Article Text

Abstract
Objective Renal injury is common in SLE. Immune complex deposition plays an important role in the development of lupus nephritis (LN), while little is known about glomerular IgG4 deposition in patients with LN. This study aimed to investigate the characteristics and renal outcome of patients with LN with glomerular IgG4 deposition.
Methods This is a single-centre retrospective study enrolling 89 patients with biopsy-proven LN. Clinicopathological features, treatment responses and renal outcomes were collected and compared between patients with and without glomerular IgG4 deposition. Renal outcome events include progression of renal dysfunction and end-stage renal disease.
Results Thirty (33.7%) patients had glomerular IgG4 deposition. Patients with glomerular IgG4 deposition had lower serum albumin level (25.06±8.61 g/L vs 28.29±6.31 g/L, p=0.05), more class V LN (60.0% vs 35.6%, p=0.03), more positive phospholipase A2 receptor (PLA2R) staining (43.3% vs 18.6%, p=0.01), more IgG1 deposits (96.7% vs 64.4%, p=0.01) and less C3 deposits (46.7% vs 72.9%, p=0.02) than those without glomerular IgG4 deposition. They also had better renal survival than those without glomerular IgG4 deposition (96.7% vs 79.7%, p=0.03). Multivariate Cox regression showed that high serum creatinine level (relative risk (RR)=1.005, 95% CI 1.002 to 1.008, p=0.01) and high Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) scores (RR=1.078, 95% CI 1.004 to 1.157, p=0.04) independently correlated with poor renal outcome, while glomerular IgG4 deposition tended to correlate with good renal outcome (RR=5.95, 95% CI 0.759 to 45.97, p=0.09). Further, patients with both glomerular IgG4 and PLA2R positivity (n=13) had higher levels of serum C3 and C4 and less glomerular C3 deposits compared with those with positive IgG4 but negative PLA2R in the glomerulus (n=17), and had a tendency of low SLEDAI score (p=0.07).
Conclusions Patients with LN with glomerular IgG4 deposits may have better renal survival, and patients with LN with simultaneous glomerular IgG4 and PLA2R deposits may have low disease activity.
- lupus nephritis
- lupus erythematosus, systemic
- autoimmune diseases
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
IgG4 deposition is a potential marker in the differentiation of idiopathic membranous nephropathy, while little is known about the impact of IgG4 deposition in patients with lupus nephritis.
WHAT THIS STUDY ADDS
Patients with lupus nephritis with glomerular IgG4 deposits may have better renal survival.
Patients with lupus nephritis with simultaneous glomerular IgG4 and phospholipase A2 receptor deposits may have low disease activity.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Elucidating the association of IgG4 deposition with clinical activity and renal pathological activity in patients with lupus nephritis will help predict the prognosis of the disease.
SLE is a chronic autoimmune and inflammatory disease that affects multiple organs. Nearly 40% of patients with SLE have kidney injury, commonly lupus nephritis (LN). Approximately 10%–30% of patients with LN develop end-stage renal disease (ESRD) within 15 years.1 2 Proliferative glomerulonephritis and deposition of various classes of immune complex (IC) in the glomerulus are the main pathological features of LN. IC deposition plays important roles in LN progression.
IgG is a key component of these immune deposits. According to the distinct constant region of its heavy chain, IgG can be classified into four different subclasses. Each subclass has unique biological functions. IgG1 and IgG3 contribute to complement activation via binding with high-affinity C1q.3 4 IgG4 is a unique subclass of IgG. It does not bind C1q and cannot activate complement via the classic pathway because the length and sequence of the amino acids in the hinge region of IgG4 result in its low binding ability with C1q. There is only weak binding to certain FcgRs, resulting in reduced capacity to activate certain immune effector cells.5 IgG4-containing ICs may activate complement via the mannose-binding lectin pathway, which is reported to be involved in various IC-related glomerulopathies,6 most notably IgA nephropathy.7 It is accepted that IgG4 autoantibodies play an important role in the pathogenesis of idiopathic membranous nephropathy (MN). Bannister et al8 reported nearly 100% IgG4 deposition in idiopathic MN kidneys, while in secondary MN there is less IgG4 deposition. In MN secondary to SLE, some studies reported IgG4 deposition in the glomerulus. Kuroki et al9 reported that nearly 60% of patients with LN had IgG4 deposition. Iskandar et al10 reported that most cases of diffuse proliferative LN showed IgG3 as the major IgG subclass present in glomerular deposits; by contrast, IgG4 predominated in six of seven cases of MN of unspecified aetiology. Imai et al11 reported that three out of four diffuse membranous LN showed glomerular IgG4 deposition. These patients with subepithelial deposits were similar to those found in patients with MN, showing IgG4 deposition along the basement membrane. Due to limited number of patients, the impact of glomerular IgG4 deposition in LN is still controversial. In this study, we examined the distribution of IgG subclass in the glomeruli from LN biopsies and aimed to find the characteristics and renal outcomes of patients with LN with IgG4 deposition in the glomerulus.
Materials and methods
We retrospectively investigated patients with LN who were hospitalised between September 2015 and April 2017 and were regularly followed up at the Kidney Disease Center of the First Affiliated Hospital, Zhejiang University School of Medicine. All patients fulfilled the American College of Rheumatology 1997 revised criteria for SLE.12 Renal pathology was obtained from each patient at hospitalisation. Data on clinical symptoms and laboratory findings were collected until the final follow-up.
We collected data including demographic information, clinical symptoms and laboratory examination results. The Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) score was calculated to evaluate lupus activity. Laboratory results included white cell count (WCC), haemoglobin (HB), platelets (PLT), serum albumin, serum creatinine (SCr), complement C3, complement C4, anti-double-stranded DNA (dsDNA) antibody, urine protein, haematuria and estimated glomerular filtration rate (eGFR).
Renal biopsy tissues were examined by light microscopy, immunofluorescence (IF) and electron microscopy (EM). Histological changes were classified according to the International Society of Nephrology and Renal Pathology Society criteria as follows: class Ⅰ, minimal mesangial LN; class Ⅱ, mesangial proliferative LN; class Ⅲ, focal LN; class Ⅳ, diffuse LN; class Ⅴ, membranous LN; and class Ⅵ, advanced sclerosing LN.13 The parameters under light microscopy included glomerular sclerosis and crescents. Glomerular IF staining included IgG and its subclasses IgG1, IgG2, IgG3 and IgG4, IgM, IgA, C3, C4 and C1q. Their intensity was semiquantitatively scored on a scale from 0 to 3+: 0, absent; 1+, weak; 2+, moderate; and 3+, strong. Typical IF images of IgG subclasses are shown in figure 1. EM was used to observe the deposition sites of ICs in the glomerulus, such as the subcutaneous area, subepithelial area, mesangium and intraglomerular basement membrane (GBM) area.

Immunofluorescence showed staining of IgG subclasses in a patient with class V lupus nephritis.
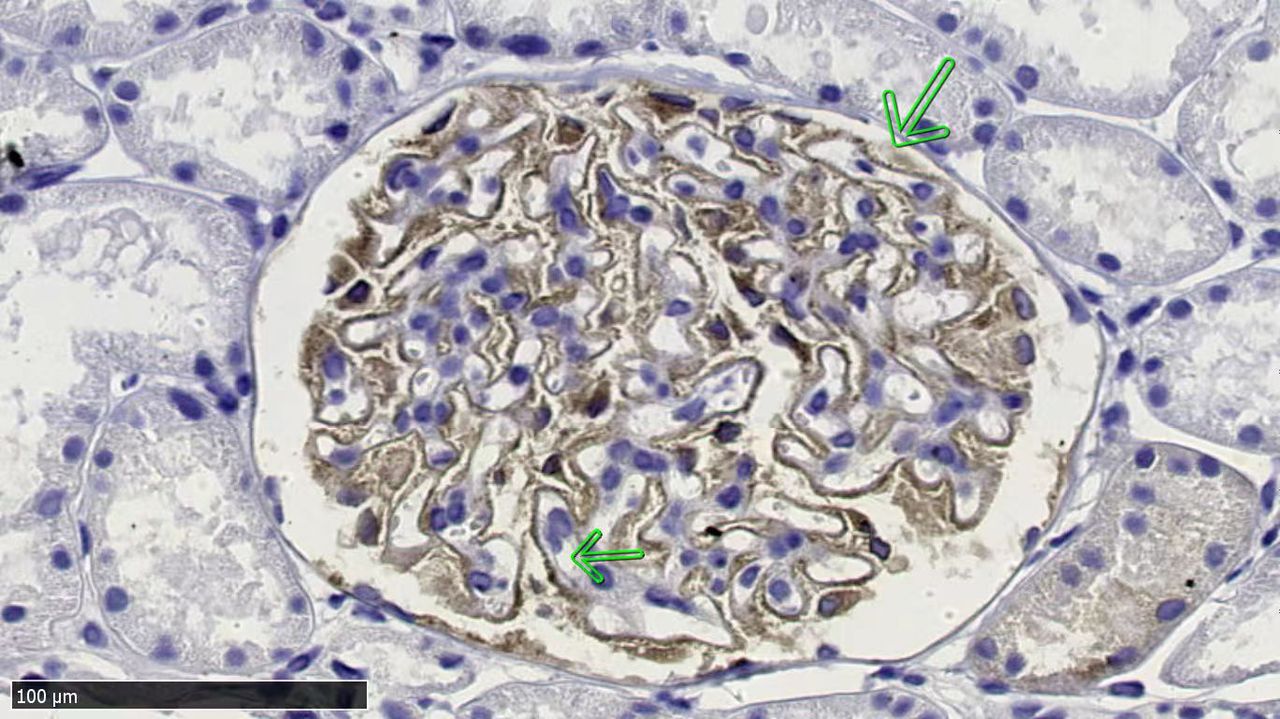
The interpretation of phospholipase A2 receptor (PLA2R) staining was according to the criteria suggested by Hoxha et al.14 Briefly, it was based on the assessment of two parameters: staining pattern and staining distribution along the glomerular capillary walls. In normal kidney tissue there is very weak expression of PLA2R in the podocytes, which was diagnosed as a negative result in this study. When strong PLA2R staining was presented along the glomerular capillary wall in a fine granular pattern, the result was diagnosed as positive. Typical positive immunohistochemistry staining of PLA2R is shown in figure 2.

Immunohistochemistry showing positive PLA2R staining along the glomerular capillary loop in a patient with class V lupus nephritis (arrows point to PLA2R fine granular staining along glomerular capillary loop). PLA2R, phospholipase A2 receptor.
Immunosuppressive treatment was collected during follow-up. For response to therapy, complete response (CR) was defined as reduction in proteinuria to <0.5 g/g per 24 hours and stabilisation or improvement in kidney function (±10%–15% of baseline); partial response (PR) was defined as reduction in proteinuria by at least 50% and to <3 g/g per 24 hours and stabilisation or improvement in kidney function (±10%–15% of baseline). Remission of LN includes CR and PR. Renal outcome events include progression of renal dysfunction, defined as glomerular filtration rate decreasing more than 30% during follow-up, and ESRD, defined as maintaining renal replacement therapy.
Statistical analysis
Statistical analysis was performed by SPSS V.23.0. Descriptive statistics for numerical data are presented as mean±SD or median and IQR, respectively. Differences in numerical data with normal distribution were tested by Student’s t-test. Other numerical data and semiquantitative scores were compared by Mann-Whitney U test. Categorical data are presented as counts with percentages (%) and compared by χ2 test. Renal survival was calculated using Kaplan-Meier analysis with log-rank test. Univariate and multivariate Cox regression were used to analyse the correlation between IgG4 deposition and renal outcomes. P<0.05 was considered significant.
Results
The analysis included 89 patients, with 16 men and 73 women. According to IgG4 subclass deposition in the glomerulus, all patients were divided into the IgG4-positive group (n=30) and the IgG4-negative group (n=59). The demographic, clinical and histological data at renal biopsy are shown in table 1.
Baseline and follow-up data of patients with lupus nephritis in the IgG4-negative group and IgG4-positive group
There were no significant differences in age, gender, anti-dsDNA positivity, levels of haematuria, urine protein, SCr, eGFR, WCC, HB, PLT, complement C3 and C4, and IgG, and SLEDAI score between the IgG4-positive group and the IgG4-negative group. Patients in the IgG4-positive group had lower serum albumin level (25.06±8.61 g/L vs 28.29±6.31 g/L, p=0.05). For renal pathological changes, there were no differences in the percentage of glomerular sclerosis and crescent between the groups. Patients in the IgG4-positive group had more class V LN (including Ⅲ/Ⅳ+Ⅴ, 60.0% vs 35.6%, p=0.03), more positive PLA2R staining (43.3% vs 18.6%, p=0.01) and more IgG1 deposits (96.7% vs 64.4%, p=0.01), but less C3 deposits (46.7% vs 72.9%, p=0.02), compared with those in the IgG4-negative group. For the deposition sites under EM, two patients in the IgG4-negative group had no glomerulus and one patient exhibited sclerotic glomeruli under EM, while all the other patients in both groups had multisite deposits under EM (≥2 sites). There were 15 (50.0%) patients in the IgG4-positive group and 30 (53.6%) patients in the IgG4-negative group with subendothelial deposits (p=0.75).
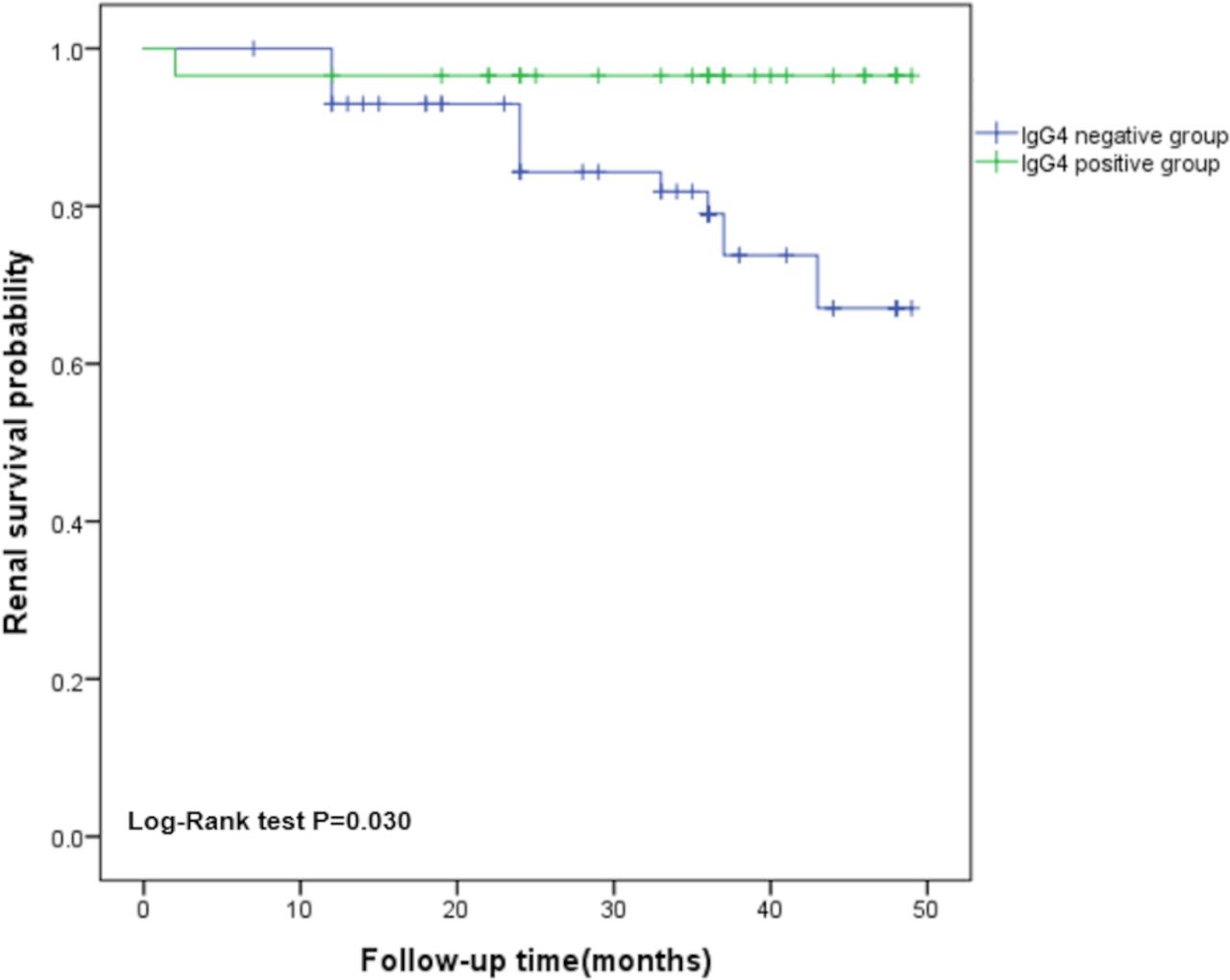
Patients in the IgG4-negative group were followed up for 30.78±11.92 months and those in the IgG4-positive group for 34.00±11.91 months (p=0.23). There was no difference in the category of immunosuppressive treatments between the groups. In the IgG4-negative group, 42 (71.1%) patients achieved CR and 4 (6.8%) patients achieved PR; in the IgG4-positive group, 17 (56.6%) patients achieved CR and 9 (30.0%) patients achieved PR. Twelve (20.3%) patients in the IgG4-negative group had renal outcome events more than that in the IgG4-positive group (one patient, 3.3%) (p=0.03). The cumulative renal survival curves by Kaplan-Meier analysis showed patients in the IgG4-positive group had better renal survival than those in the IgG4-negative group (figure 3). Multivariate Cox regression showed that high SCr (RR(relative risk)=1.005, 95% CI 1.002 to 1.008, p=0.01) and high SLEDAI score (RR=1.078, 95% CI 1.004 to 1.157, p=0.04) independently correlated with poor renal outcome, while glomerular IgG4 deposition tended to correlate with good renal outcome (RR=5.95, 95% CI 0.759 to 45.97, p=0.09).
{kind=link}
{kind=link}
{kind=link}
Cumulative renal survival rates by Kaplan-Meier analysis. Patients in the IgG4-positive group had better renal survival than patients in the IgG4-negative group (p=0.03).
We further divided patients in the IgG4-positive group into two subgroups according to PLA2R positivity in the glomerulus. As shown in table 2, there were 13 patients (43.3%) with glomerular PLA2R deposition. Patients in the PLA2R-positive subgroup had higher levels of C3 (73.08±44.68 mg/dL vs 39.82±24.16 mg/dL, p=0.03), C4 (16.58±12.19 mg/dL vs 7.41±7.40 mg/dL, p=0.02), WCC (6.56±4.75×109/L vs 3.51±1.56×109/L, p=0.04), HB (114.12±22.56 g/dL(g/L) vs 93.94±22.69 g/dL(g/L), p=0.02) and PLT (212.62±62.25×109/L vs 140.12±48.75×109/L, p=0.01), but less C3 deposits (23.1% vs 64.7%, p=0.02), less IgA deposits (30.8% vs 82.4%, p=0.01), less IgG2 deposits (53.8% vs 94.1%, p=0.01) and less IgG3 deposits (53.8% vs 82.4%, p=0.04) than those in the PLA2R-negative subgroup. Patients in the PLA2R-positive subgroup had a tendency of lower SLEDAI scores compared with those in the PLA2R-negative subgroup (10.31±4.38 vs 13.29±4.18, p=0.07). There were no significant differences in treatment response and renal outcome events between these two subgroups.
Baseline and follow-up data of patients with lupus nephritis with IgG4 deposits in the PLA2R-negative subgroup and PLA2R-positive subgroup
Discussion
IgG4 deposition in the glomerulus is widely reported to be associated with idiopathic MN. In a previous clinical analysis, IgG4 deposition was also found in different classes of LN, but the deposition rate was significantly lower than that of primary MN.9 In our study, 33.7% of patients with LN had glomerular IgG4 deposition, and among them 60% were diagnosed as class V or combined with class V LN. However, a part of patients with class III/IV LN also had positive IgG4 staining. In cases of class V LN or combining with class V LN, the IgG4 positive rate is 46% (18 of 39), while in patients with class Ⅲ/Ⅳ LN the positive rate is 25% (12 of 48). Therefore IgG4 positivity may not be a good indicator of the presence of an MN pattern. However, we found glomerular IgG4 deposition tended to correlate with good renal outcome in LN. It may predict better renal survival in patients with LN.
IgG4 cannot induce a predominant immune response and is defined as a non-inflammatory molecule.15 Human IgG4 exploits additional properties to modify immune responses, such as dynamic Fab-arm exchange, which results in the formation of bispecific IgG4 antibodies,16 17 and the interaction with the Fc part of other IgG subclass antibodies.18–22 Both mechanisms may contribute to human IgG4-mediated suppression of the hexamer formation by other IgG subclasses. van der Zee et al23 reported that in the blood of beekeepers, the IgG4 antibody of phospholipase A effectively inhibited complement activation by inhibiting the binding of C1q to IgG1. Zuo et al24 showed that administration of XVII collagen (Col17)-specific human IgG4 autoantibodies (from autoimmune patients with bullous pemphigoid skin disease) to humanised Col17 mice inhibited the complement activation and disease development by interfering with other IgG subclasses. Another study showed that IgG4 binds to the Fc portions of IgG1, IgG2 and IgG3 and blocks the Fc-mediated effector functions of IgG1 and IgG3 complexes and may assist in the clearance of ICs by forming larger complexes that are more effectively cleared, resulting in termination of the inflammatory process.16 In patients with SLE and in lupus-prone MRL-lpr mice, Pan et al25 revealed that IgG4 autoantibody (antinuclear IgG4) attenuates SLE disease progression and suppresses complement consumption and inflammatory cytokine production by competitively binding to autoantigens to form non-pathogenic ICs that result from the low affinity of IgG4 for both the Fcγ receptor and the C1 complement molecule. Pan et al26 also reported that serum antinuclear IgG4 in patients with SLE was positively correlated with C3 and negatively correlated with 24-hour urinary protein. The ratio of the deposition score for IgG4 (IgG1+IgG2+IgG3+IgG4) was negatively correlated with the score for C1q and C3 deposition in LN, which means IgG4 autoantibody may dampen the inflammatory response in SLE and thus may provide a novel therapeutic target for SLE.26
PLA2R, a transmembrane receptor in glomerular podocytes, is the major target antigen in idiopathic MN. Anti-PLA2R antibodies frequently consist of the IgG4 subtype, and glomerular capillary IgG4 deposition is a potential marker in the differentiation of primary MN from secondary MN.27 In idiopathic MN, most patients have IgG4 and PLA2R deposition in the glomerulus at the same time. A study by Kaya et al27 reported that 46.9% of patients with idiopathic MN had IgG4 and PLA2R dual-positive staining in the kidney. Another study showed that 88.3% of patients with idiopathic MN simultaneously had PLA2R and IgG4 deposition in the glomeruli. Patients with MN with positive PLA2R expression may respond to glucocorticoid and/or immunosuppressant therapy,28 while Qin et al29 reported that sustained PLA2R deposits in kidney tissue correlated with low spontaneous remission, low response to immunosuppressants or increased disease relapse. Membranous LN usually presents anti-PLA2R-negative, although cases of PLA2R-positive membranous LN have been reported,30 31 while the relationship between the PLA2R and IgG4 staining patterns and treatment response of patients with LN was not mentioned in the previous study.
In the present study, we found that 14.6% of patients with LN had both IgG4 and PLA2R staining, and among these patients 76.9% were diagnosed as class V LN. It may be difficult to differentiate class V LN and primary MN in renal pathology. In our study, 21 patients were diagnosed as class V LN. All of them had IC deposits in multiple sites of glomerulus. Among them, 2 (9.5%) patients had subendothelial, subepithelial, mesangial and intra-GBM deposits; 16 (76.2%) patients had subepithelial, mesangial and intra-GBM deposits; 3 (14.3%) patients had subendothelial, mesangial and intro-GBM deposits; and 2 (9.5%) patients had subepithelial and intra-GBM deposits. In view of the above pathological features, we diagnosed these patients as class V LN rather than primary MN, even though a part of them had PLA2R deposition. Such cases were also reported by Garcia-Vives et al,32 where circulating anti-PLA2R antibodies were detected in 7 of 37 patients with membranous LN (18.9%), of whom 5 also had positive glomerular immunohistochemistry staining for PLA2R. We further found that patients with LN with both PLA2R and IgG4 deposits in the glomerulus had higher levels of serum C3 and C4 and a tendency of lower SLEDAI scores than those with positive IgG4 but negative PLA2R staining. Also, for pathological changes, the glomerular deposits of C3, IgA, IgG2 and IgG3 were lower in patients with LN with both PLA2R and IgG4 deposits. These findings showed that patients with LN with IgG4 and PLA2R dual-positive staining in the glomerulus might have low disease activity.
There are several limitations to this study. First, this is a retrospective study with a relatively small size of cases. Second, for the relatively short follow-up period, we need longer follow-up time to determine the effect of IgG4 deposition on long-term prognosis of LN. Third, because we only included cases at our centre, our pathological techniques and diagnostic inertia may cause bias.
In conclusion, patients with LN with glomerular IgG4 deposits may have better renal survival, and patients with LN with simultaneous glomerular IgG4 and PLA2R deposits may have low disease activity.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang University School of Medicine (no: 2020571). Informed consent was not obtained from the patients of this study, as approved by the Ethics Committee. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank all clinicians at the Kidney Disease Center, First Affiliated Hospital, College of Medicine, Zhejiang University, for their efforts in this study.
References
Footnotes
Contributors All authors were involved in analysing and interpreting the data, drafting the article and revising it critically for important intellectual content, and all read and approved the final version to be published. FH is the guarantor.
Funding This is supported by the National Natural Science Foundation of China (no: 82104586; to XJ) and the Primary Research and Development Plan of Zhejiang Province (2020C03034; to FH).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.