Article Text

Abstract
Objective Infections are a common complication of SLE. Our objective was to evaluate their causes and impact on the survival of patients with SLE.
Methods Analysis of the admissions and death causes in patients diagnosed with SLE from the Spanish Hospital Discharge Database and the infection-related deaths of the Spanish population from the National Statistical Institute, between 2016 and 2018.
Only infections recorded as the main diagnosis were analysed (severe or clinically relevant infection).
Results Among 18 430 admissions in patients with SLE, disease activity was the cause of admission in 19% of all patients and infection in 15%. However, infection was the main cause of death (25%) while SLE activity was responsible for only 6% of deaths (p<0.001). Severe infection exceeded SLE as a cause of death for patients dying at ages between 40–59 (23% vs 4%, p<0.001), 60–79 (26% vs 6%, p<0.001) and older than 80 years (25% vs 6%, p<0.001). Infection was the cause of death in 8% of the Spanish population, a significantly lower rate when compared with patients with SLE (p<0.001). Compared with the general population, infections were the highest relative cause of death in patients with SLE, particularly at younger ages: 40% vs 3% for those below 20 years old (p<0.01), 33% vs 4% between 20 and 39 (p<0.001), 23% vs 5% between 40 and 59 (p<0.001), 26% vs 5% between 60 and 79 (p<0.001) and 25% vs 9% for those older than 80 years (p<0.001).
Conclusion Our nationwide study confirms that infections are the leading cause of death in SLE in Spain, with the highest proportion occurring in young patients with lupus compared with the general population of the same age range.
- systemic lupus erythematosus
- glucocorticoids
- epidemiology
Data availability statement
Data are available on reasonable request. NA.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Infections are one of the key determinants of early morbidity and mortality of patients with SLE, strongly linked to disease activity and immunosuppression.
WHAT THIS STUDY ADDS
Infections accounted for 25% of deaths in patients with SLE, in comparison with 8% in the general Spanish population.
These differences were more noticeable among younger patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Since infection is the main factor accounting for the high age-standardised mortality rate identified in patients with lupus, measures mitigating its impact on this population should be reinforced, such as a rational use of immunosuppression and glucocorticoids, vaccination and prompt identification and treatment of infection.
Introduction
SLE is a complex and heterogenic autoimmune disease that mainly affects women at a young age.1 2 Thanks to the recent advances and better management of the disease, the prognosis of patients with SLE has dramatically improved in recent decades.3 However, mortality is still twofold to fivefold higher in patients with SLE than in the age-matched and sex-matched population, confirming that there is still a lot of room for improvement.4–7 Infections are one of the key determinants of early morbidity and mortality of patients with SLE, strongly linked to disease activity and immunosuppression, particularly glucocorticoid (GC) use.4 8–11 The present study aims to analyse the characteristics and impact of infections leading to hospital admission or death in patients with SLE, as well as to compare the characteristics and deaths attributable to infection with the general Spanish population.
Materials and methods
We performed an analysis of data extracted from the Spanish Hospital Discharge Database (SNHDD) and the National Statistical Institute (NSI) databases, public access registries belonging to the Spanish Government.
Patients with SLE
Hospital-admitted patients with SLE were identified in the data extracted from the SNHDD. The SNHDD includes demographic and epidemiological data and up to 20 diagnoses carried out during admissions. These diagnoses were retrieved according to the discharge reports, and in case of decease, also according to the death certificate. Both documents are recorded by the attending physician in charge and must contain the same information, for legal and epidemiological purposes. Diseases and conditions were defined considering the International Classification of Diseases-Tenth Revision, Clinical Modification (ICD-10-CM), which is the one used by the Spanish SNHDD. We selected hospital admissions for patients with a diagnosis within the ICD-10-CM code M32 (SLE) from 2016 to 2018, at any position in the diagnostic list. Patients who presented drug-related SLE (ICD-10 code M32.0) were excluded.
According to the database structure and design, the main diagnosis was the defining reason for admission, or the cause of death if so. Therefore, all main diagnoses were decodified, analysed and clustered, but only those admissions and deaths attributable to SLE and infection were analysed. Hence, patients were considered to present active lupus if SLE was the main diagnosis during admission. On the other hand, only severe or clinically relevant infections, leading to hospital admission and/or death, were considered in the analysis. Admissions and deaths related to infectious diseases were identified and re-classified according to the specific foci, considering the different ICD-10-CM codes.
Spanish population
The NSI database provides demographic and epidemiological information about the overall Spanish population, including life expectancy and mortality rates. The number and causes of death are also recorded according to death certificates, coded by the ICD-10-CM. We retrieved the causes of death of the overall Spanish population from 2016 to 2018. Following the same criteria as in the SNHDD, deaths related to infection were classified according to the foci.
Statistical analysis
Categorical variables were reported as frequencies and percentages while continuous variables were presented as mean and SD. The significance of differences between the two groups was determined by χ2 test, Fisher’s exact test or Student’s t-test, as appropriate. First, we analysed the prevalence, characteristics, foci and mortality of infections in hospital-admitted patients with SLE. Second, we compared the characteristics of the patients who were admitted because of infections and those who were admitted because of SLE activity. Besides, we compared the proportion of deaths attributable to infection and SLE activity for each age group in this same cohort (younger than 20, 20–39, 40–59, 60–79 and older than 80 years old). Third, we compared the infection-related death rates as well as their foci between patients with SLE in the SNHDD and the general Spanish population in the NIE registry. We also studied the proportion of deaths attributable to infections for each age group. For all the analyses, a significance level of 0.05 was set. Statistical analysis was performed using SPSS V.26.0 (IBM, Spain).
Results
Characteristics of patients with SLE
Between 2016 and 2018, 18 430 hospital admissions in patients with SLE were identified in the Spanish national registry. Table 1 shows the population characteristics. Overall, 83% were female with a mean age of 53.2 years. Ninety-two per cent of patients were tagged as Caucasian, 5% as Hispanic, 2% as Arabic and <1% as Asian, Black African or Asian, respectively. Regarding outcomes, 1033 patients (6%) were admitted to the intensive care unit (ICU) and 584 (3%) died. The mean length of admission was 8.6 days.
Patient’s characteristics
Infection-related admissions
During the study period, 2755 patients (15%) were admitted because of infection, which caused 25% of all deaths (147 patients). The mortality rate for admissions related to infection was 5%. The most frequent site/type of infection was identified as follows (table 2): respiratory (37%), genitourinary (17%), sepsis (10%), viral infections (9%), non-biliary abdominal (7%), skin and soft tissue (5%), biliary tract (5%), otorhinolaryngological (2%) and gynaecological (2%). Being the cause of 1 in 10 admissions, sepsis accounted for 41% of infection-related deaths and 10% of all deaths. Consequently, sepsis presented the highest mortality rate (22%). Respiratory tract infections accounted for 27% of deaths among infection-related admissions and 7% of all deaths, thus resulting in a 4% mortality rate.
Infection foci in patients with SLE
Differences among admissions related to infection and SLE activity
Overall, SLE activity was the main cause of admission (19% of all admissions), being responsible for just 6% of all deaths (36 patients). When compared with SLE-related admissions (table 3), patients admitted because of infection were older (57.9 vs 41.2 years old, p<0.001) and presented a higher mortality rate (5% vs 1%, p<0.001), a higher ICU admission rate (7% vs 3%, p<0.001) and a longer length of stay (9.6 vs 8.5 days, p<0.001).
Differences among admissions related to infection and SLE activity
The mean age of the deceased patients because of SLE and infection was similar (67.7 vs 62 years, respectively, p=0.144). The proportion of deaths attributable to each cause was re-analysed according to age ranges (figure 1). Infection exceeded SLE as a cause of death among deceased patients 40–59 years old (23% vs 4%, p<0.001), 60–79 years old (26% vs 6%, p<0.001) and older than 80 years (25% vs 6%, p<0.001). Although infections doubled SLE as a cause of death in patients younger than 20 years (40% vs 20%), the difference did not reach statistical significance (p=0.490). The proportions of death due to each cause were similar among patients aged 20–39 years (33% vs 33%, p=0.900).

Deaths attributable to infection versus SLE activity, among hospital-admitted patients with SLE, for each age period. Data are expressed as a percentage of death for all causes among patients with SLE, for each age period. *Differences statistically significant (χ2 test).
Deaths due to infection in patients with SLE compared with the Spanish general population
According to the NSI, the Spanish population was 46 449 874 in 2016, 46 532 869 in 2017 and 46 728 814 in 2018. Within these 3 years, when the population life expectancy was 80.6 years for men and 86.3 years for women, 1 262 855 deaths were declared. Infection was the cause of death in 95 442 of them, a significantly lower rate when compared with patients with SLE (8% vs 25%, p<0.001). These differences were explained by the higher proportion of patients with SLE dying because of respiratory tract infections (7% vs 4%, p<0.001), sepsis (10% vs 1%, p<0.001) and viral infections (2% vs 0.6%, p<0.002) (table 4).
Differences between the infection foci in deceased patients with SLE and the Spanish population
Deaths due to infection by age ranges in patients with SLE and the general Spanish population
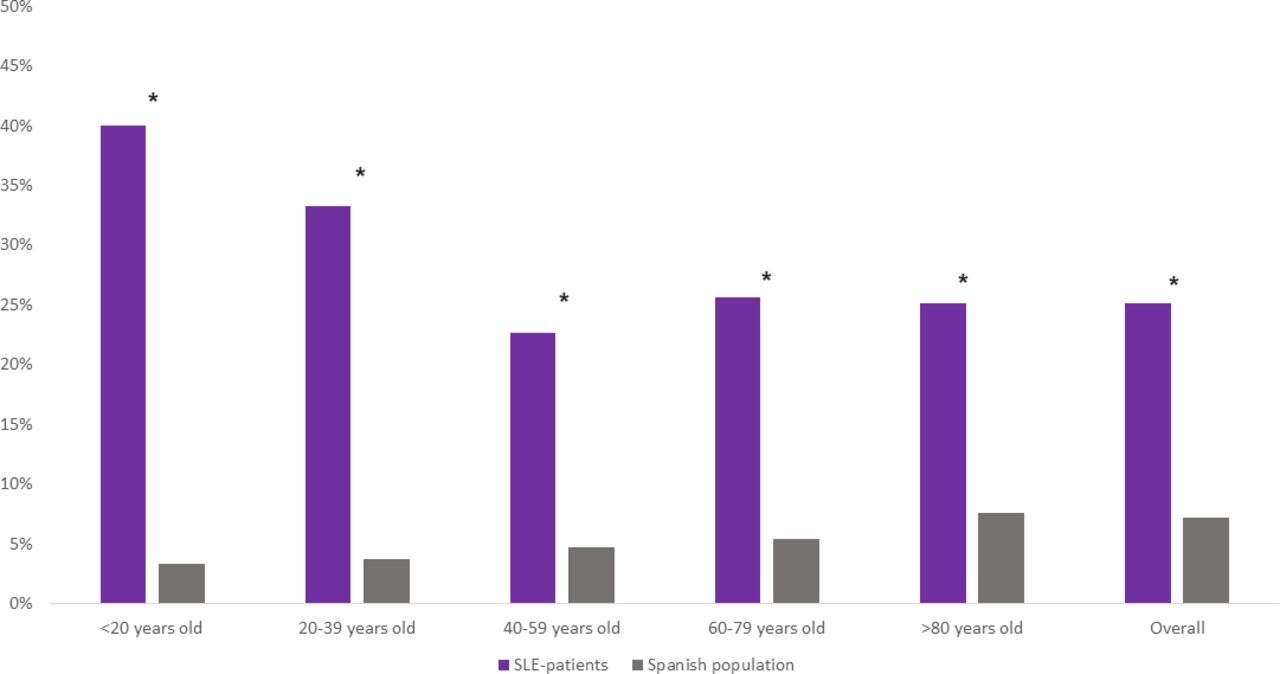
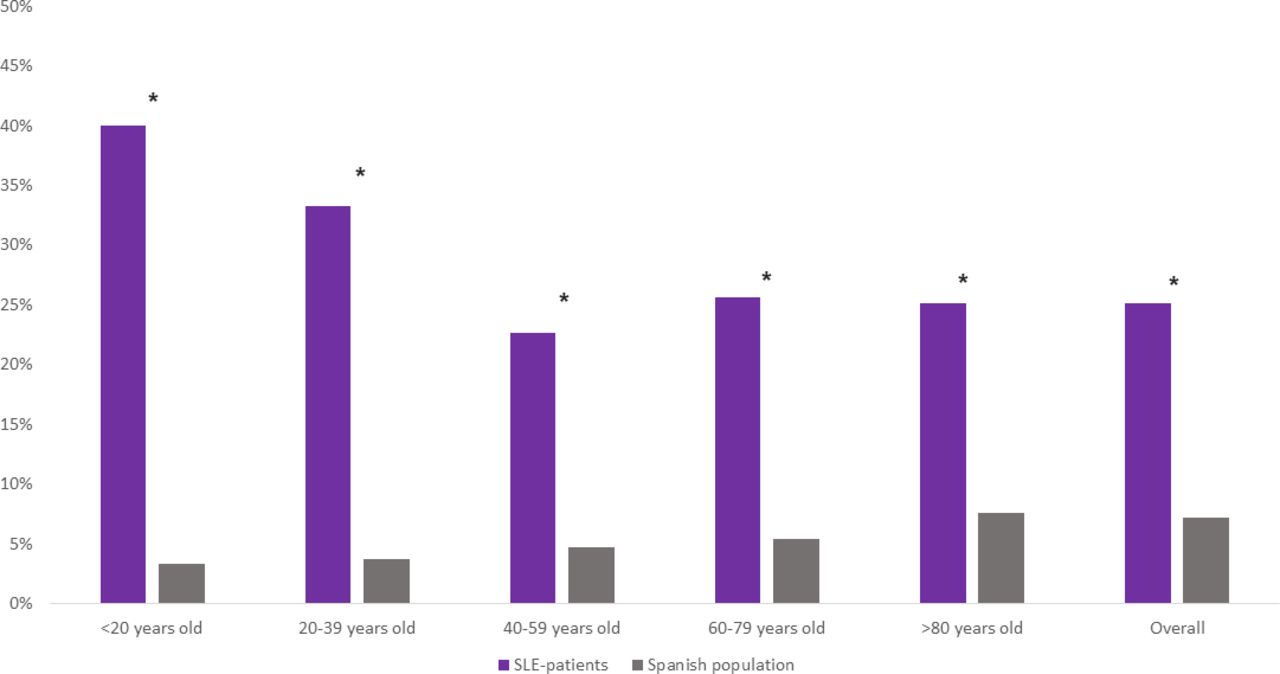
We further compared the proportion of infection-related deaths for each age range (figure 2). Compared with the general Spanish population, deaths due to infection were more frequent in SLE patients across all age groups, with the largest differences seen among younger patients: 40% vs 3% for those below 20 years old (p<0.01); 33% vs 4% between 20 and 39 years old (p<0.001); 23% vs 5% between 40 and 59 years old (p<0.001); 26% vs 5% between 60 and 79 years old (p<0.001); and 25% vs 9% for those older than 80 years old (p<0.001).
{kind=link}
{kind=link}
Infection-related deaths, among patients with SLE and the Spanish population, for each age period. Data are expressed as a percentage of death for all causes among patients with SLE and the overall Spanish population, for each age period. *Differences statistically significant (χ2 test).
Discussion
This large nationwide epidemiological study supports that infection is one of the leading causes of death in hospital-admitted patients with SLE, particularly in younger patients. We believe that these results provide a clear-cut message for clinicians treating patients with SLE, reinforcing the idea of taking any measure needed to decrease infections.
In our study, one out of four deaths in patients with SLE were attributable to infection, in comparison with 8% in the general Spanish population. By contrast, lupus itself accounted for only 6% of deaths. Other groups have previously analysed the causes of death in patients with SLE worldwide with different results, sometimes limited by sample size and monocentric design.4 5 7 11–15 Our nationwide analysis indeed confirms that infection has surpassed lupus itself as the main cause of death in this population, according to the increasing number of deaths due to infection during the last decades reported by others.4 8 16–19 Moreover, the risk of infection is particularly worrisome at a younger age, as our data confirmed, although it is not limited to this group. Infection deaths in patients with lupus were 10-fold higher than in age-matched controls among those younger than 20 years old. Therefore, the high impact of infection in young patients, where the disease is more active, is probably related to immunosuppression during SLE flares. On the other hand, severe infection in patients older than 40 years old might be secondary to cumulative drug toxicity along with irreversible organ damage.4 8 9 11 20 Accordingly, our data confirm that infections had a tremendous impact on years of life lost in SLE. While the Spanish life expectacy was over 80 years in this period, the mean age of SLE patients who died because of infection was 57 years. Altogether, it seems that infections are one main factor accounting for the high age-standardised mortality rate identified in patients with SLE.4 6 21 22
In addition to the importance of opportunistic infections in the immunosuppressed patient such as respiratory tract, abdominal, skin and soft tissue or central nervous system foci, as well as those produced by parasitic, fungal or zoonosis microorganisms, our results highlighted sepsis as a disproportionate cause of death in patients with lupus. Similar findings have been described previously, and even Singh and Cleveland recently showed that sepsis overtook pneumonia as the most common infection leading to admission in patients with SLE in the USA.18 19 Again, the striking mortality rate described in our population is especially noteworthy compared with what would be expected among young patients.12 22
Immunosuppressive agents, particularly GCs, have shown to play a major role in susceptivity to infection in patients with SLE, particularly those with more active disease.1 2 9 22–25 In fact, Selvananda et al reported that infections were concurrent with SLE flares in 41% of admissions, reflecting that both situations tend to coincide.11 Unfortunately, we were not able to consider immunosuppression in our analysis, since no information regarding treatments could be retrieved from the database. However, we strongly believe that our findings point out the need for measures to mitigate the impact of infection in patients with lupus, such as generalised antimalarial treatment, use of methyl-prednisolone pulses allowing a faster control of activity and an easier prednisone tapering, the avoidance of maintenance doses of prednisone >5 mg/day and a judicious use of immunosuppressive drugs in severe flares and whenever prednisone cannot be tapered down.9 10 26–30 Finally, other general measures such as vaccination and the early identification and treatment of bacterial infections and sepsis are especially important in immunosuppressed patients and could decrease the associated mortality.9 31 32
Several limitations of this study have to be considered. First, important information regarding disease course (early vs late disease), prednisone doses and duration and the use of immunosuppressive drugs and antimalarials or microbiological isolations was not available and could have provided more solid conclusions. Second, this analysis was restricted to hospital admissions, with the resultant limitation in power and the potential selection bias. However, we mainly evaluated categorical variables such as admission due to SLE or infection and death, which are difficult to misclassify. Third, the prevalence of SLE could not be properly assessed in the databases, therefore, the rate of infections could not be calculated and only deaths could be compared. Besides, it has to be mentioned that the cause of admission and death was defined by the main diagnosis, recorded by the attending physician during the discharge report or death certificate. To this matter, and according to the database basis, SLE was considered active when lupus was the main cause of admission event though this was not specifically defined within the ICD-10 coding. On the other hand, we did not consider other secondary diagnoses to only analyse clinically relevant infections, presumably creating selection and inclusion bias. Consequently, the true prevalence of infection in SLE was not assessed and the different processes that might occur during the same admission were not determined. In addition, the origin of infection in the patients whose main diagnosis was sepsis could not be elucidated, possibly producing some variations in the distribution of the infectious foci. In sum, and despite the previous, we believe that our study offers a nationwide analysis with a large sample size and a long study period, with consistent results confirming the ones seen in smaller studies.
Conclusions
Our nationwide study confirms that infections are the leading cause of death in SLE in Spain, with the highest proportion occurring in young patients with lupus compared with the general population of the same age range. Since infection is the main factor accounting for the high age-standardised mortality rate identified in patients with lupus, measures mitigating its impact on this population should be reinforced, such as a rational use of immunosuppression and GCs, vaccination and prompt identification and treatment of infection.
Data availability statement
Data are available on reasonable request. NA.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the local research ethics committee (expedient number PI 80-21) and complied with the Declaration of Helsinki. Due to the design of the study, and according to Spanish law, informed consent was not required.
References
Footnotes
Contributors VM-T (guarantor) and GR-I: study concept and design, statistical analysis, interpretation of results, drafting of the manuscript, critical revision of the manuscript, approval of the final version of the manuscript. VM-T, MM-U, AG-R, ES and GR-I: study concept and design, interpretation of results, drafting of the manuscript, critical revision of the manuscript, approval of the final version of the manuscript. All other authors: data acquisition, critical revision of the manuscript, approved the final version of the manuscript.
Funding This work has been supported by a grant from Instituto de Salud Carlos III (Expedient number CM19/00223) and Sociedad Española de Medicina Interna (Premio Professor Dr Miguel Villardell).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.