Article Text

Abstract
Objective In systemic lupus erythematosus (SLE), disease activity and glucocorticoid (GC) exposure are known to contribute to irreversible organ damage. We aimed to examine the association between GC exposure and organ damage occurrence.
Methods We conducted a literature search (PubMed (Medline), Embase and Cochrane January 1966–October 2021). We identified original longitudinal observational studies reporting GC exposure as the proportion of users and/or GC use with dose information as well as the occurrence of new major organ damage as defined in the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index. Meta-regression analyses were performed. Reviews, case-reports and studies with <5 years of follow-up, <50 patients, different outcomes and special populations were excluded.
Results We selected 49 articles including 16 224 patients, 14 755 (90.9%) female with a mean age and disease duration of 35.1 years and of 37.1 months. The mean follow-up time was 104.9 months. For individual damage items, the average daily GC dose was associated with the occurrence of overall cardiovascular events and with osteoporosis with fractures. A higher average cumulative dose adjusted (or not)/number of follow-up years and a higher proportion of patients on GC were associated with the occurrence of osteonecrosis.
Conclusions We confirm associations of GC use with three specific damage items. In treating patients with SLE, our aim should be to maximise the efficacy of GC and to minimise their harms.
- glucocorticoids
- outcome assessment
- health care
- lupus erythematosus
- systemic
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Exposure to glucocorticoid (GC) has been recognised as contributing to damage occurrence in patients with lupus; however, this association has been reported in different ways, leading to inconsistent conclusions.
What does this study add?
This study examines the information available in the literature from lupus cohorts/studies and confirms the association between GC exposure and osteonecrosis, cardiovascular events and osteoporosis with fractures.
How might this impact on clinical practice or future developments?
Physicians should use GC judiciously to maximise their efficacy and minimise their harms.
Introduction
Systemic lupus erythematosus (SLE) is a chronic, relapsing-remitting inflammatory autoimmune disease with multisystemic manifestations.1 Inflammation due to active SLE, if not promptly and adequately treated, leads to irreversible tissue or organ damage that negatively impacts survival and health-related quality of life.2–5 While the overall survival of patients with SLE has gradually improved over the past four decades, organ damage, particularly that of the renal and neuropsychiatric systems, has been shown to limit further improvement of the short-term and long-term survival rates of patients with SLE.6 Therefore, clinicians and scientists are actively pursuing factors that lead to organ damage in patients with SLE and devising strategies to mitigate them.
While uncontrolled SLE disease activity potentially leads to eventual tissue and organ damage, pharmacological treatment of SLE can also be contributory.6 Among various drugs that are used in patients with SLE, clinicians have long recognised that glucocorticoids (GC), while often clinically beneficial, can induce damage, particularly in the ocular, cerebrovascular, cardiovascular and musculoskeletal systems.7–11 Nevertheless, the different impacts of several modes of GC exposure including its daily and cumulative doses, as well as the mere presence of GC exposure on major organ damage in patients with SLE have not been fully addressed. The differences in study populations and chronological periods, research designs and methodologies used, duration of disease and study observation as well as the different ways of expressing GC exposure (daily, cumulative, oral vs parenteral) have led to inconsistent conclusions.7 9 12
In this study, we sought to examine the data published in the past 55 years by evaluating all longitudinal observational studies published between 1 January 1966 and 18 October 2021. Our initial aim was to conduct a meta-analysis of estimated effects of GC on damage using the relevant literature but that was not feasible due to the relatively small number of studies that supported such analysis (vide infra). Thus, a systematic literature review and meta-regression analyses of the association between GC exposure and the occurrence of major SLE-related organ damage were conducted. Damage was defined as per the Systemic Lupus International Collaborating Clinic/American College of Rheumatology Damage Index (SDI) or the corresponding terms prior to the availability of this instrument. Among the items included in the SDI, we evaluated overall damage as well as those items more probably related to GC as previously described: cataracts, cerebrovascular accidents (CVA), myocardial infarction (MI), overall cardiovascular events (CVE) including angina and coronary artery bypass graft, avascular/osteonecrosis and osteoporosis with fractures.
Methods
Literature search and data entry
This systematic literature review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Review and Meta-analysis) guidelines; the protocol has not been registered;13 online supplemental material 1 corresponds to the PRISMA checklist. The search was conducted on PubMed (Medline), Embase and Cochrane (from 1 January 1966 to 18 October 2021) for original longitudinal observational research articles that reported GC (glucocorticoids is the MESH term) exposure in terms of (i) proportion of GC users in the cohort and/or (ii) GC use with dose information, as well as the occurrence of major organ damage reported as incidence as defined in the SDI. The following keywords ‘overall damage’, ‘cataracts’, ‘cerebrovascular’, ‘stroke’, ‘cardiovascular’, ‘angina’, ‘myocardial infarction’, ‘coronary artery bypass’, ‘avascular necrosis’, ‘osteonecrosis’, ‘osteoporosis’ or ‘fractures’ were used in respective combinations with the keyword ‘lupus’ (see online supplemental material 2). Articles excluded were those with a sample size smaller than 50, with an observation duration less than 60 months, and others not describing the proportion of patients with SLE who were exposed to GC and/or without definite elaboration of the dose and/or duration of GC exposure. Studies in which the disease started in childhood, those with selected populations based on organ involvement (eg, only patients with lupus nephritis, for example) or based on presence or absence of a specific damage item (eg, osteonecrosis or stroke) and others in which damage was not examined, either globally or for any of its individual components, were also excluded. For studies conducted using the same cohort/population, the most recent one, or the one that provided more detailed data on GC use was chosen. However, if the same cohort/population reported different outcomes in different articles, the relevant article was included for each outcome. Also, if two articles from the same cohort reported the SDI, and one of them reported one specific SDI domain and another domain was reported in the other article, only the most recent or the one that provide more detailed data on GC was included for the SDI analysis, but each of them was retained for the analysis of the specific domain item that they reported. Similarly, if the same cohort/population reported GC use in different ways in different articles, both articles were used but in separate analyses of the different GC use variable.
Supplemental material
Supplemental material
Disease duration was defined as the time that elapsed from the diagnosis of SLE to entry into the cohort whereas duration of follow-up was the time elapsing from entry into the cohort, to the time the analyses were conducted.
The literature search was conducted by two independent teams; the first one was constituted by MUG, GSA, CEF and CRS and the second one by AM, JWYL, NYK and BD. Both teams extracted the data in an electronic database in the form of an Excel spreadsheet. MUG and NYK collected the extracted data, checked for the accuracy of the data inputted and returned potentially problematic data to their respective literature searchers for verification. Subsequently, each team convened to resolve potential duplications, questions related to specific publications and conflicts of data extraction before finalising the dataset. Then, the data from both teams were again reviewed and collated by MUG’s team. These data were then used for the various analyses. Figure 1 depicts the steps taken in the selection of the articles included in these analyses according to the PRISMA guidelines.13

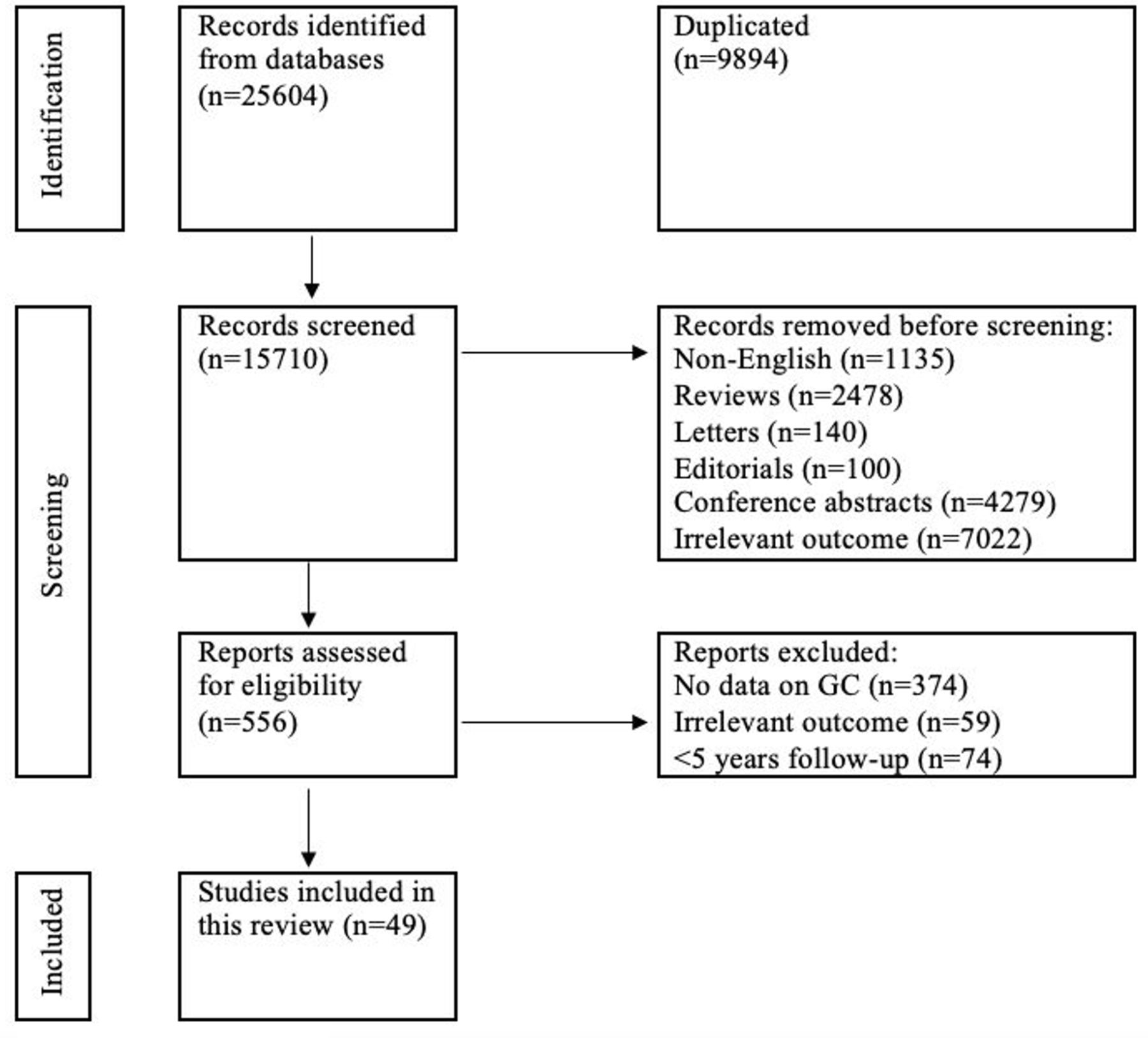{kind=link}
Identification of studies via databases and registries. GC, glucocorticoids.
Evaluation of the quality of the studies
Following the PRISMA guidelines, the quality of the studies identified for this meta-regression analysis was assessed. To this end, the Newcastle-Ottawa Scale (NOS) for cohort and case-control studies, a tool specifically developed to assess the quality of observational studies was used. The scoring system covers three major domains: (1) selection of cohorts (maximum 4 points), (2) comparability of cohorts (maximum 2 points) and (3) ascertainment of either the exposure or the outcome of interest (maximum 3 points). The resulting score ranges from 0 to 9 with a higher score representing a better methodological quality. While there is no validated cut-off value to discern between studies of good or poor quality, studies with a score of ≥7 are arbitrarily considered high quality.14 This grading was not used to either include or exclude a given study.
Statistical methods
The outcomes examined were the different types of damage including: (1) difference in average SDI scores between the beginning and the end of follow-up, (2) cataracts, (3) CVA, (4) MI, (4) overall CVE, (6) avascular necrosis/osteonecrosis and (7) osteoporosis and fractures (both had to be present). The rate of change in overall damage, as measured by the SDI, has been modelled with the rate scaled to represent the rate of increase per 100 patient years. Other damage rates have been scaled to represent rates in units of patients developing damage per 100 patient years. The analyses have been based on a random effects meta-regression model15 with the logarithm of the rate of damage as the outcome variable and with treatment related variables and variables defining other cohort characteristics as explanatory variables.
Restricted maximum likelihood estimation of this regression model was implemented in the R package ‘metafor’, as described by Viechtbauer et al.16 Further details on the methodology are provided in online supplemental material 3.
Supplemental material
The treatment-related variables that have been extracted from the publications, when possible, are the following: (1) proportion of patients using GC, (2) average daily oral GC as prednisone/prednisone equivalent (PDN)) dose across patients (mg), (3) average cumulative GC as PDN dose across patients (per 10 g); (4) average cumulative GC as PDN dose across patients per year of follow-up (g) and (5) proportion of patients using parenteral GC (as methylprednisolone). Additional variables examined include: (1) year of publication, (2) average age at diagnosis, (3) average age at cohort entry and (4) average disease duration at cohort entry. For studies in which more than one group of patients was studied, each group was examined independently; this applied to 5 of the 49 selected articles17–21 so that 54 cohorts are available for analysis.
Pooled estimates of the rates of different types of damage from a simple meta-analysis model will be presented along with I2 values which assess relative heterogeneity and an absolute measure of heterogeneity, τ2.22 Corresponding ‘forest plots’ associated with these estimates, including the estimates from the set of studies used for the meta-analysis, are provided as online supplemental material 4; 95% CI are also shown. From meta-regression models, transformed regression coefficients representing relative risk estimates along with 95% CI and significance levels are presented and R2 values representing the estimated amount of heterogeneity explained were also calculated, although these should be interpreted cautiously with small sample sizes. Detailed plots of the log rates of damage vs the various potential moderators for the different damage types are provided in online supplemental material 5.
Supplemental material
Supplemental material
Results
Out of 15 710 publications screened, 15 661 were excluded leaving 49 articles which involved 16 224 patients with SLE, 147 555 (90.9%) female and 1469 (9.1%) male, selected for these analyses (see figure 1 and online supplemental material 6 for details on the articles included (n=49) and the reasons for excluding the others (n=15 661)). Five of the 49 studies included were published prior to 2000, 10 between 2000 and 2009, 23 between 2010 and 2019 and 11 between 2020 and 2021. At study entry, patients included had a mean (SD) age of 35.1 (7.4) years and a mean disease duration of 37.1 (41.6) months; their mean follow-up time was 104.9 (49.4) months,9 17–21 23–65 each mean calculated as a weighted average of cohort averages. Seventeen out of the 49 studies had a high quality (at least seven points in the NOS). The cohorts available provided data for one or more of the outcomes examined as noted in table 1. In this table, a summary of the amount of data available for the different types of damage is presented; the number of cohorts providing information on damage varies from 15 to 29.
Supplemental material
Data availability for overall and specific damage items
Rates of damage
Table 2 presents overall estimates of the rates of damage and associated I2 relative heterogeneity measures. As might be expected, there is evidence of substantial heterogeneity in these rates of damage accrual across studies (from 80.1% for MI to 99.2% for overall damage) given the variation in cohort characteristics. Absolute heterogeneity estimates varied from 0.30 for CVA to 0.64 for osteoporosis with fractures. The estimated rate for changes in the SDI scores per 100 patient years was 9.89 (95% CI 7.59 to 12.88), corresponding to an expected change for one patient in 1 year of 0.0989. For the development of specific damage (yes/no) per 100 patient years, the range of rates was from 0.40 (0.27 to 0.59) for MI to 1.14 (95% CI 0.82 to 1.60) for osteoporosis, corresponding to 0.40% and 1.14% of patients developing damage in a 1-year period.
Estimated overall rates of observed damage
The forest plots associated with these analyses are provided as online supplemental material 4.
Damage and treatment variables
Table 3 presents estimated relative risks associated with treatment related variables in univariate meta-regression models. Plots associated with these analyses are provided in online supplemental material 5. There are no demonstrable relationships between the use of GC and the occurrence of overall damage. When examining the different specific damage items, support for such association was found for CVE and the daily dose of PDN (mg/day) (1.12 (95% CI 1.02 to 1.24), p=0.019), based on six cohorts with virtually all the heterogeneity in rates explained. Osteonecrosis was demonstrably associated with the proportion of patients receiving GC (1.24 (95% CI 1.02 to 1.51, p=0.03)), based on 17 cohorts explaining 11.5% of the heterogeneity, and with the cumulative PDN dose, adjusted (g/year) or not (per 10 g increase) for the number of years of follow-up (1.67 (95% CI 1.22 to 2.29), p=0.002 and 1.23 (95% CI 1.12 to 1.34), p<0.001), based on 12 cohorts and explaining 49.3% and 100.0% of heterogeneity, respectively. Osteoporosis with fractures was associated with the daily dose of prednisone (mg/day) (1.21 (95% CI 1.11 to 1.33, p<0.001), based on five studies and explaining 86.7% of the heterogeneity although largely based on one small study with a high rate and high average dose.61 A similar relationship was seen for the adjusted cumulative dose although, even with 11 studies, the estimated relationship was not significant.
Univariate meta-regression results
Damage and other variables
Univariate meta-regression results for the additional potential moderating variables such as year of study, age at diagnosis and age at entry into the cohort are presented in table 4 with associated plots in online supplementary material 5. Of interest, the accrual of overall damage seems to decrease from the earlier publications to the most recent ones with comparable effects estimated for cataracts, CVA and MI, the latter being highly significant and cataracts and CVA not achieving 5% significance. In addition, age at cohort entry seems to play an important role in increasing the occurrence of CVE. As well, a later average age at diagnosis is associated with a higher rate of CVE but this is heavily influenced by one study with a very high age at diagnosis.32 Longer disease duration was found to be associated with osteoporosis with fractures, but this is largely the result of having one study with a high rate of damage and high average disease duration.61 Other significant relationships in table 4 associated with age at diagnosis and age at entry are largely due to one or two cohorts with very much older ages. This can be visualised in online supplemental material 5 where explanatory variable plots are displayed. If cohorts with age at diagnosis or age at entry greater than 50 are excluded from the respective analyses, then no significant relationships are maintained except for the age at cohort entry relationship with CVE already mentioned.
Additional univariate meta-regression results
As expected, the majority of patients in the cohorts were female and the limited variation in the proportion of females was not demonstrably associated with any measure of damage except osteoporosis with fractures which was highly significant based largely on one study61 and, to some extent, cataracts with this relationship of lower rates in females generating a p value of 0.06 based on 17 studies. Plots related to the proportion of females are also included in online supplemental material 5.
Relationships between damage and GC related variables were unaltered by adjustment for other variables in selected multivariate analyses when sufficient data were available (results not shown).
Sensitivity analysis
Ten of the 49 articles, bolded in online supplemental material 6, in which the data for the intake of GC were only recorded at the baseline visit but not over time were removed, and the same analyses redone. The assumption for the primary analysis presented earlier is that the patients were taking a similar amount of GC over their follow-up, which may or may not have been the case. Nevertheless, there were, overall, no marked differences observed in comparison with the analysis in which all 49 articles were included (data not shown) except that the suggestive relationship between CVA and proportion of GC use entirely disappears (RR=0.96, 95% CI (0.62 to 1.49)) with the removal of three studies, two of which had a very low rate of damage and low rate of GC use.
Discussion
In this comprehensive systematic literature review and meta-regression analysis, we have confirmed associations of the use of GC with the occurrence of damage in patients with SLE. This applies to overall CVE, osteonecrosis and osteoporosis and fractures but not to overall damage. For CVE, it was with the average daily PDN dose; for osteonecrosis, it was with the proportion of patients on GC, and with the average cumulative adjusted or unadjusted PDN dose/years of follow-up and for osteoporosis with fractures, it was with the average daily PDN dose. It is also noteworthy that in the most recent publications included in these analyses, less damage seems to have been accrued as compared with the older studies; that was the case for overall damage and MI. This has also been reported in the Toronto cohort, with a reduction of CVE from 11% (in patients followed from 1975 to 1992 to 3.8% in those followed from 1999 to 2016).12 Whether this is due to the inclusion of patients with less severe disease, better overall control of the inflammatory disease process or cardiovascular risk factors or a decrease in the use of GC is not readily apparent from the data reviewed. Younger age seems to protect against the occurrence of osteoporosis with fractures, whereas longer disease duration seems to favour their occurrence. In terms of gender, women seem to experience osteoporosis with fractures more frequently than men; however, as noted, this seems to be driven primarily by one study and thus the finding should be interpreted with caution.
Our findings are concordant with the clinical experience of those treating lupus patients as well as with the literature on the subject. The Hopkins Cohort, for example, has shown a higher cumulative average GC dose to be associated with damage accrual.66 A higher cumulative dose of GC was also associated with a higher risk of cataracts and osteoporosis with fractures, even after adjusting for possible confounders.7 Similarly, in an Australian study, Apostolopoulos et al reported that a higher dose of GC was associated with an increase of GC-related and non GC-related damage.67 The independence of GC effects on damage accrual is supported by a large multicentre Asia Pacific cohort study which revealed strong associations between GC use and damage accrual in SLE, after adjustment for disease activity and, importantly, in a subgroup without evidence of active disease.68 In two other case-control studies comparing patients with and without osteonecrosis, osteonecrosis was associated with the use and/or dose of GC.69 70 These supporting articles were not included in our analysis because they did not fulfil our inclusion criteria; the Hopkins cohort reported the risk of damage as a function of the cumulative dose of PDN (dividing their patients into five groups) but did not provide the information for the entire group of patients;66 the report from the Asia Pacific cohort had a median follow-up of 2.2 years66 and the last two articles were case-control studies comparing patients with and without osteonecrosis and were excluded because they evaluated only selected populations.69 70 It is also noteworthy that no association was found between damage accrual, more specifically osteonecrosis, and the use of intravenous methylprednisolone. Although this was based on few studies, it is also consistent with the results observed in the Hopkins66 and Cruces cohorts.17 25
Our study has limitations. First, we need to consider that given the limited data available (only 49 studies in total and between two and 29 studies per outcome) and the potential for chance results due to multiple comparisons, the numerical results presented should be viewed with caution and not be overinterpreted. Second, it is also relevant to point out that the meta-regression methodology used is essentially an association study based on group (ie, cohort) characteristics. This contrasts to the methodologically more rigorous investigation of associations based on individual (ie, patient) characteristics, which is more common in meta-analyses and would be expected to provide more definitive conclusions. Group association studies are generally felt to be at risk of the so-called ‘ecological’ fallacy arising when other factors are associated with both the outcome (ie, damage) and the group characteristic used in the analysis (ie, GC use).71 This is basically a type of confounding. For example, although not examined in this study, ethnicity might influence the rate of damage and (through, for example, different healthcare systems) the extent of GC treatment. This limitation arose because, after carefully reviewing the available literature, there were a small number of articles meeting our criteria for selection and the variability in, and sparsity of, the recording of GC use. Also, in a meta-regression, each cohort essentially provides only one data point for each analysis and thus its power is limited in any event. Third, an attempt was also made to develop a standardised GC variable as a single explanatory variable and thus increase the sample size, but that did not lead to any substantial increase in power. Fourth, there may also be some question about the suitability of the use of the cumulative GC dose variable in a study of rates as this is influenced by the length of follow-up time. This was the reason for including the cumulative dose per year variable. Fifth, we realise that the use of GC reflects disease activity which by itself may lead to damage. However, due to the lack of information about disease activity in many of the original studies included in this meta-regression, we have not been able to adjust for it in our analysis. Sixth, while some degree of overlap for patients from the same cohorts was possible, this is unlikely given that we have included only one article per outcome or per method of reporting GC use.
To conclude, in this comprehensive meta-regression analysis of longitudinal cohort studies, in spite of their limited number and considerable heterogeneity, we confirm associations of the use of GC with damage. This applies to CVE, osteonecrosis and osteoporosis with fractures. Our study highlights the difficulties in conducting such analyses42 and suggests that the relationship between GC and damage is quite complex. Our aim should be to judiciously use GC to maximise their efficacy and minimise their harms.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MFU-G and AM are joint first authors.
MC, VF and GSA are joint senior authors.
Twitter @mugartegil, @lupusreference, @Lupusdoc, @prfortin, @lupusdoclim, @ericfmorand, @anisurrahman60, @ronfvv, @SueManzi
Contributors All authors were involved in drafting or revising this article critically for important intellectual content and have approved the final version to be published. MFU-G, VF and GA have full access to all of the data from the study and take responsibility for their integrity and the accuracy of the analyses performed. VF an GA are the guarantors
Funding This work was partially supported by a grant to the SLICC group from the Lupus Foundation of America, Inc.
Competing interests JB and RFvV are Editors-in-Chief of Lupus Science & Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.