Article Text

Abstract
Objective To investigate the frequency and determinants of flare in Chinese patients with lupus, focusing on the effect of glucocorticoid (GC) tapering on flare in patients who achieved low disease activity or remission.
Methods We collected baseline and follow-up data from all consecutive patients in a prospective lupus cohort between January 2017 and December 2020. We defined low disease activity using the lupus low disease activity status (LLDAS), applied the DORIS (Definitions of Remission in SLE) for remission criteria and then assessed flare using the SELENA-SLEDAI Flare Index.
Results Among a total of 185 patients enrolled, 139 exhibited low disease activity or remission with a median follow-up of 29.8 (21.2–35.2) months. The flare rates after achievement of LLDAS, clinical remission and complete remission on treatment were 0.23, 0.12 and 0.1 per patient-year, respectively. In contrast, the flare rate of patients who never achieved remission or LLDAS was 0.49 per patient-year. In patients with LLDAS or remission achievement, multivariate Cox regression analysis showed that lower C3 level at the time of first achieving LLDAS or clinical remission was an independent predictive factor for subsequent flares. Kaplan-Meier curves showed a significantly lower flare-free survival during the subsequent follow-up in patients with GC withdrawal compared with those maintained on a low dose of prednisone (≤7.5 mg/day) (HR=6.94, 95% CI 1.86 to 25.86, p=0.004). However, no significant differences in flare were observed in patients maintained on different low doses of prednisone (>5 mg/day and ≤7.5 mg/day vs >2.5 mg/day and ≤5 mg/day vs >0 mg/day and ≤2.5 mg/day) (p=0.200).
Conclusions Target achievement significantly lowered the rate of subsequent flare, from the perspective of both stricter targets and longer period in targets. C3 level was a strong predictor of flare in patients who have achieved treatment targets. Although GC tapering to minimal doses was feasible, its withdrawal may accelerate the risk of recurrence.
- systemic lupus erythematosus
- treat-to-target
- disease flare
- glucocorticoid tapering
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The principle of treat-to-target (T2T) in SLE was proposed in recent years and remission or low disease activity was recommended as the treatment target. Meanwhile, preventing flare was raised as a realistic goal in the recommendations.
What does this study add?
The incidence of flare after achieving low disease activity and remission was remarkably lower than of patients who never achieved targets.
Achieving targets for ≥50% of observations had a highly protective effect on preventing subsequent flare.
Patients with relatively lower C3 level at the time of target achievement were prone to experience flares even if treatment targets have been achieved.
Prednisone tapering in appropriate patients and at appropriate pace did not increase flare rate, but its withdrawal seemed to accelerate disease occurrence, which needs to be further confirmed with a larger sample size.
How might this impact on clinical practice or future developments?
The results are a reminder that glucocorticoid withdrawal strategy needs to be further investigated to reduce flare rate.
More importantly, the present results further highlight the need to promote the application of T2T/SLE in clinical practice as well as explore concrete implementation strategy for T2T/SLE.
Introduction
SLE is a chronic autoimmune disease with multiorgan involvement. Currently, irreversible organ damage and mortality remain unacceptably high owing to a paucity of advanced therapeutics for effective management of the condition.1 2 Based on this, more advanced management strategies are needed to improve the prognosis of patients with SLE.
The principle of treat-to-target (T2T) in SLE was proposed over 7 years ago with the aim to improve the prognosis of patients with SLE.3 Consequently, several recommendations have been developed by a large task force of experts.4 In these recommendations, prevention of flares is recommended as a realistic target and therapeutic goal since exacerbations of SLE activity may adversely impact long-term patient outcomes, including damage accrual or death. However, studies have shown that a third to two-thirds of all patients with lupus may experience some degree of disease flare.5 Therefore, identifying factors that influence and prevent patients from disease flare is imperative to improve the outcomes.
Among the updated management recommendations for SLE, ‘remission’ or ‘low disease activity’ has been proposed to be the treatment target. Meanwhile, the recommendations proposed the need for chronic maintenance of treatment after achievement of treatment targets, with the need to lower systemic glucocorticoid (GC) to no more than 7.5 mg/day of prednisone followed by withdrawal, when possible.4 To date, only a handful of evidence has demonstrated flare rate after achieving the treatment target as well as the influence of GC tapering and withdrawal on disease flare in patients with ‘remission’ or ‘low disease activity’. In the present study, using a prospective longitudinal SLE cohort, we investigated the frequency and determinants of disease flare, especially GC tapering, in patients who achieved ‘remission’ or ‘low disease activity’.
Materials and methods
Patients
This study enrolled patients in the lupus cohort, a single-centre prospective follow-up cohort at Peking University First Hospital established from January 2017. Subjects in this cohort fulfilled either the 1997 American College of Rheumatology modified classification criteria for SLE6 or the 2012 Systemic Lupus International Collaborating Clinics (SLICC) classification criteria.7 No specific treatment algorithm was predefined and patients were followed up every 3 months, with 6 months as the maximum allowable interval between consecutive visits. Data from all consecutive adult subjects with SLE (≥18 years) with at least two visits in the cohort between January 2017 and December 2020 were included in this study. Patients who only had one visit at recruitment in this cohort were excluded from data analyses.
Data collection
We collected each patient’s demographics, disease duration at recruitment, SLE-related manifestations and organ involvement as defined in the Definitions section on an ‘ever present’ basis. Additionally, information on Systemic Lupus Erythematosus Disease Activity Index-2K (SLEDAI-2K),8 patient global assessment (PGA; scale 0–3)9 and disease flare was collected at each visit. Moreover, the SLICC Damage Index (SDI)10 and the Short Form 36 Health Survey measure of health-related quality of life11 were completed annually. Damage accrual was defined as an increase of >1 in SDI. All data were recorded in a standardised electronic case report form, as part of the Asia Pacific Lupus Collaboration longitudinal cohort study.12 We also collected data on use and doses of GC, hydroxychloroquine (HCQ) and immunosuppressants (IS), as well as laboratory results including complete blood count, renal function, serum albumin, 24-hour urine total protein, C3 and C4, and autoimmune antibodies, at both baseline and each follow-up visit. Baseline was defined as the first recruitment in the cohort. The prescribed GC dosage was converted to prednisone equivalent dose.
Definitions
Cutaneous and mucosal involvement, leucopenia, thrombocytopaenia and serositis were defined according to the 2012 SLICC criteria.7 Lupus nephritis was defined as (1) proteinuria ≥0.5 g/24 hours or ≥3+; (2) cellular casts of red cell, haemoglobin, granular, tubular or mixed; or (3) biopsy-proven nephritis compatible with SLE.7 13 Neuropsychiatric lupus comprised a series of disorders ranging from diverse central nervous system (CNS) disorders including focal CNS syndrome, as well as peripheral nervous system disorders.7 14 15 Diagnosis of autoimmune haemolytic anaemia (AIHA) was based on evidence of reticulocytosis, bilirubinaemia, increased lactic dehydrogenase and positive direct antiglobulin test.16 Pulmonary arterial hypertension (PAH) was defined as a mean pulmonary artery pressure ≥25 mm Hg, with a pulmonary arterial wedge pressure ≤15 mm Hg by right heart catheterisation, or a mean estimated pulmonary systolic pressure ≥50 mm Hg on echocardiography.17 Prednisone maintenance was defined as a specific dose maintained for at least 3 months.
Determination of flare, low disease activity and remission
Disease flare was assessed using the flare definition generated by the Safety of Estrogen in Lupus Erythematosus National Assessment (SELENA) trial named as SELENA-SLEDAI Flare Index.18 19 Mild-to-moderate flare was defined as one or more of the following five features: (1) increase in SELENA-SLEDAI by a score of >3, with a total score of ≤12; (2) new or worsening discoid, photosensitivity, lupus profundus, cutaneous vasculitis, bullous lupus, nasopharyngeal ulcer, pleuritis, pericarditis, arthritis or fever attributable to SLE; (3) an increase in prednisone dose, but ≤0.5 mg/kg/day; (4) initiation of HCQ or non-steroidal anti-inflammatory drugs for SLE disease activity; and (5) a change of ≥1.0 but ≤2.5 in PGA score. Severe flare was defined as one or more of the following five features: (1) SELENA-SLEDAI score >12; (2) new or worsening CNS-SLE, vasculitis, nephritis, myositis, platelet count <60×109/L or haemolytic anaemia (haemoglobin level <70 g/L or a decrease >30 g/L over a 2-week period), requiring doubling or >0.5 mg/kg/day prednisone or an equivalent drug dosage or hospitalisation; (3) any disease activity requiring an increased dose of GC (prednisone >0.5 mg/kg/day or equivalent) or initiation of any new IS, including cyclophosphamide, azathioprine, mycophenolate mofetil, methotrexate, etc; (4) hospitalisation for lupus activity; or (5) a change from baseline in PGA score to >2.5.
Lupus low disease activity status (LLDAS) was defined as SLEDAI-2K ≤4, no activity in any major organ, no new disease activity feature, PGA ≤1, prednisone ≤7.5 mg/day and allowance for maintenance of IS and antimalarials.20 The definition of LLDAS, with a requirement for prednisone dose of 5 mg/day, was as that of LLDAS5 in this study.
DORIS (Definitions of Remission in SLE) was defined as a clinical SLEDAI-2K of 0 (disregarding the serology, including anti-double-stranded DNA (anti-dsDNA) and complements), with PGA <0.5. The criteria had four different definitions, namely clinical remission on treatment (clinical RONT), complete RONT, clinical remission off treatment (clinical ROFT) and complete ROFT. Generally, RONT allows for treatment of patients with a maximum prednisone dose of 5 mg/day and maintenance IS, but ROFT permits neither GC nor IS. Complete remission requires serology (anti-dsDNA and complements) negativity.21
Statistical analysis
Normally distributed continuous variable data were presented as mean±SD, skewed continuous variables as median with IQR and categorical variables as numbers (percentages or proportions). Student’s t-test was used to compare normally distributed continuous variables, Kruskal-Wallis and Mann-Whitney U tests for comparison of non-normally distributed continuous variables, while χ2 test was applied to compare categorical variables across groups. Analysis of flare rate and flare-free survival, during follow-up, was performed using the Kaplan-Meier method with the log-rank test applied for comparisons, and a primary endpoint of disease flare or data censoring. Furthermore, univariate and multivariate Cox proportional hazard models were used to determine variables that were associated with flare after first achievement of LLDAS or clinical RONT. Age at disease onset, gender, education level, disease duration at recruitment, follow-up duration after recruitment, organ involvement presenting ever during the course of disease defined in the Definitions section, scores including SLEDAI and PGA, laboratories including antibodies, complement level and some other parameters at the first visit of achieving LLDAS or clinical RONT, and treatment during follow-up were included in the univariable Cox hazard model. Variables including gender, tertiary education level, all organ involvements, antibodies, prednisone withdrawal and all IS use were analysed as categorical variables. IS use was defined as at least 3 consecutive months of use during the follow-up. Statistically significant variables (p≤0.05) after univariate Cox regression analysis were then included in a stepwise multivariable Cox regression analysis. The effect of GC tapering or withdrawal on subsequent flare was also assessed by multivariate Cox regression analysis by adjusting for age at disease onset, gender, C3, SLEDAI and IS use at the first visit of prednisone tapered to the minimum maintenance dose or withdrawal. Receiver operating characteristic (ROC) curves were generated and used to examine the usefulness of variables in predicting flare.
ROC curves were performed with MedCalc V.11.4.2.0 (MedCalc Software, Ostend, Belgium). All other analyses were performed with STATA V.13.1 for Windows and p<0.05 was considered statistically significant.
Written informed consent was obtained from each participant prior to enrolment.
Patient and public involvement
Neither members of the public nor patients with SLE were involved in the design or conduct of this study.
Results
Characteristics of subjects
A total of 200 patients with SLE were recruited in the prospective cohort between January 2017 and June 2020. Finally, 185 patients were included in this study after excluding 15 who did not return for follow-up after the first visit. A summary of patient characteristics is shown in table 1. Briefly, their mean age at disease onset was 33.5±14.9 years and was dominated by female patients (88.1%). The median (IQR) follow-up duration of 185 patients was 26.2 (12.5–34.5) months, with 142 of them (76.8%) recording a follow-up duration of more than 1 year.
Summary of overall patient characteristics
Cutaneous or mucosal lesions and lupus nephritis were the most common organ involvement (61.6% and 55.7%, respectively) (table 1). The median (IQR) SLEDAI-2K score, PGA and SDI at recruitment were 2 (2–6), 1 (0–1) and 0 (0–1), respectively. Moreover, 182 (98.4%) patients received GC treatment, 171 (92.4%) received HCQ, while 168 (90.8%) received IS for more than 3 months. The median prednisone dose at recruitment was 12.5 (5.0–40.0) mg/day, while the median daily and cumulative prednisone doses were 9.5 (5.2–14.3) mg/day and 6.0 (3.6–9.3) g, respectively, during the follow-up.
At recruitment, 58 (31.4%), 38 (20.5%), 14 (7.6%) and 12 (6.5%) patients fulfilled LLDAS, LLDAS5, clinical RONT and complete RONT, respectively. Furthermore, 81 (43.8%), 70 (37.8%), 56 (30.2%) and 47 (25.4%) patients achieved LLDAS, LLDAS5, clinical RONT and complete RONT at least once after recruitment, respectively. In total, 139, 108, 70 and 59 patients achieved LLDAS, LLDAS5, clinical RONT and complete RONT, respectively. Notably, none of the patients achieved clinical ROFT and complete ROFT during the current follow-up period.
Frequencies of flare during the whole follow-up period
At the end of the study, 73 out of 185 (39.5%) patients experienced 95 episodes of flare, of which 70 (73.7%) and 25 (26.3%) were categorised as mild/moderate and severe flare, respectively. The incidence of flare per patient-year was 0.27. Additionally, the median follow-up duration to the first flare was 9.0 (5.5–15.0) months from recruitment into the study, with 43 (58.9%) patients experiencing the first flare within the first 12 months of follow-up. The median daily dose of prednisone at onset of the first flare was 6.2 (5–10) mg/day, and 28 (38.4%) patients experienced flare at a prednisone dose >7.5 mg/day. Kaplan-Meier curves revealed overall cumulative flare rates of 11%, 23%, 46% and 53% at 6, 12, 24 and 36 months, respectively.
Among 139 patients who achieved either LLDAS or remission at least once, 12.2% (17 of 139) experienced 20 episodes of flare before achieving LLDAS over 6.8±4.3 months of follow-up from recruitment, with a flare incidence of 0.25 per patient-year. After achieving LLDAS, 37 out of 139 (26.6%) patients experienced 54 episodes of flare, with 9 (16.7%) of these episodes severe flare over 20.4±11.2 months of follow-up. Moreover, 25 out of 118 (21.2%) patients experienced 31 episodes of flare after achieving LLDAS5 over 17.8±12.0 months, 8 out of 70 (11.4%) patients had 11 episodes of flare after achieving clinical RONT over 15.3±10.8 months, and 6 out of 59 (10.2%) experienced 8 episodes of flare after achieving complete RONT over 15.0±11.0 months of follow-up period. The corresponding incidences of flare per patient-year were, respectively, 0.23, 0.18, 0.12 and 0.10 after first achieving LLDAS, LLDAS5, clinical RONT and complete RONT. A summary of flare-free survival after first achievement of any of the above targets is shown in online supplemental figure 1, where patients who achieved clinical RONT and complete RONT were likely to have a higher subsequent flare-free survival rate than those who only achieved LLDAS or LLDAS5 (log-rank p=0.003).
Supplemental material
Among 46 patients who never achieved LLDAS or remission over 11.7±9.1 months of follow-up period, 17 experienced 22 episodes of flare, resulting in a flare incidence of 0.49 per patient-year. Notably, 9 (40.9%) of these episodes were severe flare.
Different features of patients with and without subsequent flares among those who have achieved LLDAS or remission at least once
Among 139 patients who achieved LLDAS or remission at least once, 56 (40.3%) experienced subsequent flare (defined as the flare group) and 83 (59.7%) did not (non-flare group) during the whole follow-up. The characteristics of the two groups of patients are presented in online supplemental table 1. Compared with the non-flare group, the flare group were significantly younger at disease onset (30.7±12.4 years vs 37.1±16.4 years, p=0.01), more likely to have positive anti-dsDNA (48.2% vs 33.7%, p=0.047), and had lower levels of C3 (726.7±209.0 mg/L vs 844.9±206.6 mg/L, p=0.001) and C4 (148.7±53.8 mg/L vs 178.3±67.1 mg/L, p=0.005) at recruitment. With regard to treatment, the flare group had a significantly higher cumulative prednisone dose during follow-up (7.9 (5.3–10.2) g vs 5.8 (2.6–9.3) g, p=0.003). Significantly fewer patients achieved prednisone ≤5.0 mg/day in the flare group (73.2% vs 89%, p=0.016). Moreover, we found no statistically significant differences in IS and HCQ use during follow-up between the groups, although IS withdrawal ratio was significantly lower in the flare group relative to the non-flare group (0.0% vs 7.2%, p=0.040). Moreover, the ratios of achieving therapeutic targets, including LLDAS, LLDAS5, clinical RONT and complete RONT, during follow-up, as well as the ratio of target achievement ≥50% of observations, were significantly lower in the flare group than in the non-flare group (all p<0.05).
Supplemental material
Impact of target achievement on subsequent flare during the first year of follow-up
Among 117 patients who completed more than 1 year of follow-up, 32 (27.3%) achieved low disease activity (LLDAS or LLDAS5) for ≥50% of observations in the first year of follow-up, 10 (8.6%) patients achieved remission (clinical or complete RONT) for ≥50% in the first year and 75 (64.1%) patients did not achieve any target for ≥50% in the first year. We generated Kaplan-Meier curves to compare flare-free survival after the first year of follow-up among these three groups of patients and the results showed that patients who achieved the target (either low disease activity or remission) ≥50% of observations in the first year of follow-up had significantly higher subsequent flare-free survival than those who did not achieve any target ≥50% in the first year (log-rank p=0.021; figure 1). However, there was no significant difference between patients who achieved targets of remission and low disease activity (figure 1).

Kaplan-Meier curves showing flare-free survival rates after the first year of follow-up. The comparison was according to the percentage of different target achievements during the first year of follow-up. The three groups were patients who achieved remission on treatment (clinical or complete RONT) for ≥50% of observations during the first year of follow-up, patients who achieved low disease activity (LLDAS or LLDAS5) for ≥50% of observations during the first year of follow-up, and patients who did not achieve any target for ≥50% of observations during the first year of follow-up, respectively. LLDAS, lupus low disease activity status; LLDAS5, lupus low disease activity status with prednisone dose ≤5 mg/day; RONT, remission on treatment.
Determinants of subsequent flare at the timepoint of first LLDAS achievement
Univariate Cox analyses among 139 patients who achieved LLDAS at least once showed that lower C3 levels at the first achievement of LLDAS as well as having PAH during disease course before achieving LLDAS were associated with subsequent flare. In further multivariate hazard model, C3 level at first achievement of LLDAS independently determined subsequent flare (HR=0.77, 95% CI 0.65 to 0.91, p=0.002) (table 2). ROC curve also revealed the ability of C3 level to predict flare at the time of first achieving LLDAS, as evidenced by an Area Under The Curve (AUC) value of 0.63 (95% CI 0.54 to 0.713, p=0.017) (figure 2A), whereas the corresponding optimal cut-off value was ≤787 mg/L, with sensitivity, specificity, positive predictive value and negative predictive value of 60.5%, 64.4%, 44.8% and 77.3%, respectively.
Determinants of flare after achieving LLDAS for the first time by Cox regression analyses
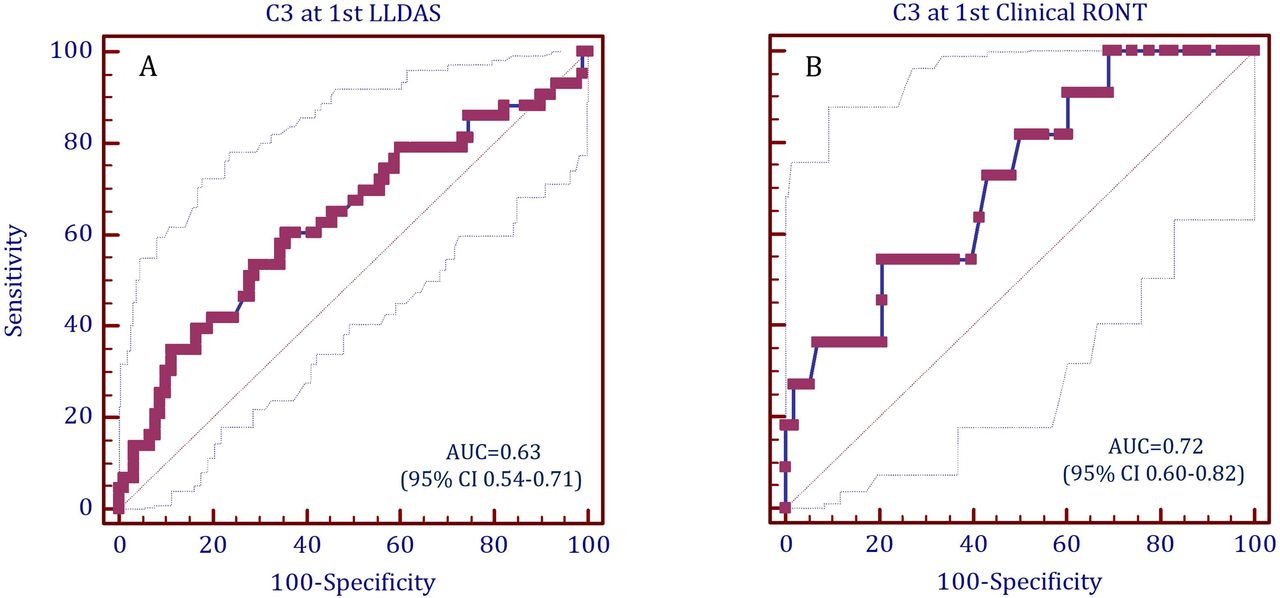
Receiver operating characteristic curves for C3 in predicting subsequent flare (A) at the first visit of achieving LLDAS and (B) at the first visit of achieving clinical RONT. LLDAS, lupus low disease activity status; RONT, remission on treatment.
Determinants of subsequent flare at the timepoint of first clinical RONT achievement
Univariate Cox analyses among 70 patients who achieved clinical RONT at least once showed that lower C3 level at the visit of first achieving clinical RONT as well as having AIHA during disease course before achieving clinical RONT were associated with subsequent flare. In the multivariate hazard model, C3 (100 mg/L) (HR=0.50, 95% CI 0.28 to 0.90, p=0.020) was confirmed to be the only independent determinant of flare after achieving clinical RONT (online supplemental table 2). ROC curve revealed an AUC value of 0.72 (95% CI 0.60 to 0.82, p=0.009) for C3 level at the time of first achieving clinical RONT to predict subsequent flare (figure 2B). The optimal cut-off C3 level was ≤764 mg/L, with sensitivity, specificity, positive predictive value and negative predictive value of 54.5%, 79.3%, 33.3% and 90.2%, respectively.
Impact of different regimens of prednisone tapering on subsequent flare in patients who have achieved LLDAS or remission
Among 139 patients ever in LLDAS or remission, 24 (17.3%) were maintained on a daily prednisone dosage of 5–7.5 mg (>5 mg and ≤7.5 mg) for at least 3 months. On the other hand, 62 (44.6%) and 46 (33.1%) patients had their prednisone dosages reduced to 2.5–5 mg/day (>2.5 mg/day and ≤5 mg/day) and 0–2.5 mg/day (>0 mg/day and ≤2.5 mg/day), respectively, while GC was withdrawn in 7 (5.0%) patients. The median duration for tapering prednisone from 7.5 mg/day to 5 mg/day was 6.2 (3.5–9.0) months, 13.8 (12.0–18.7) months from 5 mg/day to 2.5 mg/day, and 17.3 (16.4–26.9) months from 2.5 mg/day to withdrawal.
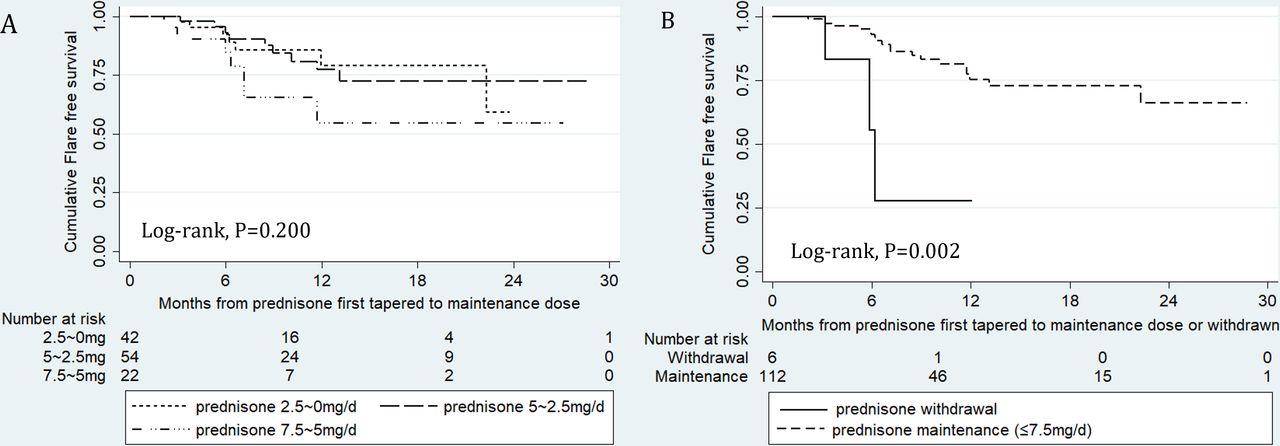
Kaplan-Meier curves showed no significant differences in flare-free survival among patients who achieved LLDAS/remission, however, with three different maintenance regimens of prednisone (5–7.5 mg/day, 2.5–5 mg/day and 0–2.5 mg/day) (log-rank p=0.200; figure 3A). Notably, cumulative flare-free survival was significantly lower in patients with prednisone withdrawal than those maintained on low-dose prednisone (≤7.5 mg/day and >0 mg/day) (log-rank p=0.002; figure 3B) in the subsequent follow-up period. Multivariate Cox regression analyses confirmed the impact of prednisone withdrawal on subsequent occurrence of flare (HR=6.94, 95% CI 1.86 to 25.86, p=0.004) after adjustment for age at disease onset, gender, C3 level, SLEDAI and IS treatment status (online supplemental table 3).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves showing flare-free survival rates in patients after prednisone tapering or withdrawal. (A) The comparison was among patients who maintained prednisone in three different dosages (>5 mg/day and ≤7.5 mg/day, >2.5 mg/day and ≤5 mg/day, and >0 mg/day and ≤2.5 mg/day). (B) The comparison was between patients who were kept on prednisone no more than 7.5 mg/day (>0 mg/day and ≤7.5 mg/day) and those who had prednisone withdrawn.
Discussion
Flare, a common occurrence during the course of SLE, has been associated with a significant increase in clinical and financial burden, as well as organ damage accrual and mortality.22 23 Therefore, prevention of disease flare is imperative to effective management of SLE. To this end, there is a great need to better understand the nature and pattern of flare in SLE and ultimately improve patient outcomes.
The results of the present study showed that almost 40% of patients in our cohort experienced flare, with an incident rate of 0.27 per patient-year during a median follow-up of 26 months. Previous research has reported comparable flare rates (approximately 20%–35% within 1–2 years and 40%–66% within 5–10 years)5 24–26 and a varied incidence (0.1–1.76 per patient-year).24 26–31 More importantly, we investigated the rate of subsequent flare in patients who have achieved LLDAS or remission, which is crucial but has rarely been reported so far.31 Our previous study in 218 newly diagnosed patients showed LLDAS, LLDAS5, clinical RONT and complete RONT were achieved in 87.2%, 73.4%, 67.9% and 43.1%, respectively, with a median follow-up duration of 4.5 (2.4–6.0) years,32 indicating the feasibility of pursuing target attainment. The present study demonstrated that the flare rate after target achievement was significantly lower relative to patients who did not achieve the targets. Specifically, incidences of flare per patient-year were 0.23, 0.18, 0.12 and 0.10 for patients who achieved LLDAS, LLDAS5, clinical RONT and complete RONT, respectively. Meanwhile, the occurrence of severe flare across the study groups also dramatically decreased. Kaplan-Meier survival analyses confirmed that the target achievement of ≥50% of observations during the first year of follow-up reduced and delayed flare in the following 2 years. A previous study has demonstrated the protective role of LLDAS achievement in subsequent flare,20 and one recent research showed that patients in remission exhibited low flare rate even after IS has been withdrawn.33 On the other hand, persistent active disease was confirmed to be a strong predictor of disease exacerbation.34 Taken together, these findings affirm the importance of T2T strategy in the management of SLE. Longer stay in low disease activity or remission status implies better outcomes. Additionally, as shown in online supplemental figure 1, the flare-free survival rates were significantly higher after first achieving clinical or complete RONT than those after first achieving LLDAS or LLDAS5. Nevertheless, figure 1 suggests that, when low disease activity had been maintained for a longer time (≥50% of observations), its value was almost the same as persistent remission in terms of preventing subsequent flare.
Unavoidably, flare happens even when patients have achieved the treatment target, although at a low rate. Therefore, it is important to identify patients at greater risk of flare and follow them up closely. The present study revealed that C3 level at the time of target achievement was a significant determinant of subsequent flares. The performance of C3 in predicting flare reported here is consistent with previous studies. Some studies have shown that complement levels at baseline as well as their decline during follow-up were predictors of subsequent SLE flares.24 30 In the present study, ROC curves showed the cut-off values of C3 for predicting flare at the time of first achieving LLDAS and clinical RONT were 787 mg/L and 764 mg/L, respectively. Nevertheless, the sensitivity of the two cut-off values was relatively low (60.5% and 54.5%, respectively).
The use of GC is a key factor for disease management in SLE. Considering the potential side effects, efforts are needed to minimise the cumulative GC dose. In the present study, we found that patients with flare had a significantly higher cumulative prednisone dose during the whole follow-up duration compared with patients without flare, which might be explained as the consequence of flare. This also hinted at the burden of more GC exposure due to flare.
To date, very limited data are available on GC tapering or withdrawal in patients who have achieved low disease activity or remission. In practice, a goal of prednisone 7.5 mg/day is often set, but a significant proportion of treating physicians are reluctant to continue to further reduce the dose. In the present study, we found that the flare proportion after tapering prednisone to ≤5 mg/day was not significantly higher than those with 7.5–5 mg/day, indicating the feasibility of tapering prednisone to a lower dose than 7.5 mg/day. Zahr et al35 found that 55% of patients in the Hopkins lupus cohort were successfully tapered and maintained on ≤5 mg/day of prednisone for a year which also supported the possibility and attainability of reducing prednisone to a lower dose. In addition, the present study showed the superiority of maintenance with low-dose prednisone to prednisone withdrawal in terms of time to first flare, which reminds clinicians of being vigilant after GC withdrawal even in patients with remission. However, this result, obtained from very limited patients experiencing prednisone withdrawal, needs to be confirmed by further studies. A previous randomised clinical trial from France showed that withdrawal of low-dose prednisone in patients with SLE with a clinically quiescent disease for more than 1 year significantly increased flare compared with those with low-dose prednisone maintenance (27% vs 7%; Risk Ratio=0.2, 95% CI 0.1 to 0.7, p=0.003).36 Conversely, another Italian study revealed that 84.6% patients who attempted discontinuing GC successfully withdrew, accompanied by 23% of subsequent flare rate during a median follow-up of 2 years, which was even lower than those who did not attempt to stop GC.37 Overall, data on GC withdrawal and flare occurrence were limited and hence more prospective randomised control studies are needed in the future to validate these findings.
There were some limitations to this study. First, the sample size was relatively small, especially with regard to the number of patients with GC withdrawal, and the follow-up duration was also relatively short. Second, we found no association between HCQ/IS use and flare, which may be partly due to the high proportion of HCQ and IS use as well as the low withdrawal rate. Third, biologics such as rituximab and belimumab were not included in the analyses due to their extremely rare application. Prospective randomised trials are needed in the future to evaluate the influence of GC withdrawal and use of HCQ, IS and biologics on flare.
Conclusions
Achievement of treatment targets significantly lowered following flare rates and delayed the onset of flare. The longer a patient stays in low disease activity or remission status, the higher the flare-free survival rate they could reach. C3 level at target achievement was a significant and independent factor for predicting subsequent flare. GC tapering in appropriate patients at an appropriate pace did not increase flare rate, but GC withdrawal seemed to accelerate disease recurrence. Future prospective studies with large sample sizes are expected to validate these findings.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Peking University First Hospital Human Research Ethics Committee (project number: 2017(1284)). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The data in this cohort were collected and recorded using the framework of the LLDAS study initiated by the Asia Pacific Lupus Collaboration.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors were involved in drafting the manuscript or revising it critically for important intellectual content, and all authors approved the final version to be published. YH made substantial contribution to study design, data collection, data analysis, interpretation of results and preparation of the manuscript, and takes responsibility for the integrity of the data and the accuracy of the data analysis. ZZ had full access to all the data in the study and takes responsibility for for the overall content as the guarantor of this article. LJ, DG, YF, YG, XZ and GL made substantial contribution to data collection and manuscript revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.