Article Text

Abstract
Objectives To observe if capillary patterns in childhood-onset SLE (cSLE) change over time and find associations between a capillary scleroderma pattern with disease activity, damage or scleroderma-like features.
Methods Clinical and (yearly) capillaroscopy data from a longitudinal cohort of patients with cSLE (minimum of four Systemic Lupus International Collaborating Clinics (SLICC) criteria, onset <18 years) were analysed. Disease activity was measured by Systemic Lupus Erythematosus Activity Index (SLEDAI) and disease damage by SLICC Damage Index. A scleroderma pattern was defined according to the ‘fast track algorithm’ from the European League Against Rheumatism Study Group on Microcirculation in Rheumatic Diseases. An abnormal capillary pattern, not matching a scleroderma pattern, was defined as ‘microangiopathy’.
Results Our cohort consisted of 53 patients with cSLE with a median disease onset of 14 years (IQR 12.5–15.5 years), median SLEDAI score at diagnosis was 11 (IQR 8–16), median SLEDAI at follow-up was 2 (IQR 1–6). A scleroderma pattern (ever) was seen in 18.9%, while only 13.2% of patients had a normal capillary pattern. Thirty-three patients had follow-up capillaroscopy of which 21.2% showed changes in type of capillary pattern over time. Type of capillary pattern was not associated with disease activity. Raynaud’s phenomenon (ever) was equally distributed among patients with different capillaroscopy patterns (p=0.26). Anti-ribonucleoprotein antibodies (ever) were significantly more detected (Χ2, p=0.016) in the scleroderma pattern subgroup (n=7 of 10, 70%). Already 5 years after disease onset, more than 50% of patients with a scleroderma pattern had SLE-related disease damage (HR 4.5, 95% CI 1.1 to 18.8, p=0.034), but they did not develop clinical features of systemic sclerosis at follow-up. Number of detected fingers with a scleroderma pattern was similar between cSLE, juvenile systemic sclerosis and juvenile undifferentiated connective tissue disease.
Conclusion This longitudinal study shows that the majority of capillary patterns in cSLE are abnormal and they can change over time. Irrespective of disease activity, a capillary scleroderma pattern in cSLE may be associated with higher risk of SLE-related disease damage.
- lupus erythematosus
- systemic
- scleroderma
- systemic
- cardiovascular diseases
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
A capillary scleroderma pattern has been observed in patients with SLE which are suggested to be patients with (subclinical) overlapping features of other connective tissue diseases.
What does this study add?
A capillary scleroderma pattern in childhood-onset SLE (cSLE) may be associated with higher risk of SLE-related disease damage.
A capillary scleroderma pattern is persistently observed in patients with cSLE without clinical features of systemic sclerosis at clinical follow-up.
How might this impact on clinical practice or future developments?
As we have shown that capillary patterns can worsen over time, it seems necessary to repeat capillaroscopy during clinical follow-up of patients with cSLE.
Nailfold microangiopathic changes in (c)SLE might be reflecting (early) vasculopathy in SLE and its relation to endothelial dysregulation should be further investigated.
Introduction
Abnormalities in nailfold capillaries of patients with SLE, visualised by capillaroscopy, have been described in literature.1 Two systematic literature reviews showed that these capillary abnormalities mainly consist of capillary haemorrhages and abnormal capillary shapes in adults with SLE but literature in childhood-onset SLE (cSLE) is scarce and mainly inconclusive.1 2 By qualitative analysis, capillary patterns in SLE are mainly described as ‘non-specific changes’ but a scleroderma pattern has also been described in SLE with percentages varying from 3% to 26%.3–9 A scleroderma pattern in nailfold capillaries was first described in patients with systemic sclerosis (SSc) and is characterised by giant capillaries, sometimes in combination with large pathological capillary haemorrhages, loss of capillaries and abnormal capillary shapes with a deterioration of capillary architecture.10 Studies have suggested that patients with SLE with a scleroderma pattern might be patients with (subclinical) overlapping features of other connective tissue diseases (CTDs), such as SSc and dermatomyositis (DM).8 Additionally, the finding of a scleroderma pattern in patients with SLE has been associated with the occurrence of Raynaud’s phenomenon as well as with the presence of anti-ribonucleoprotein (RNP) antibodies. Even more, these patients seem at risk of the development of pulmonary arterial hypertension or pulmonary fibrosis.3 7 8 11 In a cross-sectional study, we previously showed that a scleroderma pattern in nailfold capillaries can be observed in patients with cSLE, characterised by typical SLE symptoms like lupus nephritis, malar rash, serositis, aphtous ulcers, leucopenia, thrombocytopenia, but without any clinical signs of SSc.9
Vasculopathy is an important feature of SSc and this is a dynamic process in this disease changing over time. Changes of the nailfold capillary pattern, both deterioration, improvement as well as complete normalisation have been described during follow-up of patients with SSc.12–16 In one of these longitudinal studies, the appearance of digital ulcers correlated with the type of capillary patterns identified over time.15 Only one study with longitudinal follow-up of nailfold capillaroscopy in patients with SLE is available, describing changes in capillary pattern in cSLE as well as patients with adult-onset SLE. This study suggested that a scleroderma pattern might be considered a red flag for the potential development of scleroderma spectrum disorders such as SSc and mixed/undifferentiated CTD.11 More longitudinal follow-up data are obviously needed for better understanding of the meaning of a scleroderma capillary pattern in SLE.
The primary aims of this longitudinal prospective study are to observe if (ab)normal capillary patterns in individual patients with cSLE change over time and if so, if these (changes in) capillary patterns associate with disease activity and disease damage. Additionally, it is studied if a capillary scleroderma pattern in patients with cSLE indicates an increased risk of development of clinical symptoms for SSc over time. Secondary objective is to compare total finger counts with a scleroderma pattern in cSLE with patients diagnosed with juvenile SSc (jSSc), juvenile DM (JDM) and juvenile undifferentiated CTD (jUCTD) to give more value to this abnormal observation.
Methods
Study design and patients
Between April 2016 and April 2021, patients with systemic autoimmune diseases who visited the (out)patient clinics of the Amsterdam University Medical Centres (UMC) and Leiden UMC were included. Prospective capillaroscopy data were obtained in a cSLE cohort and three disease control cohorts (jSSc, JDM and jUCTD) visiting the (outpatient) clinics. Inclusion criteria for patients with cSLE were diagnosis according to the 2012 Systemic Lupus International Collaborating Clinics (SLICC) classification criteria17 and age of disease onset <18 years old. Patients were diagnosed with JDM and jSSc according to their respective European Alliance of Associations for Rheumatology (EULAR)/American College of Rheumatology (ACR) criteria.18 19 Patients with jUCTD were defined as patients with Raynaud’s phenomenon and anti-nuclear autoimmune antibodies, but without fulfilling the classification criteria for cSLE, JDM or jSSc. Capillaroscopy was part of routine clinical follow-up, demographic and clinical data were recorded from the patient charts. For patients with cSLE who were already diagnosed in the past (before capillaroscopy), retrospective clinical and demographical data were used from the time of diagnosis (autoimmune serology, Systemic Lupus Erythematosus Activity Index (SLEDAI) at diagnosis and type of organ involvement).
All patients with cSLE visiting the (outpatient) clinic in Amsterdam UMC were asked to participate in this longitudinal cohort study, patients from Leiden UMC were asked to participate during two preplanned visits using the same videocapillaroscope from Amsterdam UMC. Patients were excluded if it was impossible to collect images with good quality (due to nailfold skin thickness) or when a patient was too sick to undergo capillaroscopy examination. Demographic and clinical characteristics and disease activity were collected at the study visit. Age, gender, ethnic background, Raynaud symptoms (ever in time) and periungual trauma were noted. Disease onset was defined at the date of first SLE symptom. Disease activity was measured using the SLEDAI20; disease damage by the SLICC Damage Index (SDI).21 Disease activity was also graded by severity: inactive or mild for SLEDAI <3, moderate for SLEDAI between 3 and 6, and severe for SLEDAI >6.
Nailfold capillaroscopy technique and image analysis
Nailfold videocapillaroscopy (NVC) was performed with a ×200 magnification lens from Optilia. Images were collected by two investigators (DS-M or SB, respectively, 6 and 3 years of experience in capillaroscopy examination). Before start of examination, the patients stayed in a room of 20°C–22°C for a minimum of 15–20 min. Patients were in sitting position with the hand on a table at the level of their heart during capillaroscopy examination. A drop of oil was applied to the fingers before examination. In total, eight fingers per patient with cSLE (excluding the thumbs) were examined. Per finger, four images were stored.
Qualitatively, three capillary patterns were described. First, a scleroderma pattern was defined as extremely lowered density (≤3 capillaries/mm) with abnormal shapes or the presence of giants by ‘fast track algorithm’ according to the ‘EULAR Study Group on Microcirculation in Rheumatic Diseases standardised capillaroscopy evaluation chart’.10 22 Second, a capillary pattern was designated as ‘microangiopathy’ (also described as ‘non-specific changes’) if the observed capillary pattern showed abnormal capillary morphology (according to the EULAR study group criteria)22 23 and/or capillary haemorrhages, but did not match the criteria for a scleroderma pattern. Third, a normal capillary pattern was defined if a patient did not have any capillary abnormalities. If the type of capillary pattern in a patient changed over time, the worst pattern was used in analyses. In case of microangiopathy or scleroderma pattern, the number of fingers demonstrating this abnormal pattern was counted.
Statistical analysis
Statistical analysis was performed with IBM SPSS Statistics V.26. Descriptive statistics were reported in terms of percentages, means and SDs or medians and IQRs. For differences of variables between groups, Χ2, Mann-Whitney U and Kruskal-Wallis test analyses were used depending on (distribution, groups and number of categories of) outcome data. Logistic regression was used for occurrence of disease damage and scleroderma pattern as binary outcome data with OR reported with 95% CI. Variables for univariate logistic regression were demographic (age and gender), auto-antibodies anti-RNP and anti-Sm, organ manifestations and SLEDAI at diagnosis. Significant variables from univariate analyses and anti-RNP antibodies, nephritis and neuropsychiatric organ involvement (known to give risk for, respectively, overlap disease or damage from literature7 24) were chosen as covariates for multivariate logistic regression analysis. Longitudinal analysis (with significant variable(s) from univariate analysis) for comparison between different capillary patterns and disease damage as endpoint was performed by Cox regression analysis. P values of <0.05 were considered as statistically significant.
Results
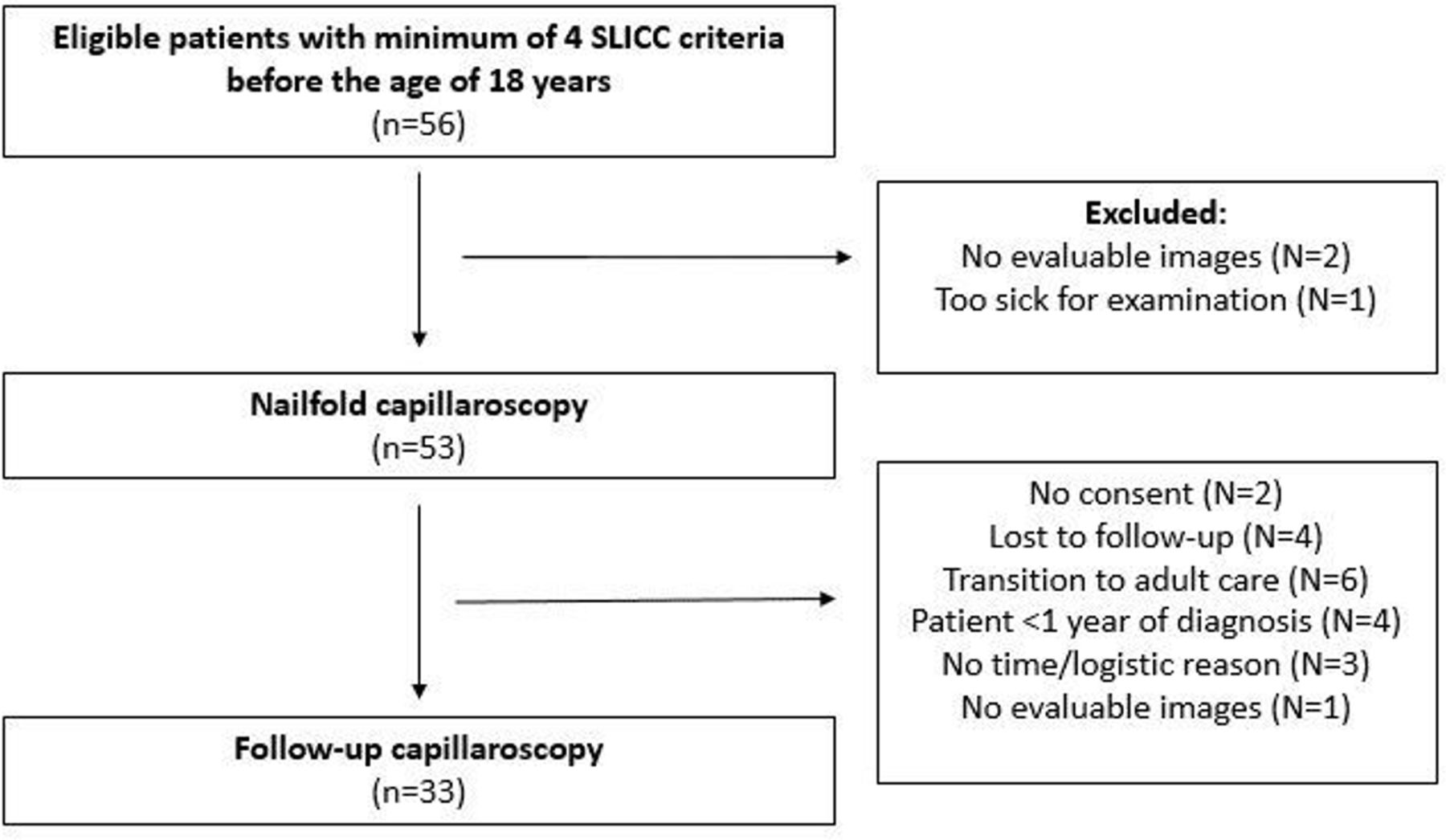
Of 56 eligible patients, capillary images could be analysed in 53 patients with cSLE at the first study visit (figure 1). Thirty-three of these 53 patients (62.3%) had a minimum of one follow-up visit for NVC with a range of 8–60 months after first capillaroscopy. N=14 and n=8 patients, respectively, had two and three follow-up visits for NVC. The reasons for no follow-up NVC (n=20) were: no consent (n=2), lost to follow-up (n=4), transition to adult care (n=6), <1 year of diagnosis (n=4), no time/logistic reason (n=3) and no evaluable images (n=1) (figure 1). Clinical follow-up data in our longitudinal cSLE cohort ranged from 0.5 to 16 years after disease onset. The baseline characteristics are listed in table 1. The patient groups with or without follow-up NVC were comparable for all baseline characteristics.
Demographical variables and clinical characteristics of all patients with cSLE (total and per subgroup with/without follow-up capillaroscopy)

Flow chart longitudinal study cohort of patients with cSLE. cSLE, childhood-onset SLE; SLICC, Systemic Lupus International Collaborating Clinics.
Type of capillary patterns and change in time
At baseline, 13.2% (7 of 53) showed a capillary scleroderma pattern. In total in our cSLE cohort, 10 of 53 (18.9%) of all patients showed a nailfold scleroderma pattern (ever) at minimal one examination, 36 of 53 (67.9%) showed microangiopathy and 7 of 53 (13.2%) a normal capillary pattern. Range for NVC follow-up time was 1–5 years. Figure 2 shows examples of nailfold capillary images with a scleroderma pattern in our patients with cSLE . Observed microangiopathy pattern consisted of abnormal capillary shapes and capillary haemorrhages (without the typical giant capillaries or extremely lowered density ≤3/mm as in a scleroderma pattern).
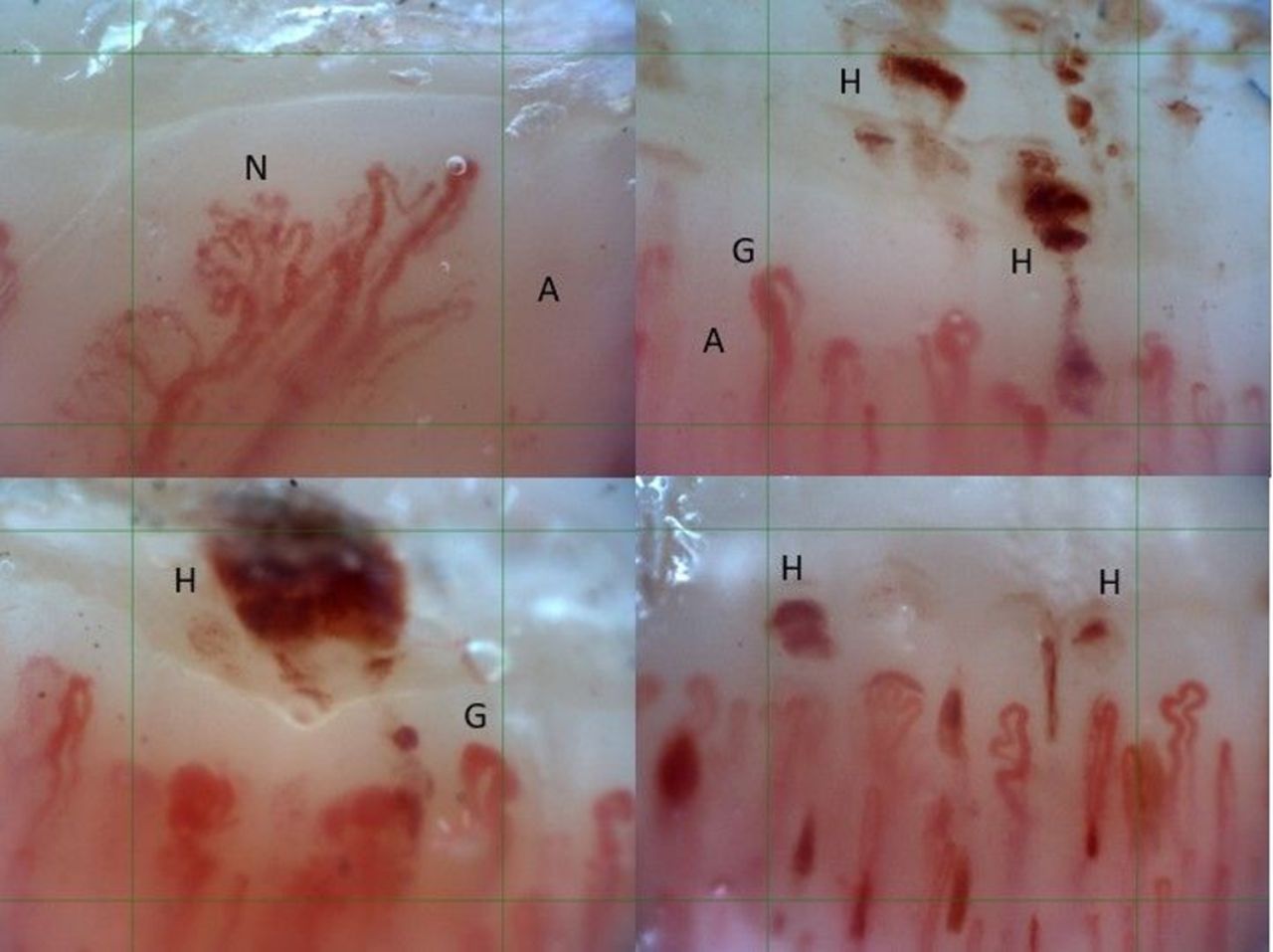
Capillary scleroderma patterns in patients with cSLE showing giant capillaries (G), haemorrhages (H) and neovascularisation (=abnormal shapes) (N) with avascular areas (A). Green grid: 1 mm. cSLE, childhood-onset SLE.
At longitudinal follow-up with NVC assessment, most patients (26 of 33, 78.8%) showed the same capillary pattern as baseline (see online supplemental file 1). Of the seven patients with a baseline capillary scleroderma pattern, in five of seven patients NVC was repeated, which showed that four of five patients (80%) had a persistent scleroderma pattern and one patient (n=1 of 5, 20%) changed to a microangiopathy pattern (with severe active disease). Range of NVC follow-up in these patients with a scleroderma pattern was 14–50 months.
Supplemental material
Of the 39 patients with a baseline microangiopathy pattern, in 24 of 39 patients NVC was repeated. Images from one patient could not be interpreted because of indistinct visualisation of capillaries (poor quality images). Eighteen of these patients (n=18 of 24, 75%) showed persistent microangiopathy and three patients (3 of 24, 12.5%) changed to a scleroderma pattern (two patients with inactive/mild and one with severe disease activity). In three other patients (3 of 24, 12.5%), microangiopathy changed to a normal pattern (two patients with inactive/mild disease and one with moderate disease activity). Range of NVC follow-up in these patients was 9–42 months.
Of the seven patients with a normal capillary pattern, in four of seven patients NVC was repeated. In all patients (n=4 of 4, 100%), this normal pattern persisted (two patients with inactive/mild disease and two with moderate disease activity). Range of NVC follow-up in these patients was 8–22 months.
Mean time between NVC in patients with a change in capillary pattern was 21.1 months (range 9–50 months). Mean time between NVC in patients without any change in pattern was comparable with 15.8 months (range 6–52 months) (see online supplemental file 1). Almost all patients but one (with a worsening of capillary pattern to scleroderma pattern), with and without change in capillary pattern, were on treatment for SLE.
Two patients with a scleroderma pattern had digital lesions at presentation of their disease and thus at time of first capillaroscopy. At follow-up, their digital lesions improved but the capillary scleroderma pattern persisted in both patients.
Capillary patterns and association disease activity/damage
There was no significant difference in ‘SLEDAI at diagnosis’ between patients with different capillary patterns (subanalysis of n=31 treatment-naive patients, Kruskal-Wallis, p=0.18). Overall, patients in follow-up had lower disease activity with median SLEDAI 2 (IQR 1.5–6) than patients at diagnosis with a median SLEDAI of 12 (IQR 8–17). Raynaud’s phenomenon (ever) was equally distributed among patients with different capillaroscopy patterns (Χ2, p=0.26). Anti-RNP antibodies (all subtypes, ever in time) were significantly more detected (Χ2, p=0.016) in the scleroderma pattern subgroup than in the other groups, (in 42.8%, 22.2% and 70% of patients with a normal, microangiopathy and scleroderma pattern, respectively). Of the anti-RNP-positive patients with a scleroderma pattern, 85.7% (n=6 of 7) also showed positive anti-dsDNA antibodies and 71.4% (n=5 of 7) also showed anti-Sm antibodies. The anti-RNP antibodies were directed against 70kD protein in 7 of 18 patients, in the other patients the anti-RNP antibodies were directed against A or C protein. The more severe disease variables nephritis and neuropsychiatric involvement were equally distributed at diagnosis among different capillary patterns (p=0.29 and p=0.44, respectively). By univariate regression analysis, discoid rash (OR 9.3, 95% CI 2.0 to 42.8, p=0.004) and anti-RNP antibodies (OR 6.8, 95% CI 1.5 to 30.9, p=0.013) were significantly associated with the occurrence of a capillary scleroderma pattern. By multivariate regression analysis, this was only seen for discoid rash (OR 5.9, 95% CI 1.2 to 30.2, p=0.033) (see online supplemental file 2).
Supplemental material
At final follow-up, disease damage (as measured by SDI), by univariate regression analysis, was significantly associated with detection of a capillary scleroderma pattern (ever) (OR 7.6, 95% CI 1.6 to 35.9, p=0.01). In this univariate analysis, neuropsychiatric involvement was also significantly associated with the risk of development of disease damage (OR 6.5, 95% CI 1.3 to 33.2, p=0.024) as was discoid lupus (OR 5.1, 95% CI 1.2 to 22.6, p=0.003). By multivariate analysis, only neuropsychiatric involvement was a significant variable for occurrence of disease damage (OR 7.8, 95% CI 1.2 to 15.4, p=0.032) (see online supplemental file 2). Cox regression analysis for occurrence of disease damage between patients with versus without a scleroderma pattern showed a significantly higher hazard for developing disease damage (figure 3, HR 4.6, 95% CI 1.1 to 18.8, p=0.034). In this longitudinal regression model for disease damage, neuropsychiatric involvement was again a significant covariable (HR 8.1, 95% CI 1.9 to 35.8, p=0.005), whereas discoid rash was not (p=0.158). Specific details on disease damage were end-stage renal disease (n=1), growth failure (n=1), extensive scarring in face (n=2), avascular skeletal necrosis (n=2), cognitive impairment/major psychosis (n=1), history of cerebrovascular accident (n=3), loss of digits (n=1), cardiac valve disease (n=1) and seizures requiring therapy for >6 months (n=1). In figure 3 is seen that, between 4 and 5 years after disease onset, half of the patients with cSLE with a capillary scleroderma pattern had irreversible disease damage compared with <10% of patients with cSLE without a capillary scleroderma pattern.

{kind=link}
{kind=link}
{kind=link}
Cox regression analysis for occurrence of disease damage in patients with cSLE with nailfold capillary non-scleroderma pattern (n=23) versus a capillary scleroderma pattern (n=10): HR 4.6 (95% CI 1.1 to 18.8) for scleroderma pattern group, p=0.034. cSLE, childhood-onset SLE.
Patients with a capillary scleroderma pattern did not show criteria to diagnose SSc (puffy hands, sclerodactyly or skin thickening, telangiectasia, interstitial lung disease or digital tip ulcers) or overlap disease during follow-up (table 2).
Clinical characteristics of cSLE-patients (n=10/53) with a capillary scleroderma pattern.
Capillary patterns in cSLE compared with disease controls
At time of first capillaroscopy, the median number of affected fingers was 5 (IQR 3–7) with microangiopathy and 4 (IQR 2–6) with a scleroderma pattern. At second capillaroscopy, the median number of affected fingers was 6.5 (IQR 2.3–8) with microangiopathy and with a scleroderma pattern 6 (IQR 4.5–7). Table 3 shows the number of fingers with a capillary scleroderma pattern in cSLE compared with patient cohorts of JDM (n=12), jUCTD (n=13) and jSSc (n=7). At first NVC and compared with cSLE, the number of fingers with a scleroderma pattern was significantly higher in patients with JDM, but this was not significantly different for patients with jSSc or jUCTD versus cSLE, nor was it different at follow-up.
Different patient groups with a capillary scleroderma pattern and follow-up (FU) data
Discussion
This is the first study reporting longitudinal follow-up data of nailfold capillaroscopy combined with clinical data in cSLE. We showed that nailfold capillary patterns in cSLE can change over time, but these changes were irrespective of disease activity. Strikingly, patients with cSLE with a capillary scleroderma pattern had a higher risk of SLE-related disease damage, although SLEDAI (at baseline nor at follow-up) did not significantly differ between different capillary pattern groups. Subsequently, as we have shown that capillary patterns can worsen over time, it seems necessary to repeat capillaroscopy during clinical follow-up. Furthermore, we are also the first to show that in cSLE, both microangiopathy and a scleroderma pattern, if detected, were observed in the majority of eight examined fingers. At baseline and follow-up, the total number of fingers with a scleroderma pattern, if present in cSLE, was comparable with patients with either jSSc/jUCTD (baseline) and JDM/jSSc/jUCTD (follow-up). This suggests that this finding is not coincidental in cSLE, and in juvenile patients might not only be a specific finding for jSSc.
Anti-RNP antibodies were significantly more detected in patients with cSLE with a capillary scleroderma pattern, but Raynaud’s phenomenon was not, also not during follow-up. A capillary scleroderma pattern has been linked to overlap disease or mixed CTD.25–27 In our study with up to 10 years of clinical follow-up after diagnosis, however, patients with cSLE with a capillary scleroderma pattern did not evolve into a scleroderma overlap disease. Clinical follow-up of these patients included routine medical history, physical examination, laboratory biomarkers and pulmonary function tests (minimal every 2–3 years), cardiac ultrasound (on indication) and pulmonary CT scan for signs of fibrosis (on indication). The mean follow-up was 7 years after diagnosis, one patient was lost to follow-up. Looking at the available anti-RNP titres (in only one-third) in our patients, these titres were quite low and this might subsequently mean that this subgroup of patients with cSLE is not at risk of overlap disease. Interestingly, our data do suggest that patients with cSLE with anti-RNP seem to be a more severe subgroup with more SLE-related disease damage, which was also stated by Dayal and Isenberg.28 On the other hand, a recent study in SSc showed that the presence of anti-RNP antibodies fits with a subgroup of SSc with a better prognostic outcome in terms of survival.29 Thus, the detection of anti-RNP antibodies might have a different prognostic meaning in these different systemic autoimmune diseases or scleroderma spectrum disorders. Most patients with anti-RNP antibodies in the scleroderma pattern group also had multiple, more SLE-specific, auto-antibodies detected, besides other clinical SLICC criteria. This shows that these patients are different than patients with UCTD with only anti-RNP and Raynaud symptoms.
Our finding that a capillary scleroderma pattern is a significant risk factor for irreversible SLE-related disease damage in cSLE is new. Longitudinally, we found that half of the patients with cSLE with a nailfold capillary scleroderma pattern had already irreversible disease damage within only 5 years of diagnosis, meaning that this disease damage develops at a young age, probably around their 20s. We have also shown that this damage could not be predicted by SLEDAI at diagnosis nor by SLEDAI at follow-up, and most of these patients had low disease activity over time. It has been described that patients with SLE with neuropsychiatric involvement and/or nephritis reflect a severe subgroup.24 In our study, this was confirmed for neuropsychiatric involvement, but not for nephritis. Previously, in our cross-sectional study in cSLE, we did find a significant correlation between nephritis and the number of capillary haemorrhages. We have also described that the number of capillary haemorrhages significantly correlated with SLEDAI.9 In this follow-up study, the capillary abnormalities remained visible although patients had low global disease activity or even inactive disease. In addition, patients with low disease activity and a scleroderma pattern at NVC were significantly more at risk of developing disease damage, despite their low disease activity over time. This might imply an ongoing vasculopathy in SLE leading to this disease damage, irrespective of disease activity, as measured by SLEDAI. The disease damage in our cSLE cohort was typical SLE-induced disease damage such as cerebrovascular incidents, seizures (>6 months of treatment), major psychosis, end-stage renal disease and avascular skeletal necrosis and extensive (facial) scarring. Only 7 of 53 patients never used prednisolone as treatment, all others used prednisone at some time in different dosages. As was shown in the specific details of disease damage, two patients suffered from skeletal necrosis and one from growth failure, probably related to chronic prednisolone use. In univariate regression analysis, prednisolone use (ever) was not associated with occurrence of disease damage, but cumulative steroid dose was not calculated in this study. All other patients had specific SLE-related disease damage, which was not related to medication. Also, most disease damage already occurred in the first years after diagnosis.
As in our cross-sectional study,9 microangiopathy with abnormal capillary shapes and high number of capillary haemorrhages was again a predominant and longitudinal persistent finding in this current longitudinal study. As we have shown as well, two types of haemorrhages can be reliably differentiated and reproduced by different raters.30 The same two types of capillary haemorrhages were observed over time in our longitudinal cohort. Other studies have described the capillary abnormalities in (c)SLE as non-specific abnormalities.1 31 32 We hypothesise that the predominant finding of ‘microangiopathy’ in (c)SLE might be capillary leakage and revascularisation and might be due to endothelial dysregulation in SLE, and may not be so non-specific at all. Dysregulation of endothelial cells in SLE has been linked to an increased risk of cardiovascular disease in these patients,33–35 which is one of the most important prognostic factors for mortality in SLE, especially in patients with cSLE.36 Thus, this microangiopathy should be further analysed in this severe and chronic disease and might be a possible new biomarker or a ‘lupus pattern’ reflecting (early) vasculopathy in SLE which warrants additional therapy to prevent future damage.
A limitation of our study is the relatively low number of patients that was included. Although almost all eligible patients from the outpatient clinic could be included, the prevalence of these systemic autoimmune diseases at paediatric age is rare. Another limitation of our study is that not all patients had follow-up visits with capillaroscopy due to several reasons. The typical age of patients at cSLE onset is in their teens which means that patients are relatively soon transferred to adult care after diagnosis, roughly around the age of 18 years. In the Amsterdam UMC, these patients were included in our longitudinal cohort but not all longitudinal capillaroscopy data could be completed. Patients with transition to other hospitals were lost to follow-up.
We conclude that a capillary scleroderma pattern in cSLE did not reflect an SLE subgroup at risk of developing SSc-like symptoms but we suggest that a capillary scleroderma pattern in SLE may be associated with a higher risk of developing SLE-related disease damage.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the ethical committee from the Amsterdam University Medical Centres (Dutch trial register registration no. NL60885.018.17). All patients were coded with a unique study number. For follow-up, according to the Dutch Medical Research Involving Human Subjects Act, informed consent was signed by children from 12 years of age, and/or both parents (if alive and authorised) for children below 16 years old.
Acknowledgments
We would like to thank all patients for (repeated) participation of undergoing capillaroscopy examination. We also thank Professor Dr R ten Cate, Dr LB van der Aa and GE Legger for their help in including patients. We would also like to thank MDJ Wolvers for her advice on statistics for the longitudinal data analyses.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DS-M, JMvdB, VS and TK initiated this study. DS-M, SB, A-N-SR, MG, MM-H, WA, KD, AEH, PHM, MvO, JS, TK and JMvdB recruited patients. DS-M, SB, VS, SSMK, JS and JMvdB were involved in data analysis and writing of the manuscript. All authors were involved in editing of the manuscript and approved this submitted version. DS-M is responsible for overall content and acts as guarantor.
Funding This work was supported by the 'Stichting Steun Emma', a research foundation for clinical research in the Emma Children’s Hospital in Amsterdam (CC401019 to DS-M).
Disclaimer The FWO and Janssen-Cilag NV were not involved in study design, collection, analysis and interpretation of data, writing of the report, nor in the decision to submit the manuscript for publication.
Competing interests VS is a Senior Clinical Investigator of the Research Foundation–Flanders (Belgium) (FWO) (1.8.029.20N). VS is supported by an unrestricted educational chair on systemic sclerosis of Janssen-Cilag NV.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.