Article Text

Abstract
Objective To characterise disease control and remission in patients with SLE receiving belimumab for up to 12 months in the real world.
Methods This post hoc analysis (GSK Study 213502) used data from the US evaluation Of use of Belimumab in clinical practice SEttings (OBSErve) study (GSK Study 117295), an observational cohort study of adults with SLE initiating and continuing belimumab for ≥6 months. Data were collected every 6 months by physician chart review; details of disease activity using the Safety of Estrogens in Lupus Erythematosus National Assessment–SLE Disease Activity Index (SELENA-SLEDAI) score were collected if routinely used by physicians. Disease control definitions evaluated were SELENA-SLEDAI score of ≤2 at 12 months, SELENA-SLEDAI score of ≤2 and glucocorticoid (prednisone equivalent) dose of ≤5 mg/day at 12 months, SELENA-SLEDAI score of ≤2 and glucocorticoid dose of ≤5 mg/day at both 6 and 12 months. Disease remission definition was SELENA-SLEDAI score=0 at 12 months. Glucocorticoid dose during follow-up was quantified.
Results US OBSErve enrolled 501 patients, 90 of whom had eligible SELENA-SLEDAI scores for inclusion in this analysis. Mean (SD) SELENA-SLEDAI scores were 13.1 (3.0) at baseline and 4.9 (3.4) at 12 months. Disease control at 12 months was achieved by 31.1% of patients when defined as a SELENA-SLEDAI score of ≤2 (95% CI 21.8 to 41.7); this decreased to 25.6% when requiring a SELENA-SLEDAI score of ≤2 and glucocorticoid dose of ≤5 mg/day (95% CI 16.9 to 35.8) and 17.8% when requiring a SELENA-SLEDAI score of ≤2 and glucocorticoid dose of ≤5 mg/day at both 6 and 12 months (95% CI 10.5 to 27.3). No patient achieved remission at 12 months. Glucocorticoids decreased from a baseline median of 20.0 mg/day (IQR 15.0–30.0) to 5.0 mg/day (IQR 0–10.0) at 12 months.
Conclusion Improved disease control and reduced glucocorticoid use was achieved for a proportion of patients following up to 12 months of belimumab treatment in a US real-world setting.
- autoimmune diseases
- biological products
- lupus erythematosus, systemic
Data availability statement
No additional data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In patients with SLE, a state of prolonged low disease activity is associated with lower organ damage accrual and prevention of flares.
Despite being a key treatment goal in the treat-to-target approach in SLE management, remission or low disease activity is challenging to achieve in real-world settings.
Belimumab, approved for active, autoantibody-positive SLE, has been found to consistently reduce disease activity and severe flares across multiple clinical trials; although post hoc analyses of pivotal phase III trials have evaluated attainment of low disease activity and remission in patients following belimumab treatment, its role in achieving disease control or remission in the real world is less well established.
WHAT THIS STUDY ADDS
This post hoc analysis of real-world data from patients with SLE in the US evaluation Of use of Belimumab in clinical practice SEttings (OBSErve) study demonstrated that disease control and a reduction in glucocorticoid use were achieved for a proportion of patients following up to 12 months of belimumab.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Belimumab may help patients with SLE achieve a sustained state of disease control with a reduction in glucocorticoids and potentially lower their risk of organ damage progression.
Introduction
SLE is a chronic autoimmune disorder characterised by a range of clinical manifestations and, in most patients, a relapsing–remitting disease course.1 Management of SLE focuses on achieving disease control, including remission or low disease activity, and prevention of organ damage and new flares.2 These goals are also a part of the treat-to-target recommendations in SLE.3 4 However, traditional medications for SLE, including antimalarials, immunosuppressants and glucocorticoids, may be insufficient to manage symptoms; up to two-thirds of conventionally treated patients experience ongoing disease activity,5 6 and few patients achieve disease control or prolonged remission.7 8 Therefore, a large unmet medical need remains for additional effective treatment(s) to control disease activity while meaningfully reducing disease-related morbidity and mortality, and limiting toxicity associated with traditional SLE treatment regimens such as glucocorticoids and immunosuppressants.
Belimumab is a disease-modifying treatment in SLE that specifically targets the underlying disease by binding to soluble B-lymphocyte stimulator, thereby inhibiting prolonged survival and differentiation of B cells.9 10 Belimumab is approved as add-on therapy for the treatment of patients ≥5 years of age with active, autoantibody-positive SLE, as well as for the treatment of adults with active lupus nephritis.11 In clinical trials and post hoc analyses, patients with SLE treated with belimumab plus standard therapy showed an improvement in clinical disease activity (SLE Responder Index 4) and reduction in the number of new severe SLE flares, glucocorticoid use and accumulation of long-term organ damage, versus those receiving standard therapies alone.12–17
Post hoc analyses of the pivotal BLISS-52 and BLISS-76 phase III trials have evaluated attainment of low disease activity and remission in patients with SLE following belimumab treatment.18 19 To add to these findings, we undertook a similar evaluation of real-world data from the US evaluation Of use of Belimumab in clinical practice SEttings (OBSErve) study, an observational study that followed up adult patients with SLE receiving intravenous belimumab 10 mg/kg, as part of standard clinical practice in the USA. The US OBSErve study found that patients treated with belimumab for up to 2 years demonstrated clinical improvements and reductions in glucocorticoid use and healthcare resource utilisation.20
The present analysis used data from the US OBSErve study to quantify the proportion of patients in a state of SLE disease control (primary objective) or SLE disease remission (secondary objective) at 12 months post belimumab initiation. Additional secondary objectives were to (1) evaluate the extent of disease control and remission by baseline immunosuppressant use and glucocorticoid dose, (2) quantify the proportion of patients achieving disease control and remission among those receiving belimumab at baseline and 6 and 12 months while receiving no or low glucocorticoid doses (≤5 mg/day prednisone equivalent) at 6 and 12 months of follow-up and (3) characterise SLE treatment patterns among patients at baseline and in the year following belimumab initiation.
Methods
Study design and data collection
This was a post hoc analysis (GSK Study 213502)21 of data from US OBSErve (GSK Study 117295), a 24-month observational cohort study conducted between 17 February 2012 and 6 May 2014 that assessed clinical outcomes and overall patterns of SLE care in patients receiving belimumab in real-world settings. Full details of US OBSErve have been published.20 In brief, 92 participating rheumatologists with ≥5 years of clinical practice experience who treated ≥10 patients with SLE annually were recruited to identify eligible patients with SLE and to collect data from the date of belimumab initiation (baseline) to up to 24 months of follow-up via medical chart review. Patient data were abstracted into case report forms (CRFs) at 6-month intervals. Within the CRFs, physicians recorded details of patient demographics, SLE-related medication use and disease activity (eg, as measured in clinical practice using Safety of Estrogens in Lupus Erythematosus National Assessment–SLE Disease Activity Index [SELENA-SLEDAI] scores). In the current analysis, data for up to 12 months of belimumab treatment were analysed.
Patient eligibility criteria
The US OBSErve study population comprised 501 patients who met the following inclusion criteria: had a documented SLE diagnosis, were ≥18 years of age at study entry, and initiated and continued belimumab (10 mg/kg intravenous) plus standard therapy for at least eight infusions at the time of study enrolment. Patients were excluded if they were currently enrolled in any SLE-related clinical trials or if they did not have at least 6 months of medical history prior to belimumab initiation documented with the participating rheumatologist. Patients were not required to have a baseline SELENA-SLEDAI score to participate in the US OBSErve study.
However, for the present analysis, only patients with a baseline SELENA-SLEDAI score of ≥6 and a follow-up SELENA-SLEDAI score measurement at 12 months were included, as this was necessary to characterise disease activity at baseline and 12 months.
Outcome definitions: SLE disease control and remission
Data collected in the CRFs including total SELENA-SLEDAI score and SLE medication use were used to define SLE disease control and complete remission at 12 months.
SLE disease control was defined using sequentially restrictive definitions: SELENA-SLEDAI score of ≤2 at 12 months, SELENA-SLEDAI score of ≤2 and glucocorticoid dose (prednisone equivalent) of ≤5 mg/day at 12 months and SELENA-SLEDAI score of ≤2 and glucocorticoid dose (prednisone equivalent) of ≤5 mg/day at 6 and 12 months. In subsequent sensitivity analyses, the initial outcome definitions were modified to take immunosuppressant use at 12 months into consideration, as detailed in online supplemental table S1. In addition, SLE disease remission was defined using sequentially restrictive definitions: SELENA-SLEDAI score=0 at 12 months; SELENA-SLEDAI score=0 and glucocorticoid dose (prednisone equivalent) of ≤5 mg/day at 12 months; and SELENA-SLEDAI score=0 and glucocorticoid dose (prednisone equivalent) of ≤5 mg/day at 6 and 12 months (online supplemental table S1).
Supplemental material
While the aforementioned definitions follow those used in the BLISS-BELIEVE study,22 some differences were introduced (eg, the allowance for low-dose glucocorticoids in all definitions and exploration of no immunosuppressant use in sensitivity analyses but not the main definitions) to more closely align with the management of SLE in the real world.
SLE medication use
SLE medication use (receipt of belimumab, immunosuppressants and/or oral glucocorticoids) was characterised from the CRF form data at baseline and 6 and 12 months. Belimumab and immunosuppressant use were characterised as any versus no use. Glucocorticoid use was characterised as any versus no use, receiving a prednisone-equivalent dose of ≤5 mg/day vs >5 mg/day, and prednisone-equivalent dose as a continuous variable summarised using mean and SD and median and IQR. During follow-up, the percentage of patients receiving immunosuppressants at 6 and 12 months (both at 6 and 12 months, only at 6 months or only at 12 months, or no use at 6 and 12 months) and/or low oral glucocorticoid doses (≤5 mg/day prednisone equivalent at 6 months and 12 months vs >5 mg/day at 6 and/or 12 months) were also reported.
Statistical analyses
Descriptive statistics were used to evaluate baseline patient characteristics and SLE medication use at baseline and 6 and 12 months. The proportion of patients achieving SLE disease control/remission was estimated with 95% CI for the following populations with a SELENA-SLEDAI score at baseline and 12 months: all patients; patients stratified by baseline immunosuppressant use; only patients stratified by baseline glucocorticoid dose (≤5 mg/day vs >5 mg/day prednisone equivalent); only patients who used belimumab at baseline, 6 months and 12 months, and who also received ≤5 mg/day (prednisone equivalent) dose of glucocorticoid at 6 and 12 months. Patients were not required to receive belimumab at 12 months; however, a sensitivity analysis for the primary objective was restricted to those patients who were receiving belimumab at baseline and at both 6 and 12 months.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of this analysis.
Results
Study population and patient characteristics
Of the 501 patients originally enrolled by rheumatologists (N=92) in the US OBSErve study,20 122 (24%) had baseline SELENA-SLEDAI scores available, of whom 117 had a baseline SELENA-SLEDAI score of ≥6. Of these 117 patients, 27 did not have a 12-month SELENA-SLEDAI score available. In total, 90 patients were eligible to be included in this analysis (figure 1).

Patient disposition. OBSErve, Evaluation Of use of Belimumab in clinical practice SEttings; SELENA-SLEDAI, Safety of Estrogens in Lupus Erythematosus National Assessment–SLE Disease Activity Index.
Baseline demographics and disease characteristics for the analysis population are shown in table 1. Patients had a mean (SD) age of 40.8 (11.4) years, and the majority (84.4%) were female and of Caucasian ethnicity (61.1%). Most patients had moderate SLE, diagnosed during the last 1 to 5 years, for which they were receiving predominantly oral glucocorticoids (87.8%; mean (SD) prednisone-equivalent dose: 24.8 [15.5] mg/day) and/or antimalarials (80.0%), and/or immunosuppressants (47.8%).
Patient demographics and baseline characteristics
SLE disease control at 12 months post belimumab initiation
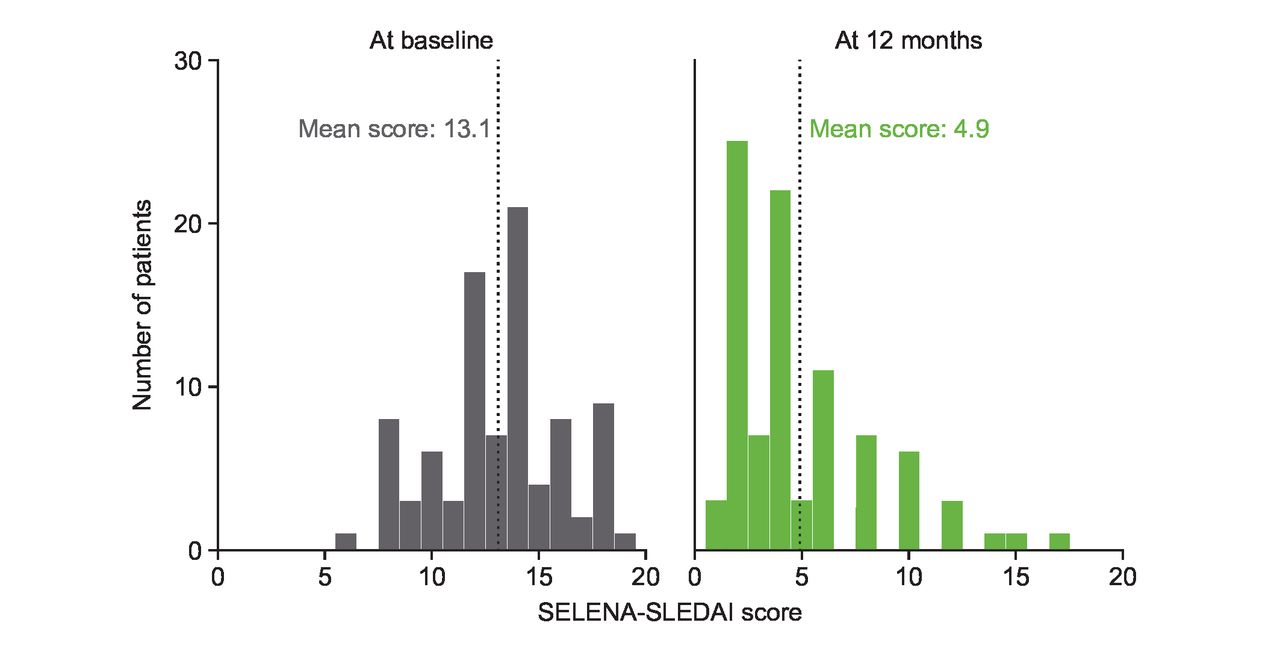
Patients had a mean (SD) SELENA-SLEDAI score of 13.1 (3.0) at baseline and 4.9 (3.4) at 12 months (figure 2). The proportion of patients achieving disease control decreased as more stringent definitions of disease control were applied: 31.1% of patients had a SELENA-SLEDAI score ≤2 at 12 months (95% CI 21.8 to 41.7), 25.6% had a SELENA-SLEDAI score of ≤2 and received a glucocorticoid dose of ≤5 mg/day prednisone equivalents at 12 months (95% CI 16.9 to 35.8); 17.8% had a SELENA-SLEDAI score of ≤2 and received a glucocorticoid dose of ≤5 mg/day prednisone equivalents at 6 and 12 months (95% CI 10.5 to 27.3) (figure 3A).
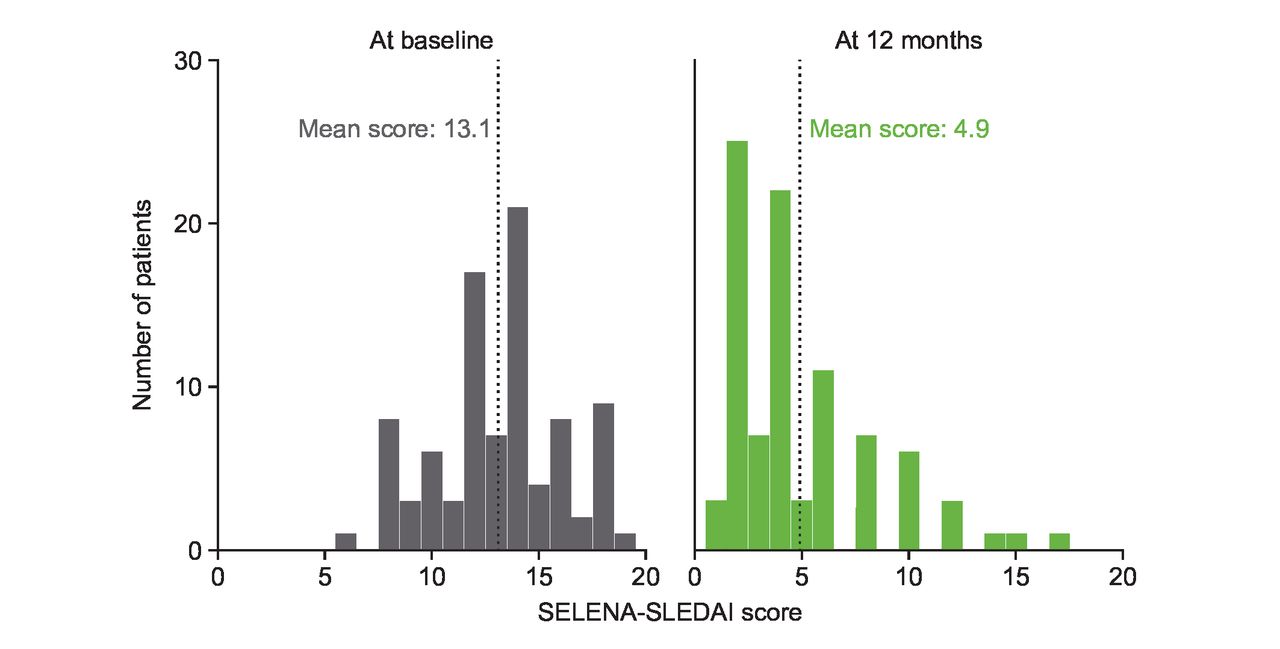
Distribution of SELENA-SLEDAI scores at baseline and 12 months following belimumab treatment (N=90). Median at baseline: 13.5; median at 12 months: 4.0. SELENA-SLEDAI, Safety of Estrogens in Lupus Erythematosus National Assessment–SLE Disease Activity Index.

Proportions of patients with SLE achieving disease control or remission at 12 months following belimumab treatment, according to definitions of increasing stringency for (A) all eligible patients (N=90); (B) stratified by baseline glucocorticoid dose (prednisone equivalent) (≤5 mg/day [n=11] vs >5 mg/day [n=79]); (C) stratified by baseline immunosuppressant use (use [n=43] vs no use [n=47]). SELENA-SLEDAI, Safety of Estrogens in Lupus Erythematosus National Assessment–SLE Disease Activity Index.
The proportion of patients achieving disease control was numerically higher among those on lower glucocorticoid doses (≤5 mg/day prednisone equivalent) at baseline (n=11) versus patients receiving higher glucocorticoid doses (n=79) (figure 3B), while no substantial difference was observed in the proportion of patients achieving disease control when stratified by baseline immunosuppressant use (figure 3C).
Among patients receiving belimumab at baseline and 6 and 12 months, and who received a glucocorticoid dose (prednisone equivalent) of ≤5 mg/day at 6 and 12 months (n=39), 38.5% (95% CI 23.4 to 55.4) achieved disease control across all definitions considered; the percentage was the same across definitions in this subgroup because all patients were required to have a glucocorticoid dose (prednisone equivalent) of ≤5 mg/day at 6 and 12 months.
The sensitivity analysis of the initial disease control definitions that was restricted to patients who received belimumab at baseline and 6 and 12 months was consistent with the primary analysis (online supplemental figure S1). Full details of subsequent sensitivity analyses are shown in the online supplemental material (supplemental results). Results of the sensitivity analysis were generally consistent with those of the primary analysis.
SLE disease remission at 12 months post belimumab initiation
None of the 90 eligible patients achieved disease remission, defined as a SELENA-SLEDAI score=0 at 12 months.
SLE medication use following belimumab treatment initiation
Of the 90 patients who received belimumab at baseline and 6 months, 92.2% received belimumab at 12 months.
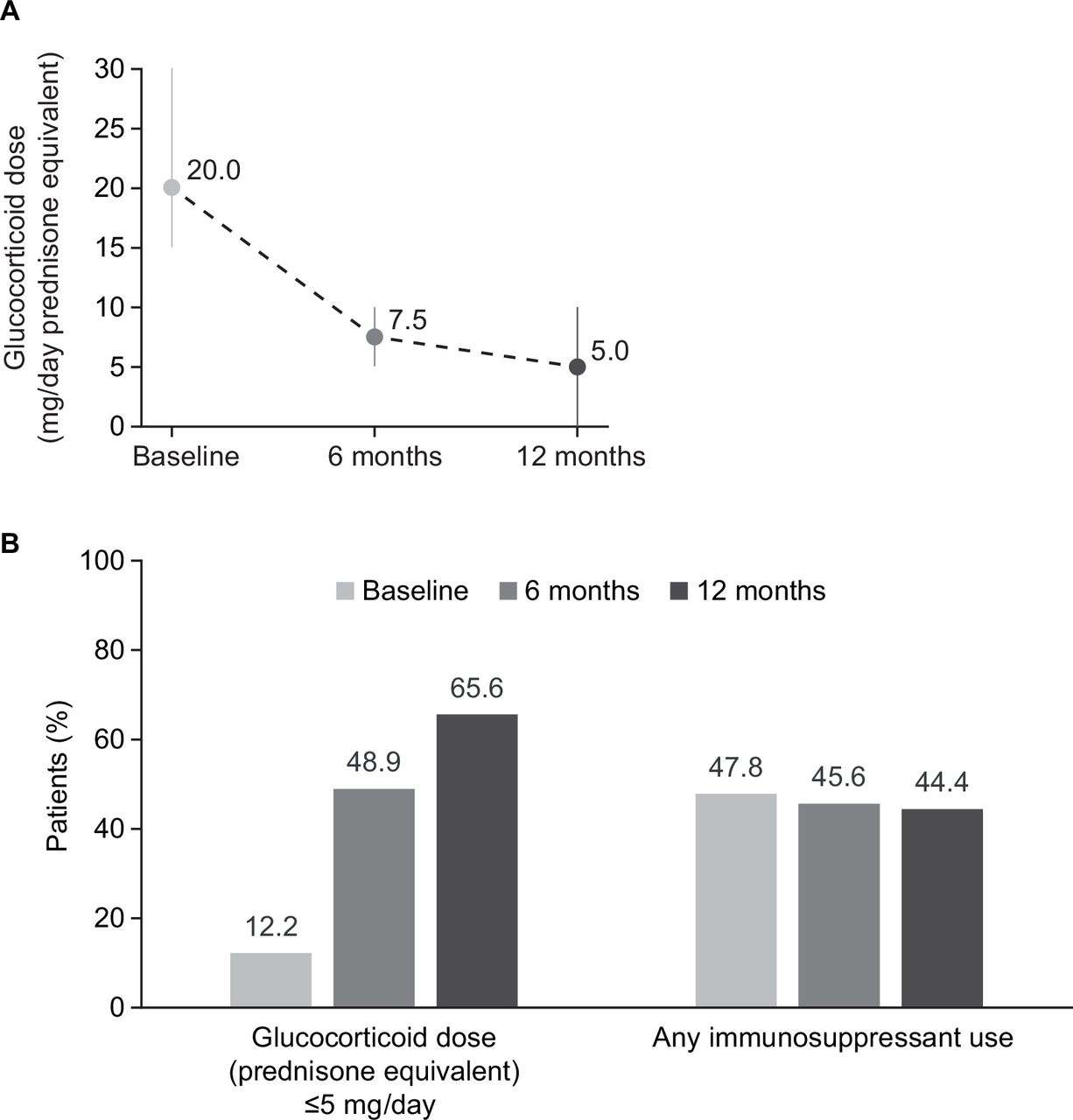
Glucocorticoid use decreased from a median (prednisone equivalent) dose of 20 (IQR 15–30) mg/day at baseline to 5 (0–10) mg/day at 12 months following belimumab initiation (figure 4A). The proportion of patients receiving doses of ≤5 mg/day increased from 12.2% at baseline to 65.6% at 12 months (figure 4B). During the same time period, the proportion of patients receiving immunosuppressants following treatment with belimumab remained largely unchanged at 47.8% of patients at baseline and 44.4% at 12 months (figure 4B). When quantifying SLE treatment patterns during follow-up (N=90), 38.9% of patients received immunosuppressants at both 6 and 12 months, 12.2% of patients received immunosuppressants at only 6 months or only 12 months, and 48.9% of patients received no immunosuppressants throughout this period. Slightly less than half (45.6%) of the patients received prednisone-equivalent glucocorticoid doses of ≤5 mg/day at 6 and 12 months. Lastly, 15 out of the 90 patients (16.7%) received no immunosuppressants and ≤5 mg/day prednisone equivalent glucocorticoid dose at both 6 and 12 months.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
SLE medication use following belimumab treatment: (A) median (IQR) glucocorticoid dose (prednisone equivalent) mg/day; (B) glucocorticoid and immunosuppressant use (N=90).
Discussion
Among adults with SLE who initiated and continued belimumab for ≥6 months in US real-world settings, nearly one in three (31.1%) achieved disease control when it was defined as a SELENA-SLEDAI score of ≤2 at 12 months. Approximately one in six patients (17.8%) achieved disease control when it was defined to also require glucocorticoid doses of ≤5 mg/day at 6 and 12 months. These findings are encouraging, given the high baseline level of disease activity in patients in US OBSErve (mean SELENA-SLEDAI score 13.1), especially when considered in tandem with the decrease in median prednisone-equivalent glucocorticoid dose (from 20.0 mg/day at baseline to 5.0 mg/day at 12 months).
Despite differences in study design and endpoint definitions, the results from this post hoc analysis of US OBSErve data are consistent with prior studies quantifying the benefit of belimumab in helping patients achieve low disease activity states at 52 weeks (online supplemental table S6).18 23–25 Two post hoc analyses of the BLISS-52 and BLISS-76 trials found intravenous belimumab (at 1 mg/kg or 10 mg/kg) plus standard therapy to be efficacious in helping patients with SLE achieve lupus low disease activity state (LLDAS) at 52 weeks compared with placebo plus standard therapy.18 23 26 In terms of real-world observational studies, Gatto et al reported that 71.7% of 466 patients with SLE treated with belimumab achieved low disease activity at 12 months24; similarly, Sbeih et al found that 58.1% of 50 patients with SLE treated with belimumab achieved stable LLDAS by 12 months.25 Such high proportions of patients achieving LLDAS may be driven by the lower levels of baseline SLE disease activity versus other studies, differences in low disease activity definitions and data collection.25 27 Nevertheless, the fact that 17.8% of patients in the current study achieved disease control with reductions in glucocorticoid use is encouraging and provides additional evidence beyond prior clinical and real-world studies that belimumab is effective for helping patients achieve low disease activity states in real-world settings.
In the current study’s stratified analyses, there was higher attainment of disease control at 12 months among the 11 patients receiving glucocorticoid doses ≤5 mg/day at baseline versus the 79 patients receiving higher doses (figure 3B). A post hoc study of BLISS-52 and BLISS-76 trials also found that lower doses of glucocorticoids were associated with low disease activity with belimumab,18 whereas another post hoc analysis of pooled BLISS-52 and BLISS-76 data showed no association of baseline glucocorticoid dose with achieving low disease activity following belimumab (online supplemental tables S6 and S7).19 When stratified by immunosuppressant use (figure 3C), the extent of disease control attained at 12 months in our analysis appeared to be similar between the patients receiving immunosuppressants at baseline (n=43) versus those who did not (n=47). However, such comparisons should be interpreted with caution due to small sample sizes, the descriptive nature of the results, and potential differences in disease severity and other factors between patients receiving different treatments at baseline.
No patient in the US OBSErve study achieved complete remission (SELENA-SLEDAI score=0) at 12 months.4 In prior studies of belimumab that implemented less stringent definitions of remission, proportions of patients achieving remission at 52 weeks following belimumab initiation ranged from ~10% to 41% (online supplemental table S7)24 25 28; however, the extent of remission varied extensively by study design, including how the remission outcome was operationalised. In the US OBSErve study, the lack of any patient achieving remission was likely influenced by the short time frame in which patients with high disease activity at baseline had to achieve complete remission. In a real-world study of the Johns Hopkins cohort, the median time to complete remission on treatment among patients with SELENA-SLEDAI score of >0 at baseline was 3.1 years, supporting the insufficient duration of the US OBSErve study period to observe complete remission.7
In the present analysis, median prednisone-equivalent glucocorticoid dose decreased from 20 mg/day at baseline to 5 mg/day at 12 months. Long-term or high-dose glucocorticoid use is associated with organ damage, adverse events and increased mortality risk in patients with SLE.29 The ≤5 mg/day of prednisone-equivalent cut-off is considered an appropriate limit for minimising the adverse effects of long-term glucocorticoid maintenance therapy while retaining effectiveness,29 and 65.6% of patients in the current analysis were able to achieve this at 12 months after belimumab initiation, compared with 12.2% of patients at baseline. This is consistent with the results of prior clinical and observational studies, which showed reductions in glucocorticoid dose following belimumab initiation,13 14 29–32 and suggests that belimumab treatment enables reductions in the use of glucocorticoids while maintaining an acceptable level of disease control.
According to 2019 European Alliance of Associations for Rheumatology (EULAR) recommendations and the treat-to-target principle, the goals of SLE management should be remission or low disease activity and prevention of flares, with the lowest possible dose of glucocorticoids.2 3 However, as observed in this study, complete remission as defined in the EULAR guidelines occurs infrequently in practice,2 8 33 34 whereas, as we also observed in this study, disease control and low disease activity are more feasible to achieve. Low disease activity, similar to disease remission, is associated with reduced organ damage rates and improvements in health-related quality of life, as well as having significant protective associations with SLE flares.24 35–40 These findings underscore the importance of promptly achieving and sustaining disease control in patients with SLE.
The results of this study should be interpreted with caution, given several limitations of the US OBSErve cohort. First, this study was single-arm, open-label and did not include a comparator group. Second, the patients included were required to be recruited by participating rheumatologists and had to initiate and continue belimumab for ≥6 months; thus, included patients may not be representative of other clinical and real-world populations. Third, data for this real-world study were only collected if they were routinely used and recorded by participating physicians. The original study did not mandate capture of SELENA-SLEDAI scores, and data availability was dependent on individual physician clinical practices. As such, SELENA-SLEDAI scores were only available at baseline and 12 months for a subset of the overall cohort, limiting the sample size for this analysis. However, the limited use of the SELENA-SLEDAI in US OBSErve is consistent with what has been documented in other real-world settings.41 Moreover, individual components of SELENA-SLEDAI were not collected, and thus, the types of clinical and serological manifestations may have differed between included patients. Fourth, data were only collected at 6-month intervals and may not adequately capture SLE medication use and patient characteristics at the granularity of other study designs and methods of data collection. Finally, these data were collected during 2012 and 2014 and may not fully reflect current clinical practice, given the increased recognition of the importance of remission and low disease activity alongside reduction in cumulative glucocorticoid exposure as goals of treatment.4
Conclusion
The extent of disease control following treatment with belimumab documented in this real-world study in the USA is consistent with previous analyses showing that patients with SLE initiating belimumab can achieve low disease activity states with reduced glucocorticoid use. Overall, these findings support belimumab in the treatment of adults with SLE and can help achieve treatment goals that are aligned with the recommended treat-to-target approach.
Data availability statement
No additional data are available.
Ethics statements
Patient consent for publication
Ethics approval
When initially conducted, the US evaluation Of use of Belimumab in clinical practice SEttings (OBSErve) study was granted blanket study approval covering all study physicians from the New England Institutional Review Board (NEIRB). With the deidentification of patient data, a waiver of informed consent for study patients was granted by the NEIRB. There were no treatment interventions or safety concerns with patients. Case report forms were provided to the participating physicians for each patient’s data to be recorded. For this post hoc analysis using US OBSErve data, no new data were collected, and no physicians or patients were contacted.
Acknowledgments
We thank Christopher F Bell for supporting discussions of this study. Medical writing support was provided by Casmira Brazaitis, PhD, of Fishawack Indicia Ltd, UK, part of Fishawack Health, and was funded by GSK.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JNH, JF-B and DC were responsible for the study design. JF-B acquired and had access to the data. All authors (JNH, JF-B, MEG, AR, YIG, HQ and DC) analysed and interpreted the results and critically reviewed and approved the final manuscript for submission. All authors accept full responsibility for the finished work. JNH is the guarantor for this publication.
Funding This study was funded by GSK (GSK Study 213502).
Competing interests JNH, JF-B, MEG, AR, YIG, HQ and DC are employees of GSK and hold stocks and shares in the company.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.