Article Text

Abstract
Objective Depression is common in individuals with chronic cutaneous lupus erythematosus (CCLE). However, how CCLE may impact patients’ psychological well-being is poorly understood, particularly among disproportionally affected populations. We examined the relationships between depression and psychosocial factors in a cohort of predominantly Black patients with primary CCLE (CCLE without systemic manifestations).
Methods Cross-sectional assessment of individuals with dermatologist-validated diagnosis of primary CCLE. NIH-PROMIS short-forms were used to measure depression, disease-related stigma, social isolation and emotional support. Linear regression analyses (ɑ=0.05) were used to test an a priori conceptual model of the relationship between stigma and depression and the effect of social isolation and emotional support on that association.
Results Among 121 participants (87.6% women; 85.1% Black), 37 (30.6%) reported moderate to severe depression. Distributions of examined variables divided equally among those which did (eg, work status, stigma (more), social isolation (more), emotional support (less)) and did not (eg, age, sex, race, marital status) significantly differ by depression. Stigma was significantly associated with depression (b=0.77; 95% CI0.65 to 0.90), whereas social isolation was associated with both stigma (b=0.85; 95% CI 0.72 to 0.97) and depression (b=0.70; 95% CI0.58 to 0.92). After controlling for confounders, stigma remained associated with depression (b=0.44; 95% CI0.23 to 0.66) but lost significance (b=0.12; 95% CI −0.14 to 0.39) when social isolation (b=0.40; 95% CI 0.19 to 0.62) was added to the model. Social isolation explained 72% of the total effect of stigma on depression. Emotional support was inversely associated with depression in the univariate analysis; however, no buffer effect was found when it was added to the multivariate model.
Conclusion Our findings emphasise the psychosocial challenges faced by individuals living with primary CCLE. The path analysis suggests that stigmatisation and social isolation might lead to depressive symptoms. Early clinical identification of social isolation and public education demystifying CCLE could help reduce depression in patients with CCLE.
- Quality of LIfe
- Epidemiology
- Outcome Assessment, Health Care
- Autoimmune Diseases
Data availability statement
Data are available on reasonable request. Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Individual de-identified data provided in this report are available on a data use agreement.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Discoid lupus erythematosus (DLE) and other chronic cutaneous lupus erythematosus (CCLE) conditions often cause substantial skin disfigurement, which may have a negative impact on patients’ mental health. These conditions are less likely to overlap with systemic manifestations, compared with other cutaneous lupus erythematosus (CLE) types, and people with black or brown skin are disproportionately affected by DLE. However, the burden of depression and its psychosocial pathways are poorly understood in individuals with CCLE, particularly among those from minority groups that have primary CCLE without systemic manifestations.
WHAT THIS STUDY ADDS
Our study establishes that approximately one-third of participants in a cohort of predominantly Black patients with primary CCLE self-reported moderate to severe depression. Findings suggest that disease-related stigma and social isolation may play important roles in depression pathways among these patients. Emotional support did not show a significant buffer effect, suggesting that depression may have profound roots in social detachment, which, in turn, may be driven by internalised stigma.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our findings underscore the importance of increased clinical attention to diagnosis and management of depression among patients with CCLE as well as suggesting additional intervention points that might prevent depression from occurring. Early identification of patients experiencing social isolation and social stigma, combined with effective interventions to address these factors could potentially prevent these patients from deeper social withdrawal and development of depression. Additionally, public health campaigns that raise awareness about these potentially disfiguring conditions may help to reduce the social stigma and mitigate the psychosocial impact of CCLE on affected individuals.
Introduction
Cutaneous lupus erythematosus (CLE) is a group of autoimmune disorders categorised into acute, subacute (SCLE) and chronic (CCLE) cutaneous lupus erythematosus.1
CCLE is the largest subgroup, with conditions prone to cause substantial disfigurement on visible skin, negatively impacting patients’ mental health and social life. Classical discoid lupus erythematosus (DLE), the most common distinctive CCLE form, is characterised by lesions largely localised on the scalp and face that heal causing skin dyspigmentation, atrophy, scarring and permanent hair loss.1–3 Furthermore, DLE lesions are more likely to be noticeable in people with black or brown skin, a population that is disproportionately affected by this condition and has an earlier onset of skin damage relative to Whites.4 In metropolitan Atlanta, where the population is evenly distributed between Whites and Blacks, we reported the overall incidence rate of CCLE and DLE at a minimum of 3.9/100 000 and 3.7/100 000 person years, respectively.5 CCLE and DLE incident rates were 3.9-fold and 4.1-fold higher for Blacks compared with Whites, respectively.
Healthy People 2030, the nation’s health objectives, addresses the prevention, screening, assessment and treatment of mental disorders and behavioural conditions, acknowledging that some populations are disproportionately affected by mental illnesses.6 Clinical conditions that have skin manifestations increase the risk of depression.7 Notably, the emotional impact of having a cutaneous disorder was found to be significantly higher in patients with CLE compared with other skin diseases.8 Depression is described in over one-quarter of patients with CLE, and healthcare costs in this population are substantially higher among those with depression.9 10 However, mental health challenges are often underdiagnosed among patients with CLE, and little is known about the mechanisms that lead to depression in this population.11 Because most studies have included patients with all types of CLE and overlapping systemic lupus erythematosus (SLE), the burden and pathways of depression remain poorly understood among those with primary CCLE.
Stigma is defined by the WHO as ‘a mark of shame, disgrace or disapproval which results in an individual being rejected, discriminated against, and excluded from participating in a number of different areas of society’. Stigma plays a role in depression for conditions as diverse as psoriasis, HIV, epilepsy and mental illnesses.12–15 Internalised shame and perceived stigma correlate with depression, and stigma has been linked to social isolation and other maladaptive responses, increasing the risk of poor mental health outcomes.12 13 16
In patients with SLE, both cutaneous involvement and stigma were found to be associated with depression,8 and stigma has contributed to low self-esteem and isolation from social activities in this population.17 We previously reported a 26% prevalence of moderate to severe depressive symptoms in a predominantly Black population-based cohort of patients with primary CCLE.18 Our work also underscored an inverse association between emotional support and depression, suggesting that social factors play a role in the pathogenesis of depression among individuals with CCLE.18 Despite the high prevalence of depression in patients with CLE in general and CCLE in particular, sparse literature explores psychosocial pathways in high-risk populations with primary CCLE.
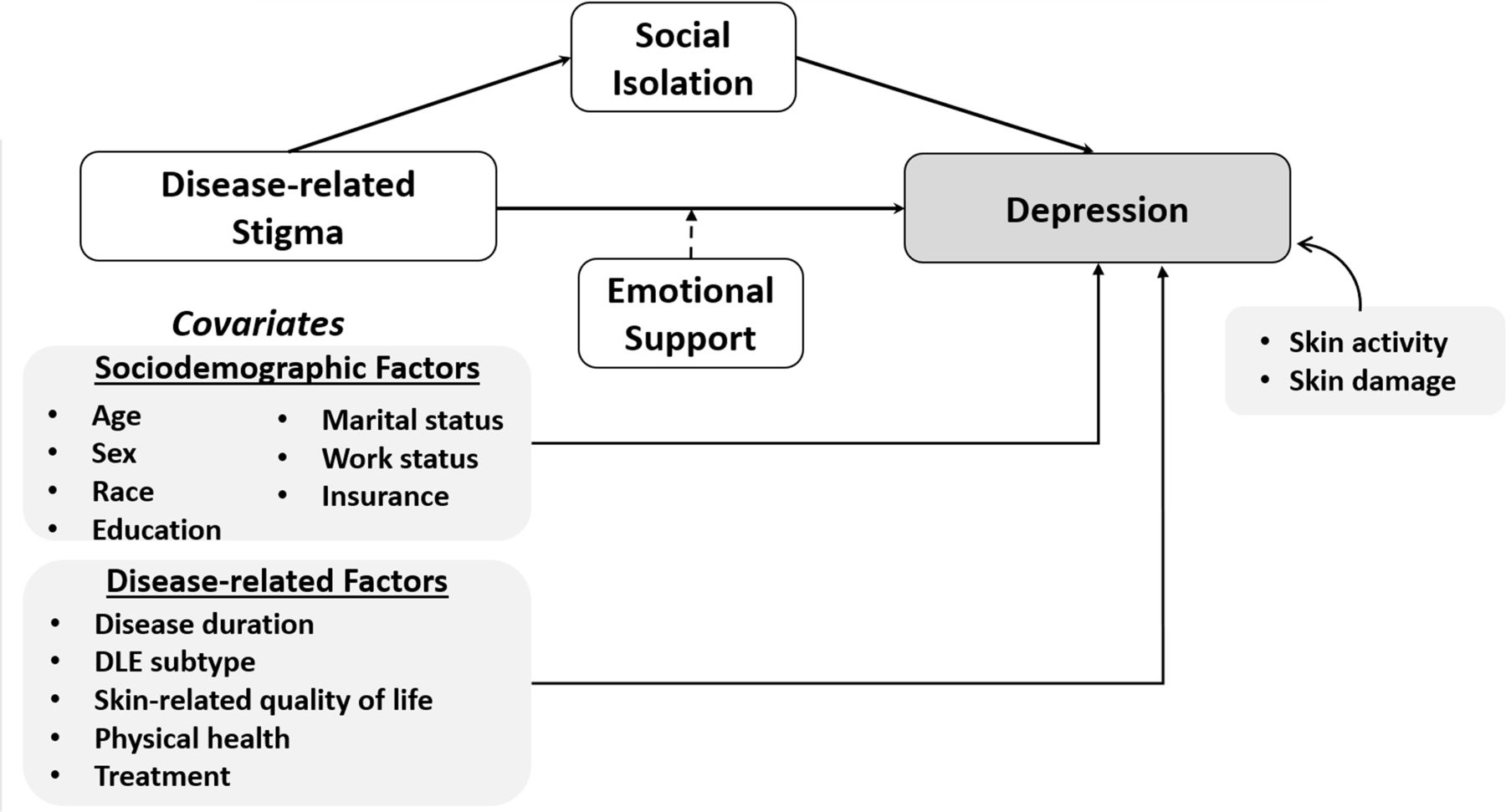
Understanding the relationships between stigma, social isolation, emotional support and depression is critical to developing interventions that facilitate non-stigmatising awareness and reduce stigma stress among people with CCLE. The inclusion of Black individuals, who are disproportionately stricken by CCLE, have worse outcomes, and have been historically underrepresented in lupus research is imperative to develop these interventions. We examined the relationships between depression and illness-related stigma in a cohort of predominantly Black patients with primary CCLE using descriptive statistics. Additionally, we explored the role of social isolation and emotional support in that relationship by testing an a priori path derived from a novel conceptual model of stigma in visible skin diseases (figure 1).19 Specifically, our objectives were to: (1) establish the independent association between stigma and depression, (2) test for potential mediation of this relationship through social isolation and (3) test for moderation of this relationship by degree of emotional support.

{kind=link}
Conceptual model of the study. We examined the relationship between stigma (main exposure) and depression (outcome) after controlling for covariates. Social isolation was evaluated as a potential mediator of the stigma-depression relationship, and emotional support as a potential buffer. In addition, we analysed the association of skin activity and skin damage on depression in a subset of participants. DLE, discoid lupus erythematosus.
Methods
Population
Georgians Organized Against Lupus (GOAL) is a population-based cohort of predominantly Black individuals with dermatologist-validated lupus supported by the Centers for Disease Control and Prevention (CDC). Its overall aim is to examine the impact of social determinants of health outcomes relevant to patients, healthcare providers and policy makers. Recruitment and data collection methods have been previously described.20 Briefly, GOAL initially recruited patients with SLE from the Georgia Lupus Registry (GLR). The GLR is a population-based registry funded by CDC to estimate the incidence and prevalence of SLE in Atlanta, Georgia, where there is a large, socioeconomically diverse Black/White population.21 22 In 2015, GOAL received CDC funding to enrol patients with CCLE or SCLE. Sources of recruitment have been the GLR, community and academic dermatology practices, and self-referrals through the Lupus Foundation of America, Georgia Chapter.
For this cross-sectional study, we selected GOAL participants with primary CCLE through a diagnosis validation process including medical records review, physician-assessment and review of pictures. Classification of CCLE required either a well-documented diagnosis of DLE, lupus panniculitis (LEP), lupus tumidus (LET) or chilblain lupus (ChLE) by a board-certified dermatologist or a skin-examination±photographs compatible with CCLE subtypes according to a study dermatologist’s (LA) review. To focus on primary CCLE, we excluded those participants with a rheumatologist-documented diagnosis of SLE and/or those who fulfilled ≥4 American College of Rheumatology criteria for SLE.23 The Emory University Institutional Review Board, the Grady Health System Research Oversight Committee and the Georgia Department of Public Health Review Board approved the study. All participants provided informed consent.
Patient and public involvement
We convened a diverse group of GOAL participants into the Lupus Patient Advisory Research Council (L-PARC); members meet at least once a year with researchers to provide advice on recruitment, retention, study measures and dissemination of findings.
Measures
Patient-reported responses collected from March 2020 through September 2021 were analysed. Patient-Reported Outcomes Measurement Information System (PROMIS) adult short forms were used to measure depression, social isolation, emotional support and overall physical health, and the Neuro-QoL system was used to assess generic disease-related stigma. These measures have been validated in patients with a variety of chronic conditions, including rheumatic diseases and lupus, and are recommended for use because of their flexibility and precision.24–26 Each tool uses a 5-point Likert scale. Raw scores were individually calculated and converted to T-scores by the HealthMeasures Scoring ServiceSM,27 which rescales the raw score into a standardised score with a mean of 50 and a SD of 10. Higher scores represent more of the domain being measured.
Depression
We used the PROMIS Depression short form 8a, comprising 8 Likert-scale questions rated from 1 (never) to 5 (always) to assess negative mood (eg, sadness, guilt), views of self (eg, self-criticism, worthlessness), social cognition (eg, loneliness) and decreased positive affect and engagement (eg, loss of interest) in the past 7 days. Self-reported depression was defined as a T-score ≥60, corresponding with the analogous Patient Health Questionnaire 9 (PHQ-9) scores.28 29 This PROMIS scale has been extensively validated and was adopted by the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) as a standardised patient-reported scale that can contribute to psychiatric diagnosis, tracking of illness course and treatment planning.30 31 PROMIS Depression showed strong convergent validity with the CES-D and the PHQ-9 (with correlations in a range from 0.72 to 0.84 across three time points).32
Stigma
The Neuro-QoL Stigma short form 8 was used to evaluate negative perceptions of self (eg, embarrassment), publicly enacted negativity (eg, people’s unkindness, discomfort, embarrassment) and discrimination (eg, being avoided, left out, blamed) as a result of disease-related manifestations.33 The scale has demonstrated high internal consistency, test-retest reliability and convergent correlations with expected legacy measures.34
Social isolation
We used the PROMIS Social Isolation short form 8a, rated from 1 (never) to 5 (always), to assess perceptions of loneliness, being avoided, excluded, detached, disconnected from or unknown by others. The scale has demonstrated very good internal consistency reliability, with Cronbach’s alpha=0.860.35
Emotional support
The PROMIS Emotional Support short form 4a was used to assess perceived feelings of being cared for and valued as a person and having confidant relationships.
Sociodemographic covariates
Self-reported data on sociodemographics that may be associated with depression included age, sex, race/ethnicity, years of education, marital status, employment and living below the poverty level (calculated using the U.S. Census Bureau’s 2011 estimates as cut-off for 100% poverty threshold.36
Disease-related covariates
Distribution of DLE lesions was determined by clinical assessment or medical record review and classified as being localised (above the neck) or generalised (above and below the neck).1 Skindex 29+3, a validated skin-specific quality of life instrument for people with CLE, was used to assess the severity of cutaneous symptoms (eg, itching, burning, irritation), the impact of the condition on functioning (eg, relationships, work, sleeping) and a lupus-specific domain (eg, limited outdoor activities, worried about hair loss, worried about flares related to sun exposure).37 38 The Skindex emotions scale was not analysed because it includes several questions about depression. Scores for each Skindex domain range from 0 to 100, with 100 indicating a poorer quality of life. In addition, we collected self-reported data on disease duration and treatment, including hydroxychloroquine or other antimalarial drugs, local steroids (topical or intralesional), systemic steroids and/or immunosuppressive drugs (oral or intravenous).
A subset of 59 participants were also evaluated with the Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI), a validated physician-based measure to score the severity of cutaneous lupus.39 Separate CLASI activity and CLASI damage scores were calculated, with higher scores (range 0–70 for activity and 0–56 for damage) indicating more severe disease.
Global physical health was measured using the PROMIS Global-10 SF, a high-reliability scale to assess physical health, physical function, pain and fatigue.40 41
Statistical analysis
Descriptive statistics were calculated to characterise the sample overall and among those with and without depression. Distributions for categorical variables were generated as number and per cent; continuous variables were expressed as mean and SD.
Figure 1 illustrates the conceptual model used to guide the path analysis. Linear regression was used to examine the relationship between stigma (main exposure), social isolation (potential mediator) and emotional support (potential moderator) with depression (outcome). The mediator effect of the stigma-depression relationship was tested using the four steps outlined by Baron and Kenny (online supplemental table 1).42 The first step was conducted through linear regression analysis to examine the relationship between stigma and depression. We then regressed separately social isolation on stigma and depression on social isolation (steps 2 and 3).
Supplemental material
Multivariable regression was used to determine whether the association between stigma and depression remained significant after controlling for sociodemographics and disease-related covariates, which were entered in blocks (depicted in online supplemental table 3, Models 1 and 2, respectively). For the fourth step of Baron and Kenny (online supplemental table 1), stigma and social isolation were tested simultaneously, controlling for all other covariates (online supplemental table 3, Model 3). Per this approach, mediation was established if the first three steps were shown to be significant, and the effect of stigma on depression was reduced when social isolation was entered in the model. Then, we estimated the extent to which social isolation contributed to the total effect of stigma on depression after adding emotional support (online supplemental table 3, Model 4) and performed the Sobel’s z-test on the significance of the mediation effect.43 Finally, we tested whether emotional support had a moderation effect on the association between depression and stigma by entering the interaction term stigma*emotional support. We built two final models by including and excluding the DLE subtype covariate, thus testing both the DLE sample (table 3, Model 1) and the whole CCLE sample (table 3 Model 2), respectively. We used R2 to measure the percentage of the variance in depression explained by all variables in each model and conducted posthoc tests of normality of residuals, heteroskedasticity, linearity and multicollinearity. We found no evidence for influential observations or outliers. We separately analysed participants with CLASI data to assess whether skin activity and skin damage were associated with depression. Statistical significance was set at ɑ=0.05 for descriptive analyses and non-overlapping 95% CI for regression analyses. All analyses were conducted in SAS V.9.4.
Results
We evaluated responses from 121 GOAL participants who had a documented diagnosis of primary CCLE (87.6% women and 85.1% self-identified as being Black). Of those, 109 had DLE (13 with another CCLE subtype) and 12 had other CCLE subtypes (LEP=5, LET=5, ChLE=2). DLE lesions were localised in 74 participants, generalised in 34 and 1 participant had missing data on location. Except for a higher proportion of Black individuals among those with DLE (89.9%) compared with those with other CCLE subtypes (41.7%), sociodemographics, psychological factors and disease-related factors were similar between both groups.
Thirty-seven (30.6%) participants reported moderate to severe depressive symptoms (PROMIS Depression T-score≥60). Descriptive characteristics for the overall sample and by depression status are shown in table 1. Mean age and disease duration were 54.1 (SD=13.8) and 14.2 (SD=10.0) years, respectively. No statistically significant differences by depression were observed for age, sex, race, marital status, insurance or disease duration. Participants with depression had significantly less years of education (mean=13.4, SD=2.6) compared with those without depression (mean=15.0, SD=3.2). Nearly 60% combined were either unemployed/disabled (31.9%) or out of the labour force (26.7%), while 41.4% were working either full-time or part-time. Employment status differed significantly by depression, with 51.4% of depressed participants being unemployed or disabled, compared with 23.5% of those without depression.
Description of the CCLE sample, overall and by depression
For all three psychosocial factors, those with depression had significantly worse values than those without: more stigma (mean=60.9 vs mean=47.0); more social isolation (mean=59.5 vs mean=45.6); lower emotional support (mean score=47.8 vs mean=53.3).
For disease-related factors, among the subgroup with DLE (n=108), generalised lesions occurred in 50% of depressed, compared with 23.7% of non-depressed, participants, p=0.012. Compared with participants without depression, depressed participants had significantly higher (worse) scores of Skindex symptoms (mean=59.2 vs mean=35.3), functioning (mean=57.8 vs mean=21.2) and the CLE-related domain (mean=83.6 vs mean=52.4).
Overall mean score for physical health was 41.4; patients with depression reported significantly worse physical health (mean=34.5) compared with those without depression (mean=44.9). Over half (59.5%) of participants were on hydroxychloroquine, 50.4% reported treatment with local steroids and 21.5% were on oral steroids or immunosuppressive drugs. A significantly higher proportion of depressed participants (81.1%) were on hydroxychloroquine, compared with non-depressed (50%); no statistically significant differences were found for other treatments by depression.
Among 59 participants with CLASI, overall mean scores were 4.5 for activity and 12.7 for damage, respectively, and did not differ by depression. We did not find a significant linear association between either skin activity or skin damage scores and depression (online supplemental figures 1 and 2). CLASI-assessed participants were more likely to be Black and uninsured, compared with others, but remaining demographics, in addition to depression, stigma, social isolation and emotional support scores were similar between both groups (online supplemental table 2).
The relationships between psychosocial exposures and depression are shown in table 2. Stigma and social isolation were significantly associated with higher depression (b=0.77; 95% CI 0.65 to 0.90 for stigma, and b=0.70; 95% CI 0.58 to 0,82 for social isolation), whereas the slope of depression decreased significantly with higher emotional support (b=−0.45; 95% CI −0.65 to –0.25).
Linear regression of depression on stigma, social isolation and emotional support
To examine the potential mediation effect of social isolation, social isolation was regressed on stigma (step 2 of Baron and Kenny), showing a statistically significantly association (b=0.85; 95% CI0.72 to 0.97).
Our hypothesis that there was a significant direct association between stigma and depression was supported by the multivariate regression analysis (online supplemental table 3, Model 1: b=0.75; 95% CI 0.62 o 0.89, after controlling for sociodemographics). Disease-related covariates were then added as a block for further controlling. The Skindex functioning domain was not included due to the multicollinearity with stigma (variance inflations (VIF)>5). The slope of depression regressed on stigma decreased; however, the association remained significant (online supplemental table 3, Model 2: b=0.44; 95% CI 0.23 to 0.66).
We then tested together stigma and social isolation, after controlling for covariates. In this model, the adjusted slope of depression regressed on social isolation slightly decreased, but the association remained statistically significant (online supplemental table 3, Model 3: b=0.40; 95% CI 0.19 to 0.62). Moreover, the effect of stigma on depression was reduced from b=0.44 (95% CI 0.23 to 0.66) to b=0.12 (95% CI −0.14 to 0.39) and was no longer significant, supporting a mediation effect of social isolation in the multivariate model (online supplemental table 3, Model 4). Sobel’s z-test rendered a significant mediation effect with 71.4% and 72% (p<0.001) of the total effect of stigma being mediated by social isolation after controlling for sociodemographic and disease covariates (online supplemental table 3, Models 3 and 4).
Our hypothesis that emotional support would have a moderating effect on the relationship between social isolation and depression was not supported. Emotional support was negatively associated with depression, but the association was not statistically significant (online supplemental table 3, Model 4: b=−0.00; 95% CI −0.17 to 0.17). The effect of each social isolation (b=0.40; 95% CI 0.19 to 0.62) and stigma (b=0.12; 95% CI −0.14 to 0.39) on depression did not change when emotional support was added to the model. Furthermore, we added the interaction term emotional support*stigma (table 3, Model 1), confirming that emotional support did not have a significant effect (b=0.01; 95% CI −0.01 to 0.03). The effect of social isolation on depression remained statistically significant with a similar slope (b=0.38; 95% CI 0.16 to 0.60) after adding the interaction. When we tested the final model in the whole CCLE sample, the results remained similar after excluding the DLE subtype covariate (table 3, Model 2).
Multivariate regression models of depression by stigma, social isolation and emotional support
Depression scores were directly associated with never married (vs currently married) and inversely associated with better physical health showing statistically significant p values in all multivariate models. Variables in Models 3, 4 and 5 explained 72% of the variance for depression, as indicated by R2 values.
Discussion
Our findings demonstrated a significant association between stigma and depression in patients with primary CCLE. Path analysis indicates that the association diminished significantly but did not disappear when social isolation was included in the model. Therefore, social isolation may partially mediate the relationship between depression and stigma, which presents additional valuable up-stream intervention opportunities.
CCLE disproportionately strikes women and Black individuals and typically starts at young ages.5 Individuals with these conditions suffer from changes in their physical appearance, with scarring lesions predominantly located on the scalp, face and hands, leading to high levels of psychological distress as these visible lesions are not easily covered.2 44 Psychological health is one of the most negatively impacted domains in the quality of life of patients with CLE.8 45 46 A recent study that used administrative data from a household sample in the U.S. Medical Expenditure Panel Survey estimated a 29.5% prevalence of depression among people with CLE.10 Likewise, the risk of depression was found to be twofold higher in people with CLE compared with the general population in a nationwide Danish study.9
In this predominantly Black population-based cohort, approximately one-third of participants with primary CCLE self-reported moderate to severe depression. Moreover, we found a direct relationship between depression and a non-specific measure of illness-related stigma, suggesting that depression can be primarily driven by negative perceptions of self and discrimination as a result of the disease. Perceptions of stigmatisation have been significantly related to both psychological distress and degree of disability among patients with other skin conditions.47
Our conceptual model was supported by statistically significant evidence consistent with our hypothesis that social isolation may be an important mediator in the relationship between stigma and depression in individuals with CCLE. Prior reports suggest that social withdrawal is a major effect of internalised stigma in individuals with skin and other stigmatising conditions.15 Stigma caused by altered skin appearance and, possibly, the need to avoid the outdoors because of photosensitivity, predispose CCLE to be a socially isolating disease.2 4 45 48 49 However, little is known about the link between stigma, social isolation and depression in skin conditions. A recent study among older Americans indicates that social disconnectedness predicted subsequent perceived isolation, whereas feelings of loneliness or isolation increased the risk of depression.50 Similarly, our findings suggest that patients with CCLE may isolate themselves to cope with their perceptions of stigmatisation, which may lead to psychological distress, more profound isolation and depression. Recent findings also suggest that higher perceived social support may lower the risk of psychological distress in patients with psoriasis.16 Although depressed patients in our study reported lower emotional support, having higher emotional support did not buffer the effect of social isolation on depression. This finding is perhaps less surprising when considering that the prevalence of depression did not differ by marital status. However, in the multivariate models, the slope of depression increased significantly (approximately 4.5–5.1 points higher) in participants who reported never being married, compared with those currently married. These findings taken together suggest that marriage itself might provide greater combined resources and social support,51 whereas stigma is a process of social devaluation causing diminished self-esteem and social isolation. More sensitive measurement instruments and complex interventions may be needed among those who already have internalised stigma.
Patients with generalised DLE (lesions above and below the neck) did have a significantly higher rate of depression, compared with those with localised DLE (lesions above the neck). However, in the multivariate analysis, we did not find a significant linear association between having lesions above and below the neck and depression scores. Moreover, the association between depression and the main exposures remained similar for the whole CCLE sample when the DLE subtype was excluded as a covariate. These data support the complex pathways implicated in the psychological impact of living with CCLE.
Younger age was independently associated with depression in our cohort, paralleling the age-related psychological vulnerability described in the general population.52 We also found a significant relationship between depression and self-reported physical health; however, neither skin activity nor damage showed a significant correlation with depression in a subset of 59 CCLE participants who had CLASI scores. Thus, our data support the multifactorial nature of depression in patients with CCLE, suggesting that patients perceptions may play a more critical role than clinical factors.53 Interestingly, in a Latino population, perceived discrimination was found to be inversely associated with self-reported physical health, and depression partially accounted for the association.54 Longitudinal studies are warranted to determine whether depressive symptoms in patients with CCLE are primarily driven by perceived stigmatisation and reduced social connections, which in turn can lead to physical and functional impairment, perpetuating the maladaptive response.
Our study has limitations. First, the cross-sectional design does not allow causal interpretations or to assess a temporal precedence of the mediation. This study also relies on self-report measures, which have known limitations. However, we used validated patient-reported outcomes measures, which have been called for by the WHO and NIH to allow the participants to characterise their experience, perceptions and outcomes of living with a disease.55 The population-based nature of the cohort also limited our ability to clinically assess all participants for skin activity and damage, which may lead to depression. However, we did not find a significant linear association between either CLASI activity or CLASI damage and depression scores in a subset of 59 participants. These results are consistent with previous findings indicating a poor correlation between physician-rated severity and psychiatric morbidity in dermatological outpatients.53 However, because the CLASI-scored subset was a small sample size, our results cannot be generalised to the rest of the cohort. We were able to explain 72% of variance in depression; however, we cannot exclude residual and unmeasured confounding. Moreover, our findings may be confounded by the order and function of the constructs in the regression models. The constructs were analysed based on the assumption that stigma, social isolation and emotional support have a critical role in depression among individuals with CCLE. Our results are applicable to a predominantly Black CCLE sample from the Southeastern USA and cannot be generalised to other populations. Future longitudinal studies can help to elucidate the causal direction of the associations that we found and provide context for understanding psychosocial pathways and mental health in patients with CCLE.
Our study also has several strengths, including extending the literature by focusing our analyses on patients with CCLE. Prior studies included patients with all CLE types; consequently, the burden and pathways of psychological distress in those with CCLE remained unknown. Second, in contrast to previous studies, which predominantly involved White patients, we examined a largely Black cohort of individuals with primary CCLE. Blacks have higher susceptibility to CCLE,5 but these patients, particularly those with DLE, also have more noticeable ear and scalp dyspigmentation and scarring alopecia than Whites.56 Therefore, the psychological impact may be greater in this population. Third, as opposed to other academic-based cohorts, our CCLE participants were recruited from multiple sources, including community practices, allowing us to conduct a ‘real-world’ assessment. Fourth, by focusing on people with CCLE without SLE, we were able to reduce the confounding effect of SLE manifestations on depression. Fifth, our study is the first to our knowledge to propose, test and provide initial evidence for psychosocial pathways to depression in a largely Black population with primary CCLE, creating opportunities for both confirmatory research and upstream interventions.
In conclusion, our findings underscore that people living with CCLE are at risk for experiencing adverse effects of stigma, social isolation and depression and present a theoretical model explaining potential pathways in the relationships between these psychosocial effects. In addition to providing a blueprint for longitudinal research to test this promising model, these findings are essential to inform clinical, social and individual interventions. Healthcare workers serving patients with CCLE should be aware of the high prevalence of stigma, social isolation and depression in this population and be trained to conduct early screenings and referrals to mental health services. Ideally, these findings could delay, reduce or prevent depression in this population by pushing interventions upstream to when patients are experiencing ‘warning signs’ of stigma and social isolation. Campaigns to educate patients’ family members and friends as well as the general public about the disease are needed as a parallel effort to reduce sources of social stigma. Moreover, psychoeducation and peer support may help reduce internalised stigma, enhance social interactions and minimise the psychosocial impact of living with these visible conditions.
Data availability statement
Data are available on reasonable request. Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Individual de-identified data provided in this report are available on a data use agreement.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Emory Institutional Review Board; Study number 00003656. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank the GOAL Research Coordinators for their support of the GOAL Cohort as well as Grady Memorial Hospital and the lupus patients who participate in our research.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors have contributed to the preparation of the manuscript. CD, LA, TTL, CD-T, GB and SSL have contributed to the study design and/or data collection. CD serves as guarantor and is responsible for the overall content.
Funding The GOAL Cohort is supported by the Centers for Disease Control and Prevention (CDC) Grants U01DP005119, U01DP006488. SSL and CD are supported by the NIH (R01AR065493-01; R01MD010455-01; R01AR070898-01) and the CDC (U01DP005119). This publication was supported by the Centers for Disease Control and Prevention of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award totalling $6 406 636 with 100 percentage funded by CDC/HHS and $0 amount and 0 percentage funded by non-government source(s).
Disclaimer The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by CDC/HHS, or the U.S. Government. A license to use the Skindex 29+3 was provided by Mapi Research Trust.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.