Article Text

Abstract
Objective Treatment response in lupus nephritis (LN) is defined based on proteinuria, yet protocol kidney biopsy studies have shown that patients with lupus can have active nephritis in the absence of proteinuria. Using estimated glomerular filtration rate (eGFR) trajectories, we characterised early chronic kidney disease in LN and examined whether certain patients continue to accrue renal damage despite proteinuric response.
Methods We conducted a single-centre study of patients diagnosed with their first episode of biopsy-proven class III, IV, and/or V LN (n=37). For each patient, eGFR trajectory was graphed over 5 years following renal biopsy. Participants were divided into those with progressive eGFR loss (eGFR slope <−5 mL/min/1.73 m2/year) versus those with stable eGFR. Participant demographics, renal biopsy features and response status at 1 year (urine protein to creatinine ratio <500 mg/g) were compared between eGFR trajectory groups.
Results Overall, 30% (n=11) of participants accrued progressive eGFR loss despite standard of care therapy over the first 5 years following renal biopsy. There were no significant differences in baseline renal biopsy features, medication regimens or comorbidities between eGFR trajectory groups. Resolution of proteinuria at 1 year did not differentiate between groups: 6 of 18 (33%) of complete responders continued to accrue renal damage compared with 5 of 17 (29%) of non-responders. Response status could not be assigned for two participants in the stable eGFR group due to missing clinical information at 1 year.
Conclusions We identified an understudied category of patients with LN who accrue progressive renal damage despite apparent response to standard of care therapy. Better definitions and biomarkers of response are needed to improve renal outcomes and trial design.
- Lupus Nephritis
- Systemic Lupus Erythematosus
- Outcome Assessment, Health Care
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic?
Despite currently available therapies, chronic kidney disease is common in lupus nephritis (LN) and, when severe, is a strong predictor of mortality. Recent protocol renal biopsy studies have shown that proteinuria may not accurately reflect disease activity for certain patients.
What does this study add?
This is the first study of estimated glomerular filtration rate (eGFR) trajectories in LN. Nearly one-third of patients in this study experienced ongoing rapid loss of eGFR despite standard of care therapy, and proteinuric response at 1 year did not predict eGFR trajectory, with one-third of ‘responders’ continuing to lose eGFR.
How might this impact clinical practice or future research?
Better biomarkers of LN treatment response are needed to improve renal outcomes in clinical practice and to inform trial design.
Introduction
Up to 40% of individuals with SLE with class III, IV or V lupus nephritis (LN) will develop irreversible renal impairment within their lifetime.1 2 Over 20 years of follow-up, at least 20% of those with SLE will develop end-stage renal disease (ESRD), which is the single strongest predictor of mortality in lupus.3 At a population level, proteinuria is an important biomarker of lupus disease activity in the kidney. Proteinuria within the first year of SLE diagnosis is a strong predictor of future ESRD, and conversely, achievement of complete proteinuric response (traditionally defined as <0.5 g/24 hours) after 1–2 years of LN therapy is generally associated with improved renal outcomes.4 5 Recently, however, it has become increasingly appreciated that those with SLE can have active class III, IV or V LN even in the absence of proteinuria, active urinary sediment or an abnormal estimated glomerular filtration rate (eGFR).6–10
It follows that traditional definitions of treatment response in LN (based on proteinuria) may fail to account for individuals who continue to have disease activity in the kidney despite the resolution of proteinuria and/or having a normal eGFR. We hypothesised that some patients with LN might continue to accrue kidney damage despite being classified as treatment responders based on resolution of proteinuria. We sought to characterise the early stages of chronic kidney disease (CKD) in LN and assessed the ability of traditional prognostic features such as renal biopsy class and proteinuria to predict progressive renal damage.
Nearly all prior studies of long-term renal outcomes in LN have focused on CKD definitions based on numerical cut-offs for eGFR, for example, defining stage 3 CKD as eGFR <60 mL/min/1.73 m2.1–3 5 Using these traditional definitions, at least 5 if not more than 10 years of eGFR loss are needed to develop this degree of renal injury. This is inadequate to detect early stages of CKD, when intervention is more likely to be successful. We thus assessed eGFR slope, which the US Food and Drug Administration has recently accepted as a surrogate outcome for CKD progression in clinical trials.11 To our knowledge, this work is the first cohort study to focus on early eGFR trajectory in LN in this fashion.
Methods
Study design
This study was an analysis of prospectively collected patient data from the Hopkins Lupus Cohort. Patients in the Hopkins Lupus Cohort are seen quarterly for physician assessment of disease activity, laboratory tests including renal function, and cardiovascular risk factors including blood pressure measurement at each visit. Eligible participants with LN were selected via review of stored cohort data. All demographic and clinical data, as well as information regarding selection and dosage of immunosuppressive therapy, were extracted from our cohort dataset.
Patient population
Patients with SLE who were diagnosed with their first episode of renal biopsy-confirmed class III, IV, and/or V LN through follow-up with the Hopkins Lupus Cohort were identified for this study. Individuals were excluded if their biopsy of interest was before 2004 (to reflect modern outcomes) or if they had fewer than 5 years of follow-up data available after biopsy. One patient was excluded due to receiving a renal transplant within the first 5 years after biopsy. In total, 37 patients with class III, IV, and/or V LN were included.
eGFR analysis and outcome assignment
For each patient, eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration formula12 at each visit within the time frame of interest. eGFR slope was calculated using linear regression across the eGFR values over the 5 years of follow-up after each patient’s biopsy. The first 90 days after biopsy were excluded from this calculation so as to avoid acute effects. Participants were then divided into those with progressive eGFR loss (eGFR slope <−5 mL/min/1.73 m2 per year) versus those who maintained a stable eGFR (eGFR slope not meeting the above threshold). This threshold for eGFR slope has been used as a definition of rapid CKD progression per Kidney Disease Improving Outcomes 2012 guidelines and has been applied in similar studies of early CKD.13 As for treatment response, complete renal response was defined as proteinuria of less than 500 mg (per random urine protein:creatinine ratio or 24-hour urine protein collection) at 1 year after renal biopsy. Each participant was categorised as either a complete responder or non-responder based on this definition.
Statistical testing
Baseline demographics, renal biopsy features, immunological status, treatment regimen and comorbidities were compared between eGFR trajectory groups using the Student’s t-test, Wilcoxon rank-sum test or Fisher’s exact test as appropriate.
Patient involvement in research
Patients were not involved in the design of the Hopkins Lupus Cohort at the time of its inception 36 years ago.
Results
eGFR trajectory analysis identified early CKD in one-third of patients with LN
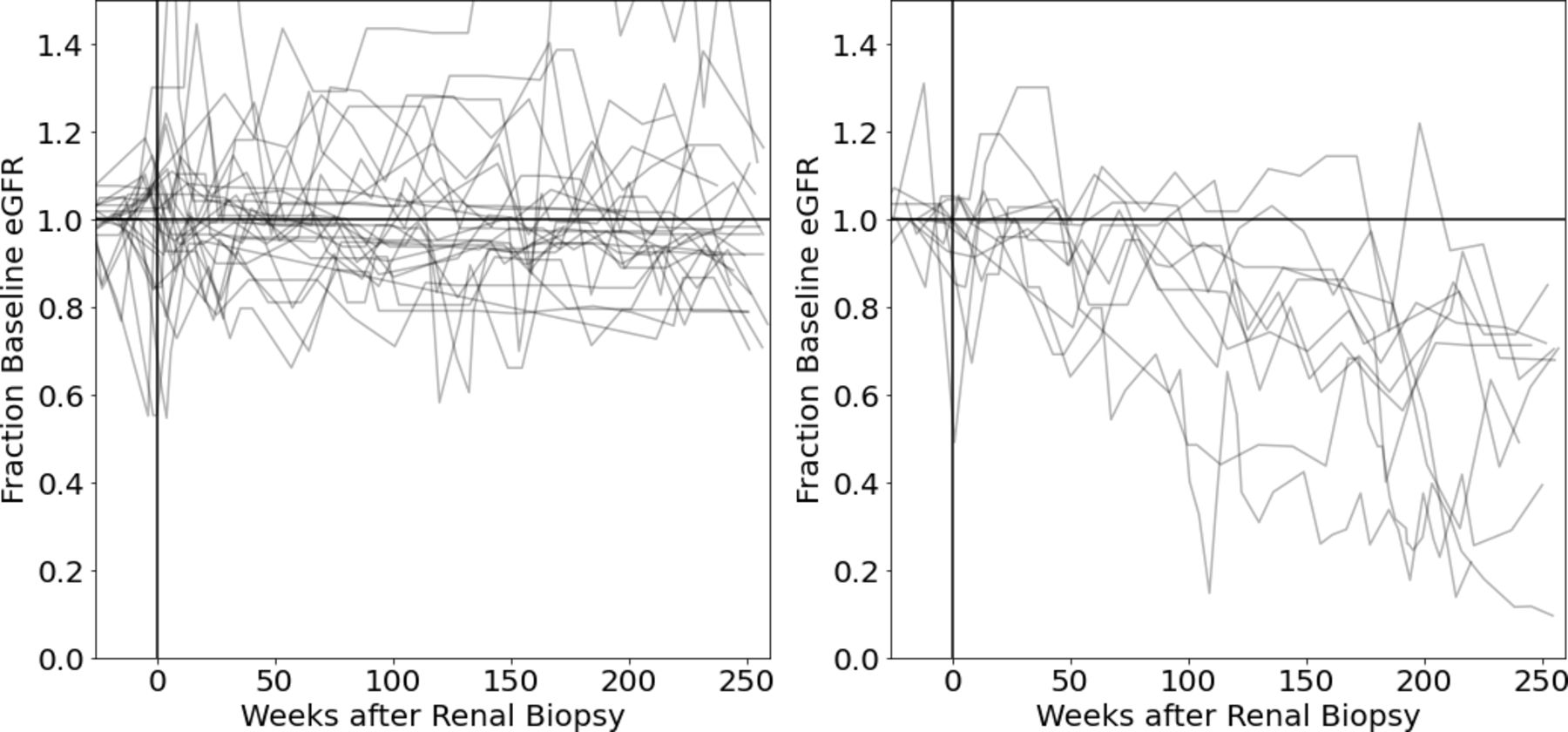
eGFR was graphed over time for each participant, with the resulting trajectories shown in figure 1. Serum creatinine was graphed over time in the same fashion with similar results (not shown). Among these 37 participants diagnosed with their first episode of LN, 30% (n=11) accrued progressive renal damage (eGFR slope <−5 mL/min/1.73 m2 per year) despite standard of care therapy over the first 5 years following renal biopsy.
{kind=link}
Among patients with their first episode of LN, 30% exhibit progressive eGFR loss despite standard of care treatment. Shown here are the eGFR trajectories of participants who maintained a stable eGFR (left panel; n=26) versus those who progressively lost eGFR (right panel; n=11). Each line represents the eGFR values for one participant over time. To facilitate comparison between participant trajectories, eGFR values were normalised to each participant’s pre-LN baseline eGFR (average eGFR from 3 to 12 months prior to biopsy). eGFR, estimated glomerular filtration rate; LN, lupus nephritis.
The distribution of eGFR slopes is shown in online supplemental figure 1. All participants included had at least 5 years of follow-up data available, and only these first 5 years of data were used to calculate eGFR slope. On average, 18 observations of eGFR per participant were available and included in the eGFR slope calculation. Only one participant had fewer than five clinic visits during the 5-year follow-up period. Prior to developing LN, the majority of participants (78%, n=29) had a normal eGFR of >90 mL/min/1.73 m2. Five participants had stage 2 CKD (eGFR 60–90 mL/min/1.73 m2) at baseline, two had stage 3A (eGFR 45–59 mL/min/1.73 m2), and one had stage 3B CKD with an eGFR of 44 mL/min/1.73 m2.
Supplemental material
Baseline clinicodemographic characteristics were similar in patients with stable or declining eGFR
Participant demographics, renal biopsy features, baseline immunological status, treatment regimen and pertinent comorbidities in the two eGFR trajectory groups are summarised in table 1. None of these baseline features independently predicted the likelihood of eGFR stability versus decline. Specifically, sex, race, age or body mass index did not associate with eGFR trajectory group. The mean pre-LN eGFR was >100 mL/min/1.73 m2 in both groups. Histological features were similar: 77% and 82% of participants had some component of proliferative LN in the stable and declining eGFR group, respectively, and activity and chronicity indices were also comparable. Serological autoantibody status, such as prevalence of anti-dsDNA positivity, was also not different between the eGFR trajectory groups.
Baseline or other early characteristics of the eGFR trajectory groups
Treatment with hydroxychloroquine, mycophenolate mofetil (vs other immunosuppressive therapy), ACE inhibitors or angiotensin II receptor blockers and maximum prednisone dose did not associate with eGFR stability versus decline (table 1). Finally, there was no significant difference in the prevalence of pre-existing hypertension or diabetes mellitus between the eGFR groups. Furthermore, none of these participants developed diabetes mellitus within the first year of LN treatment. As diabetic nephropathy generally only develops several years after a diabetes mellitus diagnosis,14 this likely did not have a significant impact on eGFR in either group.
Blood pressure control was examined in greater detail as shown in tables 2 and 3, again with no clear differences between the eGFR trajectory groups. Mean blood pressures at baseline and during follow-up were similar between the eGFR groups. Blood pressure variability was numerically higher in the eGFR decline group, with a mean within-person SD of 14.5 mm Hg vs 10.2 mm Hg in the stable eGFR group (p=0.068). This is nevertheless difficult to interpret, as decreased eGFR itself may lead to higher or more variable blood pressures,15 and indeed the directionality of the causal relationship between increased blood pressure and reduced eGFR is generally difficult to determine for this reason. Regardless, there did not appear to be a profound association between blood pressure and eGFR trajectory group in this study.
Comparison of eGFR trajectory groups with respect to blood pressure (BP) measured at various points in time after renal biopsy
Comparison of eGFR trajectory groups with respect to blood pressure variability
Proteinuric response at 1 year did not predict early CKD
Proteinuric response status was determined for each participant as described in the Methods section. Response status at 1 year did not differentiate between the eGFR trajectory groups (table 4). Notably, 55% of participants with progressive eGFR loss (n=6 of 11) would have been classified as complete responders, traditionally viewed as low risk for ongoing renal damage, based on <500 mg/g urine protein at 1 year after biopsy. Among all complete responders at 1 year, 33% continued to accrue significant renal damage despite standard of care therapy (n=6 of 18). These results were unchanged when we repeated this analysis using a slightly relaxed threshold of <700 mg/g urine protein as the definition of response. Three additional participants would be classified as responders per this threshold, where two maintained a stable eGFR, and one experienced progressive eGFR loss. Thus, again, 33% of responders (n=7 of 21) experienced eGFR loss despite proteinuric response. In the eGFR decline group, 64% would be classified as responders (n=7 of 11) compared with 58% (n=14 of 24) responders in the stable eGFR group (p=1.0).
Response status (based on proteinuria <500 mg/g) at 1 year per eGFR trajectory group
Serum albumin and the presence of active urine sediment (ie, >5 red blood cells per high-power field and/or presence of cellular casts) at 1 year also did not significantly differ between the eGFR trajectory groups. After 1 year, the mean serum albumin was 3.7 g/dL in the stable eGFR group vs 3.6 g/dL in the declining eGFR group (p=0.67). Active urine sediment was present in 20% (n=5 of 25; one patient had missing urine microscopy) of the stable eGFR group vs 0% (n=0 of 11) of the declining eGFR group (p=0.30).
Discussion
We have identified an understudied category of patients with their first episode of LN who accrue progressive renal damage despite apparent response to standard of care therapy. Specifically, roughly half of the participants in this study with a worrisome eGFR trajectory would be misleadingly classified as complete responders after 1 year of treatment based on resolution of proteinuria. These findings indicate that definitions of LN treatment response which are based on proteinuria can fail to identify many patients who continue to accrue renal damage despite treatment. To our knowledge, this work is the first to examine trajectories of early progression of CKD in LN and to de-couple this analysis from proteinuria.
We incidentally noted a subacute decline in eGFR in many patients during the 3 months leading up to their renal biopsy, which then rapidly improved to near pre-LN baseline with treatment as shown in figure 1 (note the week 0 time point). To our knowledge, this is the first published account of this phenomenon. This finding is also potentially relevant to clinical trial design, where definitions of treatment response may also be based on the preservation of eGFR assessed at the time of renal biopsy. If a patient’s eGFR is transiently reduced at the time of biopsy, then this measurement is not a true baseline eGFR, and thus not an accurate goal or metric for renal recovery.
We were not able to identify any clear predictors of early renal decline (after biopsy) based on demographics, immunological status, renal biopsy features, immunosuppressive treatment regimen or relevant comorbidities. This is at odds with traditional views of poor prognostic factors in LN such as proliferative features on biopsy, activity or chronicity indices, and race,1 though it is possible that any associations between these prognostic factors and renal outcome are present but much weaker than expected, and thus were not detected in this study given the relatively small sample size. As the vast majority of outcome studies in LN have been based on eGFR cut-offs rather than slope, these factors may still be meaningful with respect to informing which patients will go on to develop ESRD, but do not appear to consistently identify those with rapid eGFR decline early after diagnosis (that is, those with a significant loss in eGFR but not reaching ESRD) despite appropriate immunosuppressive therapy.
We acknowledge that proteinuria remains an important biomarker in current clinical practice. At the population level, proteinuria is still generally successful at risk stratifying which patients will progress to severe CKD, especially ESRD.4 5 Follow-up analyses of both the MAINTAIN Nephritis Trial16 and the Euro-Lupus Nephritis cohort17 determined that proteinuria of <700–800 mg/g after 12 months of treatment was generally predictive of a positive long-term renal outcome, defined as a serum creatinine of ≤1.0 mg/dL after 7 years in these studies. The sensitivity and specificity of this proteinuria threshold in predicting a positive long-term outcome were 70%–80% in both cohorts. While this demonstrates the broad prognostic ability of proteinuria, it also indicates that there were a significant portion of patients for whom reduced proteinuria did not portend long-term renal protection or vice versa. This is conceptually consistent with the results of our work and likewise highlights the limitation of proteinuria as a metric of treatment success for any given individual. It is additionally worth noting that a serum creatinine of 1.0 mg/dL would represent a 20%–30% loss of eGFR for most young women who start with an eGFR of >100 pre-LN, as in the patients in this study.
Our work complements prior studies which used protocol kidney biopsies in LN, which have shown that proteinuria can be absent in the presence of active renal histology (or vice versa). Wakasugi et al performed renal biopsies on nearly 200 patients with lupus with and without clinical renal involvement, which was defined as proteinuria >400 mg/g, active urinary sediment, and/or eGFR <67 mL/min/1.73 m2 in their analysis.6 They discovered that up to 20% of cases of class III, IV and V LN diagnosed on biopsy were entirely clinically silent based on the criteria above. More recently, De Rosa et al performed per protocol renal biopsies on a subset of patients with LN who had been in renal remission for at least 12 months.9 Persistent histological activity was present in 44% of these participants (despite resolution of proteinuria), and the activity index on biopsy could accurately predict which participants would experience a renal flare when immunosuppression was tapered. Malvar et al similarly identified a discordance between clinical and histological features in patients with proliferative LN: one-third of patients with clinical response had persistently high histological activity, and roughly two-thirds of patients in histological remission would still be considered clinically active based on the presence of proteinuria.8
CKD progression in patients with proteinuric response may be secondary to persistent intrarenal inflammation,8 9 profibrotic processes18 or other mechanisms not yet discovered. We speculate that specific urinary proteins that correlate with intrarenal inflammation or active fibrosis–rather than the total amount of protein in the urine–could potentially be superior predictors of the development of CKD in LN.19 20 Urine proteomic biomarkers of intrarenal matrix remodelling and inflammation can successfully detect early CKD in various other nephropathies and predict risk of CKD progression in diabetic nephropathy.21–23 Good et al identified 273 urinary peptides which characterise individuals with CKD secondary to various aetiologies (including SLE in roughly 10% of participants).24 This multidimensional biomarker, called CKD273, was then validated for the diagnosis of CKD (blinded to aetiology) in two independent cohorts24 25 and has been found to be superior to urinary albumin in predicting early and/or progressive CKD in diabetes mellitus in multiple follow-up studies.21–23 The discovery of a similar biomarker panel in LN could (1) guide early identification and personalised treatment of patients at high risk of progressive CKD despite immunosuppression, and (2) identify potential novel targets in the treatment of LN overall.
Several agents which are effective at slowing eGFR decline are already available and might prove particularly useful in high-risk patients with LN. It has already been demonstrated that belimumab can slow eGFR decline in patients with LN as compared with standard therapy alone.26 27 It was also recently shown that dapagliflozin, a sodium-glucose cotransporter 2 inhibitor, reduces the composite risk of sustained eGFR decline, ESRD, or death from a renal or cardiovascular cause in a general population with CKD, although individuals with LN were excluded.28 Specific treatments for APOL1-associated renal disease are not yet available, though may be in the near future.29 Genetic variants in APOL1 have been associated with an increased risk of CKD in those with African ancestry, both in the general population and among those with LN,30 31 and targeted therapeutics along these lines might be of particular benefit for many black patients with LN.
There are several limitations to this study. This was a single-centre study with a relatively small sample size, though we intentionally focused only on patients diagnosed with their first episode of LN so as to minimise confounding factors and more clearly identify patterns in eGFR trajectory. This small sample size may have limited the ability to detect differences in features of interest (eg, demographics, biopsy features) between eGFR trajectory groups. We were also unable to assess genetic risk factors such as APOL1 (see above). APOL1 genotyping has been performed on a subset of African-American patients in the Hopkins Lupus Cohort,32 but unfortunately these data were only available in two of the participants in the eGFR decline group, and thus we could not pursue a meaningful investigation into this factor.
Nevertheless, we believe that this work demonstrates that traditional metrics of renal response (namely proteinuria) may be falsely reassuring for certain individual patients. Our results also indicate that such patients may be relatively common, with one-third of proteinuric responders developing progressive renal decline in this cohort. Overall, these results suggest that better definitions and biomarkers of renal response in LN are needed to improve long-term renal outcomes and trial design.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The Hopkins Lupus Cohort Study is approved on an annual basis by the Johns Hopkins University School of Medicine Institutional Review Board (Research Project Notification: NA_00039294) and informed written consent is obtained from all participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at This manuscript is based on work presented at American College of Rheumatology Convergence 2021: 'One Third of Lupus Nephritis Patients Classified as Complete Responders Continue to Accrue Progressive Renal Damage Despite Resolution of Proteinuria' (Abstract Number 1284), authored by EW, AF, DG and MP.
Contributors EW conceived of the study, completed data analyses, and drafted and revised the manuscript. LM completed all statistical analyses pertaining to blood pressure control. All authors including AF, DG and MP contributed significantly to conceptual refinement of the analyses performed and critical revision of the manuscript. EW and MP accept full responsibility for the finished work and conduct of the study, had access to the data, and controlled the decision to publish.
Funding The Hopkins Lupus Cohort is funded by R01-AR069572. EW was funded through the National Institutes of Arthritis, Musculoskeletal, and Skin Diseases (NIAMS) of the National Institutes of Health (NIH) under award number T32-AR048522.
Disclaimer This content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or NIAMS.
Competing interests EW, AF, LM and DG—none. MP has received research funding from and/or served as a consultant to Alexion, Amgen, AstraZeneca, Aurinia, Eli Lilly, Emergent BioSolutions, Exagen, Gilead Sciences, GSK, IQVIA, Idorsia, Janssen, EMD Serono, Momenta Pharmaceuticals, PPD, Sanofi, Thermo Fisher and UCB.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.