Article Text

Abstract
Cytokine autoantibodies, particularly those directed to type I interferon (T1IFN), have been reported to portend an increased risk of severe COVID-19. Since SLE is one of the conditions historically associated with T1IFN autoantibodies, we sought to determine the prevalence of cytokine autoantibodies in our local cohort of 173 patients with SLE prepandemic and intrapandemic, of which nine had confirmed exposure to SARS-CoV-2. Autoantibodies to 16 different cytokines, including T1IFN, were measured by an addressable laser bead immunoassay. None of the 9 patients with confirmed exposure to SARS-CoV-2 had autoantibodies to T1IFN and none had severe COVID-19 symptoms, necessitating hospitalisation. Hence, we could not confirm that TIIFN autoantibodies increase the risk for severe COVID-19. In addition, the cytokine autoantibody pattern did not differ between those with and without evidence of SARS-CoV-2 exposure.
- Autoantibodies
- Autoimmunity
- COVID-19
- Lupus Erythematosus, Systemic
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Recent evidence indicated that the presence of neutralising anti-type 1 interferon (T1INF) antibodies is associated with severe COVID-19 outcome. Previous studies reported antibodies to a wide range of cytokines in SLE, including T1INF.
We sought to determine the prevalence of cytokine antibodies including anti-T1INF in patients with SLE, exposed versus unexposed to COVID-19.
What does this study add?
In a cohort of patients with SLE examining prepandemic and intrapandemic antibodies to cytokines, none of the COVID-19 exposed patients (although all had a mild infectious course) had antibodies to T1INF compared with 3.7% of those without COVID-19 exposure (not statistically significant).
Autoantibodies to other interferons and cytokines were not associated with exposure to SARS-CoV-2.
How might this impact on clinical practice?
Measurement of antibodies to T1INF in SLE may be an important biomarker identifying SLE at risk of severe COVID-19. A larger study including patients with SLE with a more severe COVID-19 course and the impact of neutralising autoantibodies and vaccines are needed.
Introduction
Autoantibodies directed to cytokines, including type I interferon (T1IFN), have been reported in a wide variety of infectious and autoinflammatory diseases including in up to 27% of patients with SLE.1–3 A remarkable finding reported during the SARS-CoV-2 pandemic was that pre-existing autoantibodies directed to T1IFN were associated with a higher risk of developing severe COVID-19.4–6 Given the importance of IFN in host viral defences,7 these observations raised the question of whether anti-T1IFN autoantibodies are associated with an increased risk of severe COVID-19 in SLE, a disease in which T1IFN plays a key role.8
Methods
We examined the prevalence of cytokine autoantibodies in prepandemic and intrapandemic sera from a SLE cohort using a commercially available 15-PLEX anticytokine array (Luminex Corporation, Austin, Texas, USA), which included detection of IgG autoantibodies directed to IFN-gamma (γ), IFN-beta (β), B cell activating factor (BAFF)/B lymphocyte stimulator (Blys), tumour necrosis factor alpha (α), granulocyte colony stimulating factor, interleukin (IL)-1α, IL-6, IL-8, IL-10, IL-12 (p40), IL-15, IL-17A, IL-17F, IL-18 and IL-22. In addition, autoantibodies to IFN-α (IFN-α2b) were detected by an addressable laser bead immunoassay (ALBIA) using the full-length purified human protein (Abcam, Cambridge, UK) following protocols as previously published.9 A cut-off of 500 median fluorescence intensity was established at two standard deviations above the mean of age-matched healthy controls, following the requirements for validation of laboratory tests in the accredited laboratory (MitogenDx) that performed these tests. SLE-related autoantibodies (anti-double stranded DNA (dsDNA), anti-Smith (Sm), anti-U1-ribonucleoprotein (RNP), anti-ribosomal P, anti-SSA/Ro60, anti-Ro52/(tripartite motif containing-21) TRIM21 and antichromatin) were detected in the prepandemic and intrapandemic sera by commercially available multianalyte immunoassays as previously published.9 10 Prepandemic serum samples from the SLE cohort were biobanked prior to 01 January 2020 and intrapandemic samples were collected from 15 March 2020 to 31 January 2021; all patients were unvaccinated at the time of serum collection.11 All samples were tested for SARS-CoV-2 antibodies using an ELISA measuring IgA and IgG antispike 1 (S1) protein (Euroimmun AG, Lübeck, Germany) and an assay detecting IgG antibodies to nucleocapsid (N), S1 receptor binding domain (RBD) and S1 (XMAP: Luminex Corporation, Austin, Texas, USA).11 RT-PCR tests were performed if clinically indicated and results collected retrospectively through to 31 January 2021.
Cytokine autoantibodies were compared between patients with SLE with SARS-CoV-2-positive serology and/or RT-PCR confirmed SARS-CoV-2 infection (SARS-CoV-2 serology methods previously published)10 vs the remaining cohort using a χ2 test. The Bonferroni method was used to correct for multiple comparisons (17), with a corrected α of 0.0029 being considered statistically significant. Potential associations between each cytokine autoantibody and each SLE-related autoantibody in the prepandemic and intrapandemic periods were assessed using a χ2 test, with a Bonferroni corrected α of 0.00045 being considered significant to account for the 112 comparisons.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Results
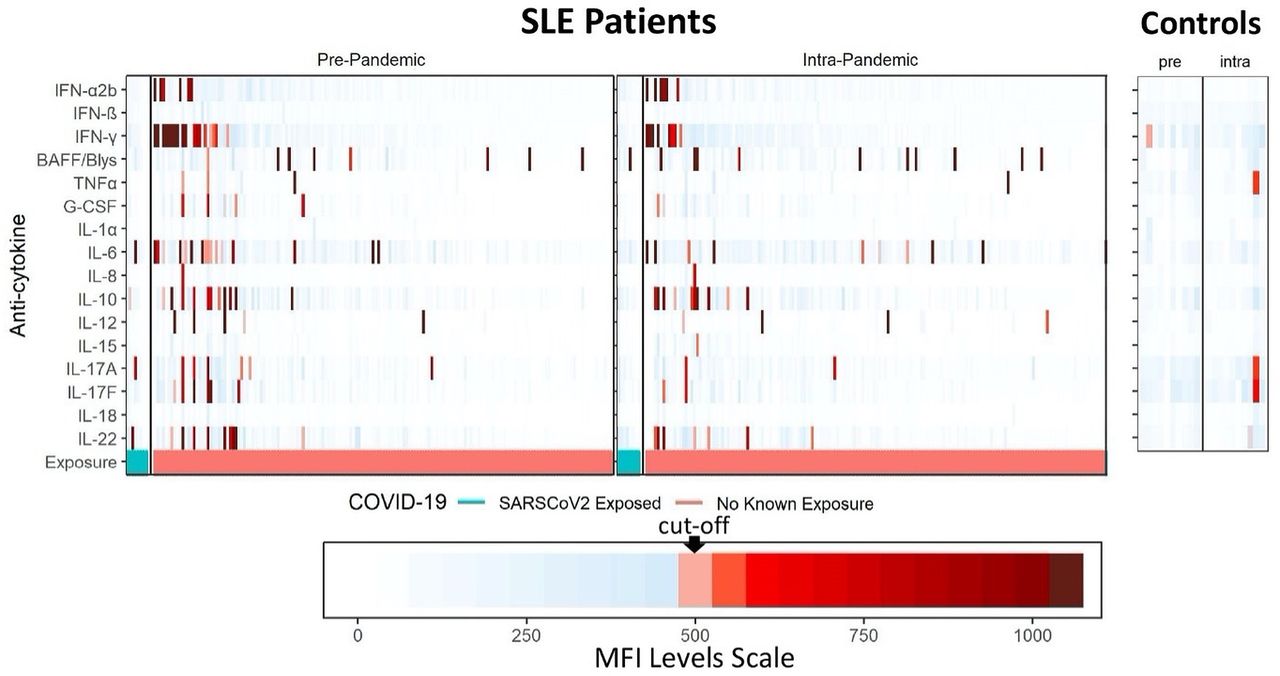
The SLE cohort consisted of 173 patients (94.8% female, mean age 48.5 years, mean disease duration 11.7 years, 42.8% non-White race/ethnicity, 83.2% prescribed hydroxychloroquine, 28.9% corticosteroids and 43.9% other immunomodulators).11 Intrapandemic samples from nine patients had SARS-CoV-2-positive serology and/or RT-PCR confirmed SARS-CoV-2 infection (SARS-CoV-2 serology + and RT-PCR+ (n=3); SARS-CoV-2 serology + and RT-PCR not done (n=3); SARS-CoV-2 serology− and RT-PCR+ (n=3)), yielding 164 patients with no laboratory evidence of SARS-CoV-2 exposure. The frequency of cytokine autoantibodies in the prepandemic and intrapandemic samples stratified by SARS-CoV-2 exposure is shown in table 1, the patient characteristics and cytokine autoantibodies for the nine exposed patients are shown in table 2, and a graphical representation of the distribution of cytokine autoantibodies and their titers is shown in figure 1 (patients are sorted from left to right based on descending T1IFN autoantibody titres separately for prepandemic and intrapandemic samples).
Frequency of cytokine autoantibodies among prepandemic and intrapandemic samples stratified by SARS-CoV-2 exposure (positive RT-PCR test or positive SARS-CoV-2 serology)
Characteristics of SLE cohort patients with positive intrapandemic SARS-CoV-2 serology and/or positive RT-PCR
{kind=link}
Heat map of cytokine autoantibody titres in prepandemic and intrapandemic patients with SLE who had evidence of SARS-CoV-2 exposure versus those who had no evidence of SARS-CoV-2 exposure. Apparently healthy controls are shown for comparison as a reference for established cut-offs. Each vertical column in the heat map represents an individual patient. The patients are sorted from left to right based on descending type I interferon (T1IFN) autoantibody titres. Therefore, the order of the patients in the prepandemic and intrapandemic panels are not the same. A supplemental figure where the prepandemic and intrapandemic results are vertically aligned is provided online supplemental figure 1. MFI, median fluorescence intensity.
Supplemental material
In the prepandemic samples, 33.3% (3/9) of patients with serological and/or RT-PCR evidence of SARS-CoV-2 exposure versus 28.0% (46/164) without exposure had at least one cytokine antibody (p=1.00). In the intrapandemic samples, 22.2% (2/9) of exposed versus 23.1% (38/164) without exposure had at least one cytokine antibody (p=1.00). Overall, there was no difference in the frequency of cytokine autoantibodies in prepandemic compared with intrapandemic samples (28.3% (49/173) vs 23.1% (40/173), respectively; p=0.33). In the entire cohort of 173 patients, the most common cytokine autoantibodies in prepandemic samples were directed against IFN-γ (9.8%), followed by IL-6 (8.7%), IL-10 (5.8%) and BAFF (4.6%) (table 1 and figure 1) compared with 5.2% for IFN-γ and anti-IL-6, 5.8% for IL-10% and 6.4% for BAFF in intrapandemic samples. In the prepandemic samples, none of the exposed patients had autoantibodies to IFN-γ versus 10.4% (17/164) without exposure (p=0.66). In the intrapandemic samples, 11.1% (1/9) of the exposed patients had autoantibodies to IFN-γ versus 4.9% (8/164) without exposure (p=0.96). In the prepandemic and intrapandemic samples, none of the exposed patients had autoantibodies to T1IFN (IFN-α or IFN-β) versus 3.7% (6/164) without exposure had autoantibodies to IFN-α and 0% without exposure had autoantibodies to IFN-β (p=1.00 and not applicable, respectively).
When cytokine autoantibodies were analysed for associations with SLE-related autoantibodies, only in intrapandemic samples were there associations with p values less than 0.05: anti-IFN-α and anti-dsDNA (intrapandemic p=0.015 vs prepandemic p=0.7035); IL-12 and anti-dsDNA (intrapandemic p=0.043 vs prepandemic p=0.816); IL-12 and anti-ribosomal P (intrapandemic p=0.009 vs prepandemic p=1.000); and IL-12 and anti-Sm (intrapandemic p=0.005 vs prepandemic p=1.000). However, after correcting for multiple comparisons none of these associations met the reduced α (α=0.00045) to be considered statistically significant.
Discussion
The frequency of cytokine autoantibodies observed in our study is in keeping with previous publications that used similar assay techniques reporting that up to 27% of patients with SLE had cytokine autoantibodies.1 3 In the present study, none of the patients with SLE with confirmed exposure to SARS-CoV-2 had autoantibodies to T1IFN and, as we previously reported,11 none of the 173 patients in our cohort, including the 9 patients with confirmed exposure, had severe COVID-19 symptoms necessitating hospitalisation. Hence, we could not confirm that T1IFN autoantibodies increase the risk for severe SARS-CoV-2. The overall observed frequency of anti-IFNγ autoantibodies in our study is consistent with a previous report of 11% in patients with SLE.1 In an earlier communication, we reported that this SLE cohort had a lower rate of prepandemic seropositivity and a slightly lower to similar rate of intrapandemic seropositivity compared with contemporaneous controls.11 Granted, in the current report we did not study the neutralising effect of cytokine autoantibodies, but it would be difficult to explain T1IFN neutralising activity in the absence of detectable T1IFN cytokine autoantibodies. In addition, we found a non-significant association between IFNγ autoantibodies and dsDNA autoantibodies in intrapandemic samples, which is similar to a previous report that anti-IFNγ autoantibodies were associated with anti-dsDNA.1 Further, due to the size of our cohort and its geographical context, our results may not be generalisable to a broader population of patients with SLE. Because of interest in vaccine responses in patients with SLE,12–15 current efforts are focusing on a possible relationship of cytokine autoantibodies to adverse or unusual reactions.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the University of Calgary Ethics Board (REB13-0425). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank Haiyan Hou, Meifeng Zhang and Dr Paul Sciore (University of Calgary) for their laboratory technical assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AEC and MJF are joint senior authors.
Contributors All authors were involved in the concept and design, data analysis and interpretation, and editing for intellectual content. MJF and AEC are joint senior authors.
Funding AEC holds The Arthritis Society Chair in Rheumatic Diseases at the University of Calgary and some of these funds were used to support HW and FSC.
Competing interests MJF is a consultant to and has received honoraria and/or travel support from Werfen (Barcelona, Spain, San Diego, CA). MJF is also Medical Director of Mitogen Diagnostics Corporation. MYC has received consulting fees from Janssen, AstraZeneca and MitogenDx. AEC has received consulting fees from AstraZeneca, Bristol Myers, Squibb and Glaxo Smith Kline. All other authors declare no conflict of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.