prevalence of hypertension, as well as the percentages of antihypertensive and lipid-lowering treatment, were comparable (online supplemental table S3). A percentage of 19.7% and 80.3% of patients with DM were assigned to high and very high CVD risk categories, respectively. The percentage of patients with LDL (44.8% vs 15.3%, p<0.001) and BP target attainment (85.3% vs 65.6%, p=0.012) was lower in patients with DM than patients with APS. The results for LDL target were also confirmed in the group of patients currently on lipid-lowering treatment, while those on BP target in the group of patients currently on antihypertensives. The achievement of multiple CVRF target control was comparable between the two groups (figure 3B).
In the comparison of the 2016–2020 APS subgroup with the age-matched/sex-matched DM group, exercise level and smoking prevalence were lower in APS than DM, while triglycerides levels were significantly higher in APS, with a trend for LDL levels (figure 4A). In addition, a significantly higher percentage of patients with DM were classified as high and very high risk compared with patients with APS (21.3% and 78.7% vs 0% and 29.8%, respectively) (online supplemental table S5). Regarding CVRF control, the exercise target attainment was worse in APS versus DM (28% vs 44%, p=0.077) but a significantly lower percentage of patients with DM than patients with APS achieved the smoking (p=0.047) and the LDL target goal (p<0.001), which remained significant after the exclusion of patients currently on lipid-lowering medication (online supplemental table S4). No difference was found in multiple CVRF control between the APS and DM groups, except the four CVRF target attainment that was better in patients with APS than patients with DM (p=0.036) (figure 4B). It should be noted that 79 (65%) of 122 matched patients with DM had type I DM and 43 (35%) patients had type II DM. A significantly higher number of patients with type II DM fulfilled the HbA1c target compared with those with type I DM (56.1% vs 30%, p=0.007), but no statistically significant difference was found between the two DM groups that were matched with the 2011–2015 and the 2016–2020 APS subgroups, respectively.
Discussion
Our study showed a high prevalence of traditional CVRFs in patients with APS but low therapeutic target attainment, supporting the need for increased awareness among care providers. To our knowledge, this is the first study to assess individual and multiple modifiable CVRF target achievement in patients with APS according to established guidelines in the general population, and to perform a direct comparison between APS and other rheumatic and non-rheumatic conditions of high CVD risk, such as RA and DM.
CVD, and especially stroke and myocardial infarction, are part of the definition of APS and represent its most common arterial vascular manifestations, observed in 26% and 5% of patients, respectively, in large international cohorts.33 They are also the leading causes of death in APS, referring to 19.8% and 5.5% of deaths, respectively, over a 5-year follow-up of the European APS cohort.2 In addition to thrombotic mechanisms, antiphospholipid antibody-mediated atherogenesis and the impact of traditional CVRFs on CVD in APS have been increasingly recognised.3–7 27 In the present study, we found a similar or even higher prevalence of traditional CVRFs in APS compared with that in RA and DM. A few previous studies8–10 13 have examined the prevalence of CVRFs in APS versus age-matched and sex-matched healthy individuals. In a recent multicentre study, we showed for the first time that hypertension and ever smoking were more prevalent in patients with APS versus age-matched and sex-matched patients with RA, while the frequency of dyslipidaemia and obesity were comparable.15 In addition, in a previous case-control study conducted by our group, patients with primary APS accumulated more traditional cardiovascular risk factors than age-matched and sex-matched patients with DM.34
Although CVD is one of the major causes of morbidity and mortality in several RMDs and especially in inflammatory arthritis and SLE, an inadequate CVD risk assessment and management has been reported.22–26 35 36 In a cohort study including 720 patients with RA, 69% had an indication for lipid-lowering or antihypertensive drugs, however, 42% of them received inadequate treatment and 40% no treatment at all.36 In our APS cohort, an improvement in some CVRFs control (waist circumference, LDL, a trend for smoking) between the two halves of the past decade may suggest a potential increase in CVRF control awareness. It should be noted that the 2016–2020 APS group had lower baseline LDL levels, which may be partly explained by a more extended use of lipid-lowering agents in this group (21% statin use in 2016–2020 vs 12% in 2011–2015 group). The lower baseline LDL levels in the 2016–2020 APS group could also explain the statistically significant difference between the two APS subgroups in the LDL target achievement, when excluding the patients currently on lipid-lowering treatment. We did not find statistically significant differences in the prevalence of hypertension, use of antihypertensives and the BP target achievement between the two time periods.
Comparing the 2011–2015 APS subgroup with the matched RA patients, patients with APS had lower target attainment levels than patients with RA for several CVRFs such as smoking, waist circumference and HDL. Regarding the composite risk factor control, five factor target attainment was significantly higher in the RA group. Collectively, our findings showed a better target attainment for several CVRFs in RA compared with APS group, probably due to an increased CVD risk awareness in the context of systemic inflammation in RA that was further improved by the 2010 and 2015/16 EULAR recommendations for CVD management in RA and other forms of inflammatory joint disorders.28 29
Comparing APS versus DM, a higher percentage of patients with DM were classified at high or very high CVD risk versus patients with APS, but this finding would be expected according to the ESC/EASD guidelines.32 Patients with DM with at least one CVRF or target organ damage are considered as very high risk and therefore approximately 80% of matched patients with DM were classified in the very high-risk category, and all other patients with DM as high risk. Consequently, therapeutic targets were generally stricter in DM and therefore more difficult to achieve. Additionally, the majority of matched patients with DM were type I DM and only one-third of them had optimal glycaemic control.
We performed a sensitivity analysis by not including a priori patients with APS with arterial thrombotic events in the very high-risk group since the newer ESC guidelines clarified that only atherosclerotic CVD events are classified as very high risk and by also including patients with atherosclerotic CVD events in the comparison of patients with APS and RA (excluded in the main analysis due to the higher CVD prevalence in DM vs the other groups). The results were similar with those in the main analysis for the majority of CVRF targets in the entire APS and the two APS subgroups, and for the comparison between the patients with APS and patients with RA.
The strengths of our study include (1) the assessment for the first time of CVRF target achievement in patients with APS based on established general population guidelines, and especially in high/very high-risk patients; (2) the comparison of CVRF prevalence and CVRF target achievement between APS and age-matched and sex-matched rheumatic and non-rheumatic disorders of high CVD risk such as RA and DM; (3) the assessment of any differences in CVRF control between two time periods of a significant number of patients with APS (n=61 for each subgroup), considering the rarity of the syndrome. However, multicentre studies with prospective design are warranted to confirm our results. Another limitation is the use of stricter therapeutic targets for traditional CVRFs according to established guidelines in DM than those in APS and RA, making difficult the comparison of therapeutic goal achievement between them.
Benefits of CVRF evaluation and control are well known in the general population and among patients of high CVD risk. Better understanding of atherogenic—in addition to thrombotic—cardiovascular risk in patients with APS, and development of CVD-specific—in addition to thrombotic18—risk prediction tools, as well as disease-specific CVD risk management strategies should be included in the future CVD risk management research agenda in APS. However, it should be noted that previous efforts for the development of disease-specific CVD risk prediction models in RMDs with well-known high CVD risk and higher prevalence than APS, such as RA, have been proven to be inadequate. Consequently, given the high CVD risk observed in APS, CVD risk assessment and control measures similar to those in DM, could be implemented in patients with APS.
In conclusion, our study showed a high prevalence of several traditional CVRFs, comparable or even higher of that in RA and DM, but suboptimal CVRF target attainment and especially in high/very high-risk patients, despite an improving trend across the two halves of the past decade. Awareness of CVD risk in APS among healthcare providers and patients, and regular assessment and control of modifiable traditional CVRFs following similar CVRF control strategies to other disorders of high CVD risk, can help to improve CVD risk management in APS.
Data availability statement
The data that support the findings of this study are available by the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the hospital’s Institutional Review Board of Laiko General Hospital (Laiko Hospital Scientific Council; IRB number 7748) and all participants gave informed consent.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors EB: acquisition of data, analysis of data, drafting and critical revision of the manuscript. NT: acquisition of data, critical revision of manuscript. PPS: interpretation of data, critical revision of manuscript. MGT: conception and design of the study, acquisition of data, analysis and interpretation of data, drafting and critical revision of the manuscript, guarantor. All authors have read and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.