Article Text

Abstract
Objective This retrospective analysis evaluated the prognostic value of renal response status 2 years after biopsy-proven lupus nephritis (LN) for the prediction of long-term renal outcomes.
Methods Eligible patients with SLE as per American College of Rheumatology or Systemic Lupus International Collaborating Clinics criteria and biopsy-proven class III, IV, V or mixed LN were identified from the Hopkins Lupus Cohort, and categorised into binary renal response categories (modified primary efficacy renal response (mPERR) or no mPERR at 2 years post biopsy). These categories were defined by a modified version of the Belimumab International Lupus Nephritis Study (BLISS-LN) protocol using urine protein:creatinine ratio (≤0.7 g/day) and estimated glomerular filtration rate (≥60 mL/min/1.73 m2 or ≤20% below the baseline value) criteria. Long-term renal survival (defined as survival without end-stage renal disease (ESRD) or death) and chronic renal insufficiency-free survival were assessed in Kaplan–Meier plots with log-rank test and covariate-adjusted Cox proportional hazards models.
Results Of the 173 eligible patients, 91.3% were female; the mean (SD) age at biopsy was 36.2 (11.8) years. At 2 years post biopsy, 114 (65.9%) patients achieved mPERR. These patients showed a lower risk of ESRD/death and chronic renal insufficiency in the follow-up period (HR (95% CI) 0.33 (0.13 to 0.87), p=0.0255; and HR (95% CI) 0.26 (0.14 to 0.47), p<0.0001, respectively).
Conclusions The 2-year post-biopsy renal response status, defined per 2019-updated BLISS-LN criteria, has prognostic value for long-term renal survival and lower risk of chronic renal insufficiency in patients with LN.
- lupus erythematosus, systemic
- lupus nephritis
- outcome assessment, health care
- autoimmune diseases
Data availability statement
Data are available on reasonable request. Anonymised individual participant data and study documents can be requested for further research from ClinicalStudyDataRequest.com (www.clinicalstudydatarequest.com).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known about this subject?
End-stage renal disease, a condition associated with lupus nephritis (LN), is a strong predictor of poor disease prognosis; as such, the identification of early-stage predictors of long-term renal outcomes would be of value in clinical practice and LN trials.
Renal response is frequently used as a treatment target in LN clinical trials, yet there is no consensus for the definition of these outcome measures, and it is questionable whether they accurately predict long-term renal survival.
What does this study add?
This retrospective analysis of the Hopkins Lupus Cohort evaluated the prognostic value of a defined renal response status assessed at 2 years post-LN diagnosis for the prediction of long-term renal outcomes.
Achieving a modified primary efficacy renal response (mPERR; as defined by the urine protein:creatinine ratio and estimated glomerular filtration rate criteria in the Belimumab International Lupus Nephritis Study (BLISS-LN) study 2 years post biopsy) is significantly associated with better long-term renal survival and chronic renal insufficiency-free survival in patients with LN.
How might this impact on clinical practice or future developments?
The modified BLISS-LN primary endpoint mPERR has prognostic value for long-term renal outcomes of patients with LN.
Introduction
Lupus nephritis (LN) is a common and severe manifestation of SLE that is present in 38% of patients at SLE diagnosis, and occurs in as many as 70% of patients with SLE during the course of their disease, depending on factors such as age, gender, race and ethnicity.1–3 LN accounts for substantial morbidity and mortality in patients with SLE.4 5 One study reported that patients with SLE and LN had an approximately threefold higher standardised mortality ratio than patients with SLE without LN (6.8 vs 2.4).6 End-stage renal disease (ESRD) is a condition that ~22% to 26% of patients develop within 15 years after LN diagnosis and is a strong indicator of poor prognosis.7 8 Identifying early-stage predictors of long-term renal outcomes would allow for optimisation of LN treatment in clinical practice and a consistent and accurate evaluation of treatments in LN clinical trials.
Renal response is a frequently used treatment target in LN clinical trials. Most studies have used proteinuria level and glomerular filtration rate (GFR) in their definition of renal response; however, there is no consensus on the precise combination and threshold levels for these outcome measures.1 9 10 As a result, the renal response endpoints used in LN clinical trials lack uniformity and it is questionable whether they accurately predict long-term kidney survival.1 9 11
A retrospective analysis of real-world data from the Hopkins Lupus Cohort by Davidson et al examined the renal response definition used in the Efficacy and Safety of Belimumab in Patients With Active Lupus Nephritis (BLISS-LN; GSK Study BEL114054; NCT01639339) clinical trial.12 The Hopkins Lupus Cohort is a prospective, longitudinal, real-world study of lupus activity, organ damage and treatment of patients with SLE, which began in 1987.13 Within this analysis, the renal response definition was largely aligned with the BLISS-LN primary endpoint at that time (ordinal response: complete, partial, no response) but with a modification to exclude urinary sediment.14 This response category assessed at 2 years post biopsy was found to be a predictor of long-term (up to 25 years) renal outcomes.12
Several studies have shown that a decrease in proteinuria to <0.7–0.8 g/day is a reliable predictor of long-term renal survival.15–18 In addition, estimated GFR (eGFR) <60 mL/min/1.73 m2 is considered a predictor of poor renal prognosis.19 In contrast, urinary sediment can have confounding effects on the evaluation of renal response.20 Consequently, the BLISS-LN primary endpoint was modified before unblinding in 2019 to a binary ‘primary efficacy renal response’ (PERR) at 2 years post biopsy.21 22 To harmonise with growing evidence on predictors of long-term renal outcomes, PERR was defined as urine protein:creatinine ratio (uPCR) ≤0.7 g/day, eGFR of ≤20% below the baseline value or ≥60 mL/min/1.73 m2, and no use of rescue therapy for treatment failure.14
This study aimed to assess the prognostic value of a modified version of the BLISS-LN study PERR endpoint (mPERR) for predicting real-world, long-term renal survival, and chronic renal insufficiency-free survival of patients with LN in the Hopkins Lupus Cohort. For the mPERR endpoint, mandatory tapering of rescue therapy was removed as a requirement, and eGFR was compared with the GFR value at biopsy, due to the real-world nature of this study.
Materials and methods
Study design
This was a retrospective analysis nested within the prospective, longitudinal Hopkins Lupus Cohort study. Data were collected in this cohort at each outpatient visit (at least quarterly) and included SLE clinical activity indices, laboratory data and treatment (medication and dose).13 The Hopkins Lupus Cohort study was approved on an annual basis by the Johns Hopkins University School of Medicine Institutional Review Board (Research Project Notification: NA_00039294), and all participants gave informed consent.
Eligible patients were identified from cohort records and patients’ renal status were categorised retrospectively into binary categories (mPERR (‘responders’) or no mPERR (‘non-responders’)) at 2 years post-biopsy date, based on laboratory data available in the cohort records.
Patients were followed up from 2 years post biopsy until censoring due to an outcome event (ESRD, death or chronic renal insufficiency), loss to follow-up or the end of study (December 2013). Each visit included measurements of serum creatinine and urinary protein (uPCR, 24-hour urinary protein (g/24 h) or urine protein semi-quantitative dipstick) levels. Due to the real-world setting, the timing of renal function assessments varied. Thus, a ±3-month window for inclusion of laboratory data was defined around each interval date (ie, baseline, 0.5, 1, 2, 3, 4 and 5 years post biopsy). Baseline was defined as the date of biopsy. An overview of the study design is shown in figure 1.
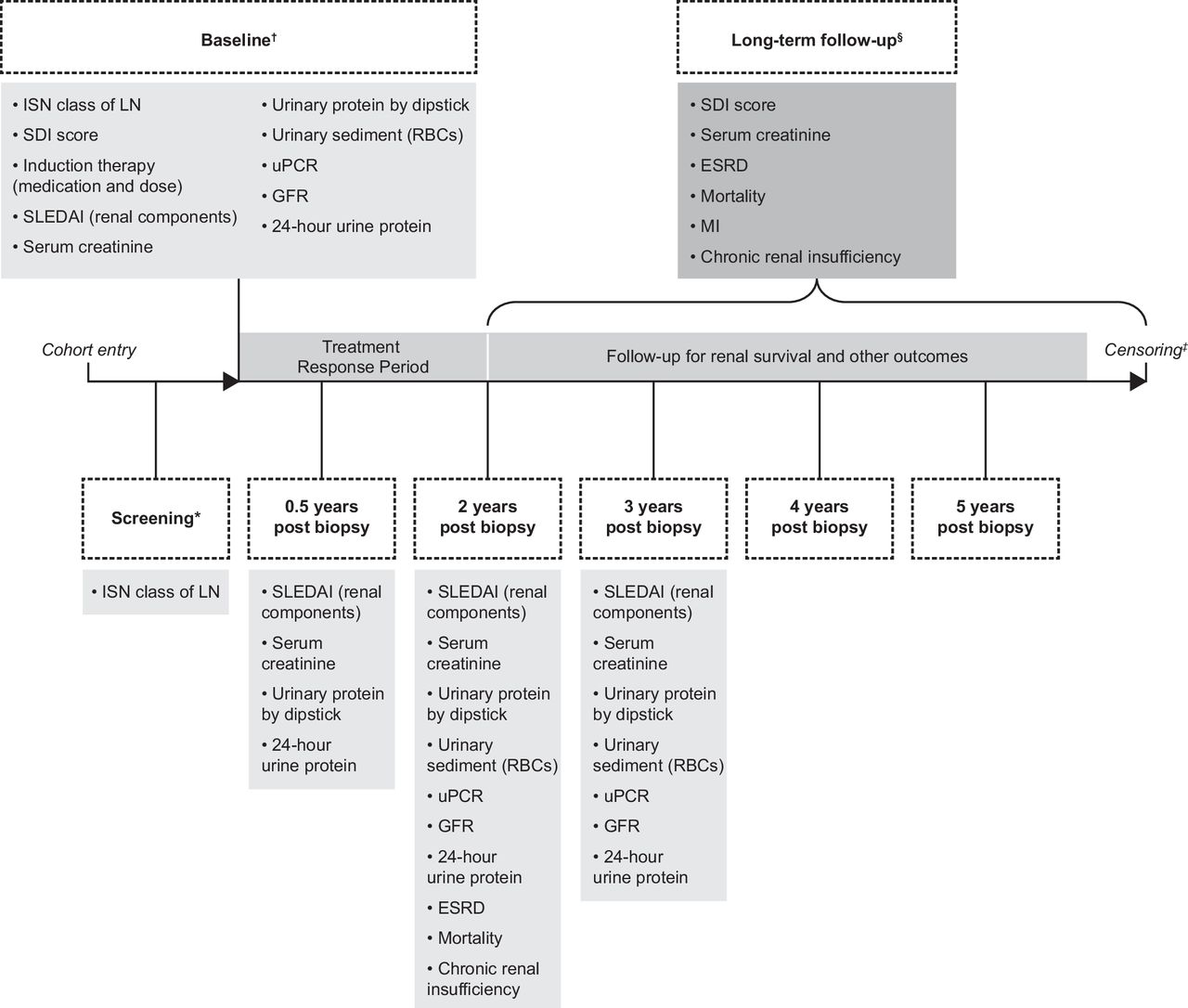
Study design. *Screening defined as cohort entry date to biopsy date. †Baseline defined as the closest date to the biopsy date within a period of 3 months prior to biopsy to 3 months post biopsy. ‡Censoring occurred due to outcome event, loss to follow-up or end of study dataset (December 2013). §From 2 years post biopsy until censoring. GFR, glomerular filtration rate; ISN, International Society of Nephrology; LN, lupus nephritis; MI, myocardial infarction; RBC, red blood cell; SDI, SLICC/ACR Damage Index; SLEDAI, Systemic Lupus Erythematosus Disease Activity Index; uPCR, updated mPERR proteinuria component.
Patients
Eligible patients had SLE as per revised American College of Rheumatology (ACR)23 or Systemic Lupus International Collaborating Clinics (SLICC)24 criteria and International Society of Nephrology and the Renal Pathology Society (ISN/RPS) 2003-defined class III, IV, V or mixed lupus glomerulonephritis25 proven by biopsy results. Patients were ≥18 years of age at LN diagnosis (biopsy date) and made at least one visit to the Johns Hopkins Lupus clinic in both the 3 months following biopsy and the 2 years following immunosuppressive (IS) therapy (cyclophosphamide, mycophenolate mofetil, or azathioprine) initiation.
Patient records were required to contain sufficient data within the baseline (biopsy date) and 2 years post-biopsy windows to assess their renal response status at 2 years post biopsy. ‘Sufficient’ was defined as ≥1 serum creatinine measurement, plus either (1) measurement of the uPCR, (2) 24-hour urine protein measurement or (3) urine dipstick measurement. If multiple measures were available, uPCR was given preference over a 24-hour urine protein measurement as the former was done routinely, and the 24-hour urine protein measurement was preferred over a urine protein semi-quantitative dipstick score.
The presence of ESRD, defined as having received renal replacement therapy (dialysis or transplantation), at biopsy precluded participation.
Renal response
Binary mPERR status at 2 years post biopsy (responder or non-responder) was defined as an eGFR ≤20% below the baseline value or ≥60 mL/min/1.73 m2, and uPCR ≤0.7 (or 24-hour urine protein ≤0.7 g/24 h if uPCR data were missing, or urine protein semi-quantitative dipstick score ≤1 (≤30 mg/dL) if both uPCR and 24-hour urine protein data were missing (a proxy quantitative measure created based on the published literature26)).
Endpoints
The primary endpoints were long-term renal survival, defined as the absence of ESRD or death between 2 years post biopsy and censoring. Secondary endpoints included (1) incidence of chronic renal insufficiency defined as occurrence of kidney damage or a GFR <60 mL/min/1.73 m2 recorded on ≥2 consecutive visits (≥3 months apart); (2) eGFR over time calculated from serum creatinine measurement using the Cockcroft-Gault formula27; and (3) serum creatinine over time as measured during visits at 2, 3, 4 and 5 years post biopsy.
The proportion of mPERR responders who went on to achieve a modified complete renal response, defined as an eGFR >90 mL/min/1.73 m2, and a uPCR of <0.5 (or 24-hour urine protein <0.5 g/24 h or urine protein semi-quantitative dipstick score ≤1 (≤30 mg/dL)), was also described at 3, 4 and 5 years post biopsy.14
Analysis
Descriptive analyses were reported in terms of mean, median and SD for continuous variables, and as proportions for categorical variables.
The association between mPERR status at 2 years post biopsy and renal survival and chronic renal insufficiency-free survival post 2 years of follow-up was analysed using Kaplan–Meier plots with log-rank tests. The association between mPERR status at 2 years post biopsy and the risk of ESRD or death, or developing chronic renal insufficiency was investigated via Cox proportional hazards models, using univariate models, as well as covariate-adjusted models from the previous study.12
Results
Study population
Overall, 173 patients from the Hopkins Lupus Cohort met the eligibility criteria. Table 1 provides an overview of the baseline characteristics. The mean (SD) age at biopsy was 36.2 (11.8) years and 91.3% were female. Patients were distributed across LN ISN/RPS classes; most patients (82.7%) had received IS therapy in the 3 months before or 3 months after biopsy. Of the 173 patients, 114 (65.9%) were mPERR responders and 59 (34.1%) were non-responders at 2 years post biopsy. The median follow-up time of the cohort was approximately 6 years.
Patient demographics and baseline clinical characteristics
Association between mPERR status at 2 years post biopsy and renal survival during follow-up
Kaplan–Meier analysis and associated log-rank test showed that there was a statistically significant increased likelihood of renal survival among mPERR responders than non-responders (p=0.0057; figure 2A). Furthermore, in the Cox proportional hazard model, after adjusting for SLICC/ACR Damage Index (SDI) and hypertension, mPERR responders had a statistically significant lower risk of ESRD or death than non-responders (HR (95% CI): 0.33 (0.13 to 0.87); p=0.0255; table 2).
Multiple Cox proportional hazards models (adjusted for covariates identified by Davidson et al12) for the association between mPERR category at 2 years post biopsy and ESRD or death and renal insufficiency during follow-up
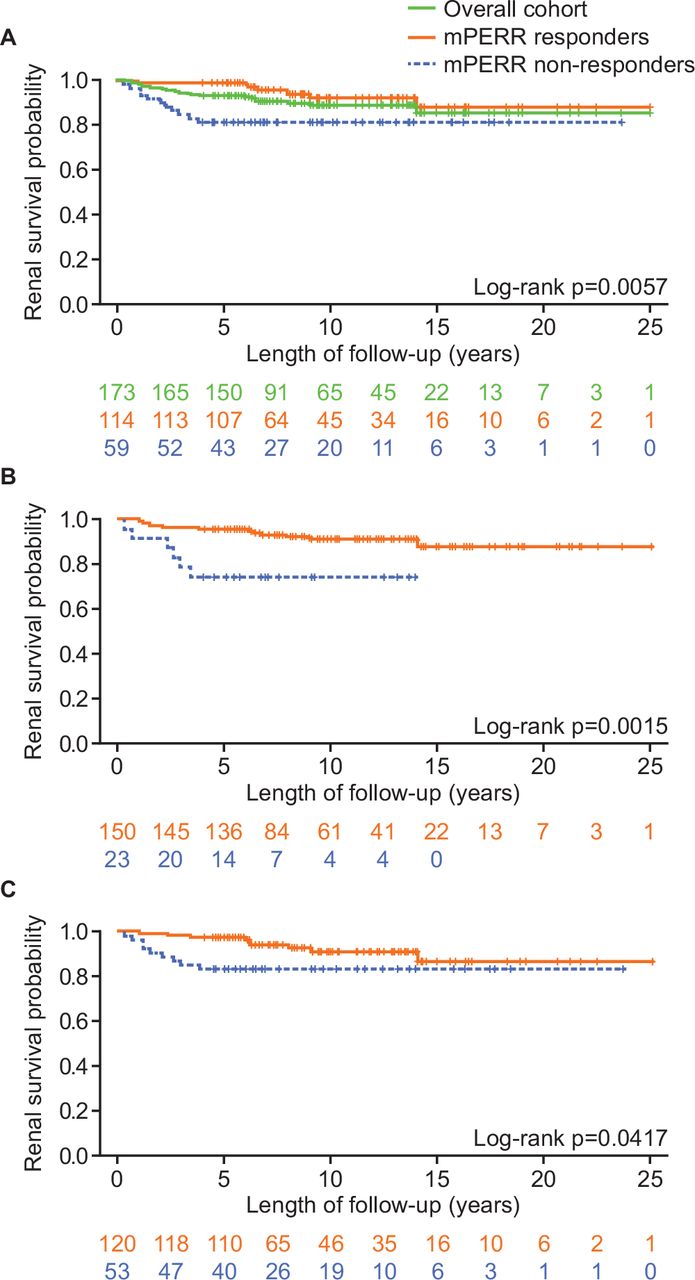
Long-term renal survival of responders and non-responders with regard to (A) mPERR overall; (B) GFR component of mPERR*; (C) proteinuria component of mPERR. *Reduced length of follow-up for mPERR GFR no response is due to no ESRD/mortality events occurring after this time point. ESRD, end-stage renal disease; GFR, glomerular filtration rate; mPERR, modified primary efficacy renal response.
The components of mPERR categorisation (ie, GFR and proteinuria levels) were explored individually. Renal survival was significantly more likely in patients with GFR ≤20% below baseline or ≥60 mL/min/1.73 m2 at 2 years post biopsy than in patients who did not meet this criterion (p=0.0015; figure 2B). Regarding proteinuria, renal survival was significantly more likely for patients with uPCR ≤0.7 (or 24-hour urine protein ≤0.7 g/24 h, or urine protein semi-quantitative dipstick score ≤1 (≤30 mg/dL)) than patients who did not meet this criterion (p=0.0417; figure 2C). Over the course of 5 years of follow-up, the proportion of patients with a GFR ≥60 mL/min/1.73 m2 was consistently greater, and the proportion of patients with serum creatinine ≥1.0 mg/dL was consistently lower, in mPERR responders compared with mPERR non-responders (table 3).
GFR and serum creatinine levels during follow-up period by mPERR status
Association between mPERR status at 2 years post biopsy and chronic renal insufficiency during follow-up
Kaplan–Meier analysis and associated log-rank test showed that responders were significantly less affected by chronic renal insufficiency than non-responders (p<0.0001) (figure 3). In addition, the Cox proportional hazard model, after adjusting for age at biopsy and hydroxychloroquine use between baseline and 2 years post biopsy, showed that responders were at a significantly lower risk of chronic renal insufficiency than non-responders (HR (95% CI): 0.26 (0.14 to 0.47); p<0.0001; table 2).

{kind=link}
{kind=link}
{kind=link}
Long-term renal insufficiency-free survival of responder and non-responders. mPERR, modified primary efficacy renal response.
Association of complete renal response over time with mPERR
The majority (n=94/114; 82.5%) of mPERR responders also met the criteria for complete response at 2 years post biopsy. Eighty-two (71.9%) mPERR responders met complete response status at 3 years, 63 (55.3%) at 4 years and 51 (44.7%) were in complete response at 5 years post biopsy.
Of the 20 mPERR responders who did not meet the complete response criteria at 2 years post biopsy, 7 (35%), 7 (35%) and 3 (15%) patients went on to achieve complete response at 3, 4 and 5 years, respectively. The cumulative proportion of responders who achieved complete response over 5 years post biopsy was 8 (40%).
Discussion
This study investigated the use and prognostic value of a modified version of the updated primary endpoint of BLISS-LN (PERR at 2 years post biopsy) for long-term renal survival and renal function, as applied to the Hopkins Lupus Cohort. Patient classification into binary categories of mPERR or no mPERR at 2 years post biopsy showed clinical relevance for the prediction of long-term renal outcomes.
Consistent with previous results, patients who showed mPERR at 2 years post biopsy were significantly more likely to achieve long-term renal survival and maintenance of renal function than those who did not.12 When analysing the individual components of mPERR, the association between proteinuria levels and renal survival was consistent with the findings of previous studies that reported proteinuria reduction (<0.7–0.8 g/day) 1 year after LN treatment initiation to be a strong predictor of long-term renal prognosis.15 18 Although the results of these studies were primarily from Caucasian patients, similar findings were observed in more diverse cohorts of patients with LN.16 28 The outcomes predicted by the updated mPERR proteinuria component (uPCR ≤0.7, or 24-hour urine protein ≤0.7 g/24 h, or urine protein semi-quantitative dipstick score ≤1 (≤30 mg/dL)) in this current study support previous indications that lower proteinuria thresholds (<0.8 g/day at 1 year) are a strong predictor of long-term renal outcomes.15 16 18 In addition, mPERR responders were also less likely to develop chronic renal insufficiency in the long term (up to 25 years of follow-up) than non-responders. The consistency of these findings with previous data suggests that this target threshold for proteinuria (uPCR ≤0.7 g/day) is likely to be generalisable for prediction of renal outcomes.
The modified BLISS-LN complete renal response criteria, defined as an eGFR >90 mL/min/1.73 m2 and a uPCR of <0.5 (or 24-hour urine protein <0.5 g/24 h or urine protein semi-quantitative dipstick score ≤1 (≤30 mg/dL)), was more stringent than mPERR, and a lower proportion of patients in the Hopkins Lupus Cohort study met this definition of renal response (40.9%) compared with mPERR (67.3%).12 14 A proteinuria cut-off of <0.5 g/day may be too restrictive to predict positive renal outcomes, as reported in the literature.15 28
We found that the majority of mPERR responders met the criteria for complete renal response at 2 years post biopsy. Although the complete renal response criteria in the current study was similar to the outcome criteria of other LN trials, half of the mPERR responders who did not meet the complete renal response criteria at 2 years post biopsy did so in the 5 years of follow-up. This could support the hypothesis that the complete renal response criteria were too stringent and may have excluded some patients who would subsequently show long-term clinical improvements.
Progression of chronic renal damage in LN results from a gradual loss of nephrons; this can result in a substantial decrease in GFR, which may serve as a marker for long-term negative outcomes.19 Patients in the current study with no GFR worsening >20% below baseline (or ≥60 mL/min/1.73 m2) had significantly greater renal survival at 2 years post biopsy than those who did not, indicating that this threshold for GFR is useful for the prediction of long-term renal outcomes. This is supported by previous studies that established GFR <60 mL/min/1.73 m2 as a marker of renal function in chronic kidney disease, and as a risk factor of poorer long-term renal prognosis due to disease complications, more rapid progression to ESRD and death.19 29 In the current study, the mean GFR over the 5 years of follow-up was higher in mPERR responders than in non-responders, and mPERR responders maintained lower serum creatinine values over 5 years of follow-up than non-responders.
With documentation of patient details and outcomes over a relatively long follow-up, the Hopkins Lupus Cohort is one of the most characterised lupus cohorts globally. While this rich source of real-life data from a community cohort is suitable to assess the long-term clinical relevance of renal response status at 2 years post biopsy, certain limitations of the present analysis are apparent. First, as only data from patients presenting to Johns Hopkins University (ie, from the Baltimore area) were analysed, this study population may not be representative of the wider demographic makeup of the US population and treatment practices. For example, half of the study population were of Black African ancestry, and the generalisability of the results to a wider LN population may be somewhat limited. The study population may also differ from clinical trials, which often require eligible patients to have proteinuria >1 g/24 h.30 31 In addition, as the Hopkins Lupus Cohort is centered in an outpatient clinic, some patients had baseline proteinuria and initial IS therapy during a previous in-patient admission prior to cohort entry, such that the renal measures could be after treatment onset. IS pretreatment may have also been for non-renal involvement, which may have introduced bias. Missing data regarding IS use within 3 months of baseline also limited interpretation of the results. Misclassification may also have occurred through the retrospective application of clinical trial endpoint criteria to real-world data. Fully quantitative proteinuria measures were also missing for some patients prior to the adoption of uPCR; semi-quantitative urine dipstick measures were available for 99.4% of patients. However, changes over time in the availability of proteinuria metrics within the cohort may have also introduced bias. Proteinuria measurement data were selected using a hierarchical approach, with uPCR as the first choice as it was the most commonly used, followed by 24-hour urine protein (g/24 h). For patients missing these measures, semi-quantitative urine dipstick measures were used, and proxy quantitative measures were created based on the published literature.26 These measures can be limited by multiple confounders (eg, urine concentration and pH) and the semi-quantitative nature of the urine dipstick. Finally, the decrease of patient numbers over time (particularly beyond 10 years) due to censoring limits the strengths of the data presented in the Kaplan–Meier plots.
Conclusions
The data from this study suggest that the mPERR status (responder vs non-responder) at 2 years post biopsy has prognostic value for the long-term renal outcomes of patients with LN and support the validity of mPERR as an endpoint when used in real-world studies. However, further observational studies in larger multicenter LN cohorts are required to confirm these findings.
Data availability statement
Data are available on reasonable request. Anonymised individual participant data and study documents can be requested for further research from ClinicalStudyDataRequest.com (www.clinicalstudydatarequest.com).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Johns Hopkins University School of Medicine Institutional Review Board (Research Project Notification: NA_00039294).
Acknowledgments
The authors thank Kerry Gairy for reviewing the data. Medical writing support was provided by Julia Eckhoff, PhD, and Liam Campbell, PhD, of Fishawack Indicia Ltd, UK, and was funded by GSK. The authors would like to thank the participating patients and their families, clinicians and study investigators.
References
Footnotes
Contributors DWG and MP acquired the data. SC, QF, YG, AM, and DAR designed the experiments and analysed the data. PJ analysed the data. All authors contributed to the development of the manuscript. PJ is the guarantor for this publication.
Funding This work was funded by the National Institute of Health (NIH grant R01-AR069572) and GSK (study number 213039).
Competing interests SCB and AM were employees of GSK at the time of the study. QF, YG, PJ and DAR are employees of GSK and hold shares in the company. DWG has nothing to disclose. MAP received research funding from GSK.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.