Article Text

Abstract
Objective Lupus nephritis is a key driver of morbidity and mortality in SLE. Detecting active nephritis on a background of pre-existing renal damage is difficult, leading to potential undertreatment and accumulating injury. An unmet need is a biomarker that distinguishes active lupus nephritis, particularly important in paediatrics where minimising invasive procedures is desirable.
Methods This was a multicentre, prospective study of 113 paediatric patients with biopsy-proven lupus nephritis. Clinical data and urine were obtained every 3–4 months and patients averaged 2 years on study with seven time points. Urine was analysed for human epidermal growth factor receptor 2 (HER2), tumour necrosis factor-like weak inducer of apoptosis and vascular cell adhesion molecule-1 (VCAM-1) by ELISA. We defined active disease as either a rise in serum creatinine ≥0.3 mg/dL from baseline or a rise in renal Systemic Lupus Erythematosus Disease Activity Index score from the previous visit. These markers were also studied in patients with acute kidney injury, juvenile idiopathic arthritis (JIA), amplified pain syndrome and healthy controls.
Results The rate of active disease was 56% over an average of 2 years of follow-up. HER2 and VCAM-1 were significantly elevated at time points with active disease defined by increased serum creatinine compared with time points with inactive disease or patients who never flared. All three biomarkers were associated with new-onset proteinuria and VCAM-1 was elevated at time points preceding new-onset proteinuria. These biomarkers were not increased in acute kidney injury or JIA.
Conclusion All three biomarkers were associated with new onset proteinuria and increased VCAM-1 may predict impending proteinuria. These biomarkers provide potential non-invasive measures for monitoring that may be more sensitive to impending flare than conventional measures.
- lupus nephritis
- autoimmune diseases
- autoimmunity
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information. Primary data are avaialble upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Lupus nephritis is a quality-of-life-defining complication. It has been difficult to distinguish effects of pre-existing renal damage from acute flare of lupus nephritis on the basis of a typical urinalysis, and renal biopsy is currently the gold standard for diagnosis. Yet, repeated biopsies are invasive and a urine biomarker would be a valuable adjunct for treatment decisions.
WHAT THIS STUDY ADDS
This study identified biomarkers in urine that could be used in a point-of-service test to identify a flare of lupus nephritis or an impending flare of lupus nephritis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study requires validation on a larger cohort but these biomarkers show promise as early indicators of flare of lupus nephritis. A point-of-service urine test would allow early intervention to prevent accrual of renal damage.
Introduction
Pediatric-onset SLE usually confers a lifelong risk of end-organ damage, poor quality of life and disability. One of the more common organs affected is the kidney, where the cumulative effect of episodes of inflammation can lead to renal failure and the need for dialysis or transplant. The frequency of lupus nephritis (LN) in paediatric SLE ranges from 50% to 80%,1 2 and there have been limited improvements in LN outcomes over the years.3 Adult studies have found that 20% of patients with LN in the first year of diagnosis develop end-stage renal disease and that nearly half of patients with LN class IV will develop end-stage renal disease within 15 years.3 4 The presence of LN also confers an increased risk of mortality.5 While there are fewer outcome studies of paediatric SLE, a study of 111 adults with paediatric-onset SLE, with median disease duration of 20 years, showed that 60% had LN and 24% of those developed renal damage.6 7 In the latter group, 38% received a renal transplant and half of those needed a second transplant.6 These data convey the burden of LN not only during childhood but continuing after transition to adulthood. Ongoing renal inflammation and cumulative damage from repeated flares contribute to poor renal outcome.8–10 A central conundrum is the relatively poor concordance between clinical assessment and findings of kidney biopsy. There is, therefore, a crucial need for improved identification of renal inflammation with better biomarkers.11 12
There have been increasing efforts dedicated to identifying markers of active LN, allowing the targeting of interventions. As the therapeutic armamentarium for SLE improves, precision approaches to the disease become feasible. Plasma markers of LN have recently been identified and point to both immune activation and tissue remodelling.13 Specifically for paediatrics, a constellation of six inflammatory mediators (NGAL, KIM-1, MCP-1, APN, CP, HEPX) in the urine has been identified that are increased in active LN.14 15
Urinary biomarkers are particularly attractive as they are not invasive and serial measurements are possible. Diverse markers such as ceruloplasmin, angiostatin, CXCL4, vascular cell adhesion molecule-1 (VCAM-1), MCP-1, NGAL, CD11b, HMGB1, hepcidin and tumour necrosis factor-like weak inducer of apoptosis (TWEAK) have been examined with some success,16–23 however, thus far there has been little consensus.24–26 Human epidermal growth factor receptor 2 (HER2) was included in this biomarker study as a proposed marker of proliferation.27 Our rationale for the selection of these three biomarkers was that HER2 captured proliferation, while TWEAK and VCAM-1 detected infiltration of distinct inflammatory cells with TWEAK arising from myeloid lineage cells and VCAM-1 reflecting endothelial activation. This prospective study was designed to test urinary biomarkers for the ability to correctly associate with LN flare and to predict impending flare.
Patients and methods
Subjects
Prospective paediatric cohort
Paediatric patients with biopsy-proven LN were recruited across the five sites (N=113). The time from biopsy to study entry was a mean of 1.7 years and a median of 1 year with a range of 1 month–9 years. All patients had some treatment prior to enrolment. Patients were enrolled up to 21 years of age and the only exclusion was pregnancy. The mean age was 15 years (median 15 years). Midstream urine and clinical data were collected every 3–4 months after enrolment. We additionally studied three control groups also enrolled up to age 21 years, excluding those with known renal disease: 40 healthy female adolescents (mean age 15.7 years, median 15 years); 28 female subjects with amplified pain syndrome (mean age 15 years, median 15 years) and 20 female patients with rheumatoid factor-positive juvenile idiopathic arthritis (RF+ JIA) (mean age 14.6 years, median 14 years). Paediatric patients who were part of a study on acute kidney injury (AKI) related to bone marrow transplantation (N=50, mean age 13 years) have been previously reported but were reanalysed for this study.28 Urine was stored frozen at the site with Complete Protease Inhibitor Cocktail (Roche) added for stability and shipped in batches for analysis.
Biomarker analysis
All biomarkers were analysed by specific ELISA (HER2, TWEAK and VCAM-1) (R&D, Minneapolis, Minnesota, USA). Urine creatinine was measured using a colorimetric kit from Cayman Chemical (Ann Arbor, Michigan, USA). Samples were run in duplicate by a technician blinded to patient category. Urine creatinine was used to normalise for urine concentration. Normalisation to creatinine did not change the overall conceptual results in this study. Therefore, raw biomarker levels are shown in the figures and tables since normalisation to urine creatinine did not change the results and would be an additional complication in transitioning this assay to point-of-service assay.
Disease activity and endpoint definitions
Recognising the imperfect assessment of flare using current clinical markers,29 we defined two study endpoints. In one analysis, disease activity was defined using renal Systemic Lupus Erythematosus Disease Activity Index 2000 2K (R-SLEDAI). The R-SLEDAI score (range 0–16) represents the sum of: proteinuria of >0.5 g/day or protein/creatinine >0.5, haematuria (>5 cells/high power field), pyuria (>5 cells/high power field) and cellular casts. Each item has a score of 4 points. We defined the active disease outcome as a rise in R-SLEDAI from the previous time point or a rise in serum creatinine of >0.3 mg/dL from baseline. We additionally assessed all non-renal flares using the non-renal elements of the SLEDAI for comparison. New-onset proteinuria time points were defined as the first visit where proteinuria was found with at least one previous time point lacking proteinuria. Only the first time point for each patient was counted when there were multiple episodes of proteinuria. For assessment of previous visit parameters, we used the visit immediately preceding the finding if <5 m prior to the finding.
Statistical analyses
The study design was structured to capture at least 50 flares of LN based on the adult flare frequency of 0.56 flares per year.9 30 Analyses and endpoints were determined during study design. Patient characteristics associated with disease activity (table 1) at 0.05 significance level were included for regression analyses (see below). For other analyses, where appropriate, the level of statistical significance corrected for multiple comparisons using the Bonferroni method appears in the figure legend. Summary statistics were generated including frequency tables and mean, SD, minimum, maximum, median and IQR for continuous measures (including biomarker levels).
Clinical and laboratory features associated with renal disease activity
The association of patient-level and visit-level characteristics with LN endpoints was assessed with Χ2 or Welch-Satterthwaite tests for categorical and continuous variables, respectively. Welch-Satterthwaite was selected as the continuous measures were normally distributed but with unequal variance. To ensure a consistent approach, all comparable analyses used that test. Biomarker levels in patient subgroups were assessed using Mann-Whitney U tests due to biomarker levels being non-normally distributed. Kruskal-Wallis was used to analyse biomarker levels across different subsets of patients with multiple classes. The association of biomarker urine levels was also assessed using mixed-effects logistic regression while controlling for variables identified in bivariate analyses or considered clinically meaningful. The models included biomarkers, demographic variables, autoantibodies, time on study, International Society of Nephrology (ISN) class, medications, with rise in R-SLEDAI and serum creatinine as the outcomes. The models were run iteratively until they converged. All analyses were done using SAS V.9.4 except the receiver operating characteristic (ROC) curves which used Prism V.9. Graphs were generated in Prism V.9. All analyses were done with significance level 0.05 with Bonferroni correction for multiple comparisons when noted.
Results
Paediatric prospective cohort description
We enrolled 113 subjects previously diagnosed with LN, collecting urine samples every 3–4 months with clinical data matching each time point to better assess the utility of HER2, TWEAK and VCAM-1 as biomarkers in paediatric LN (N=771) (figure 1A). The gender of participants was 81% female, and the median age was 15 years. The cohort was 35% African American, 25% Caucasian, 17% Hispanic, 12% Asian and 12% multiple races. The number of visits ranged from 1 to 20 with a mean of 7 visits and 2 years of longitudinal data. The distribution of ISN class at entry demonstrated expected diversity with class IV being most common at 41% (online supplemental table 1). Seven participants out of 18 who had a second biopsy had an increase in the ISN biopsy class during the study. Two patients entered the cohort with a flare defined by serum creatinine increased over baseline. SLE autoantibodies at the time of entry into our cohort were as expected (online supplemental table 1). Similarly, medications were also typical for an SLE cohort (online supplemental table 2).
Supplemental material
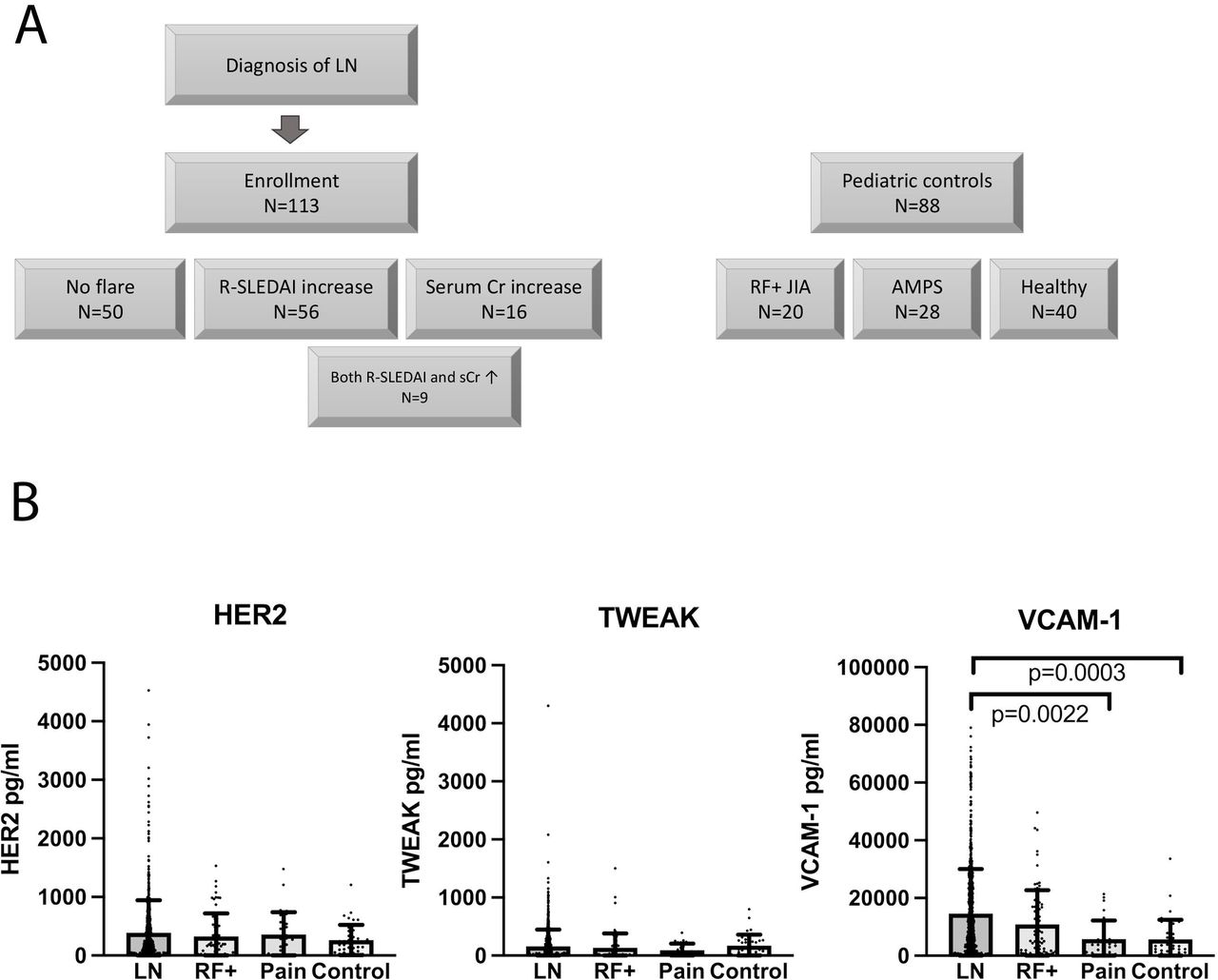
Urine biomarker study. (A) The sample sizes of the clinical subsets described in the manuscript are displayed. (B) HER2, TWEAK and VCAM-1 were measured by ELISA in the entire LN cohort and three control cohorts with RF+JIA (RF+), amplified pain (Pain) and healthy donors (Control). Significance after Bonferroni correction was set at 0.0083. VCAM-1 is significantly higher in LN compared with Pain and Control. The bars represent the mean and the error bars are SDs with each dot representing a single measure. AMPS, amplified pain syndrome; Cr, creatinine; HER2, human epidermal growth factor receptor 2; LN, lupus nephritis; RF+ JIA, rheumatoid factor-positive juvenile idiopathic arthritis; R-SLEDAI, renal Systemic Lupus Erythematosus Disease Activity Index; TWEAK, tumour necrosis factor-like weak inducer of apoptosis; VCAM-1, vascular cell adhesion molecule-1.
Biomarkers across cohorts
We compared biomarker levels in the entire LN cohort with three control groups: 20 female patients with RF+ JIA with 60 visits, 28 female patients with amplified pain syndrome (single visit) and 40 healthy female teenage controls (single visit) (figure 1B). There were no differences between the LN cohort and the three control groups regarding urinary levels of HER2 and TWEAK. VCAM-1, however, was elevated in the LN cohort when compared with patients with amplified pain syndrome (p=0.0022) and healthy controls (p=0.0003). Importantly, none of the biomarkers were increased in RF+ JIA compared with controls. These data suggest that an inflammatory disease state such as RF+ JIA does not lead to increased levels of these biomarkers in urine, although disease activity was not assessed. All three biomarkers were strongly associated with each other across the cohorts with p<0.0001 in all pairwise comparisons using Pearson correlation.
Biomarker associations in the LN cohort
To understand the variables governing biomarker levels in urine, we first analysed levels according to ISN class at entry (online supplemental figure 1A). Kruskal-Wallis analysis of association with ISN class did not show any association with HER2 and TWEAK levels. VCAM-1 levels were associated with ISN class by Kruskal-Wallis. We further analysed whether the biomarker levels were associated with any of the non-R-SLEDAI components. Cumulative non-R-SLEDAI components from zero to seven are displayed in online supplemental figure 1B. There were no detectable trends of HER2 and TWEAK levels with increasing numbers of non-R-SLEDAI components. VCAM-1 levels trended higher with increasing levels of non-R-SLEDAI components. These data collectively suggest that non-renal features do not influence the HER2 and TWEAK levels.
Disease activity
We used the most common definitions for LN flare to identify associations between biomarkers and LN flare. The overall flare rate was 56% in this paediatric cohort with known LN. Fifty-six subjects (50%) had a rise in their R-SLEDAI score and there were a total of 90 visits that met this definition (ie, there were multiple flares in some patients). We identified 16 patients (14%) who had a rise in serum creatinine >0.3 mg/dL over baseline. Some patients had multiple flares with a total of 35 visits with a rise in serum creatinine. Of those, nine patients also had active disease defined by a rise in R-SLEDAI (figure 1A). We determined whether any clinical feature or medication was associated with disease activity (table 1) using bivariate analyses. There were individual associations with R-SLEDAI rise and increased serum creatinine but no single variable was associated with both endpoints, supporting that these two measures are distinct metrics of disease.
Biomarkers and detection of renal disease activity
To understand whether biomarkers can detect different aspects of renal disease, we assessed biomarker levels in the LN cohort associated with each component of the R-SLEDAI score cross-sectionally treating each time point as an individual data point (figure 2A). Elevated HER2 and VCAM-1 levels were associated with proteinuria cross-sectionally. We further compared flare time points defined as either a rise in R-SLEDAI or rise in creatinine with 34 patients who never flared (NEVER Flared) or time points excluded by the criteria of disease activity (Non-flare) (figure 2B). HER2 and VCAM-1 levels were higher at time points defined by a rise in serum creatinine compared with time points with inactive disease. VCAM-1 additionally was higher at flare time points defined by rise in R-SLEDAI when compared with patients who never flared.
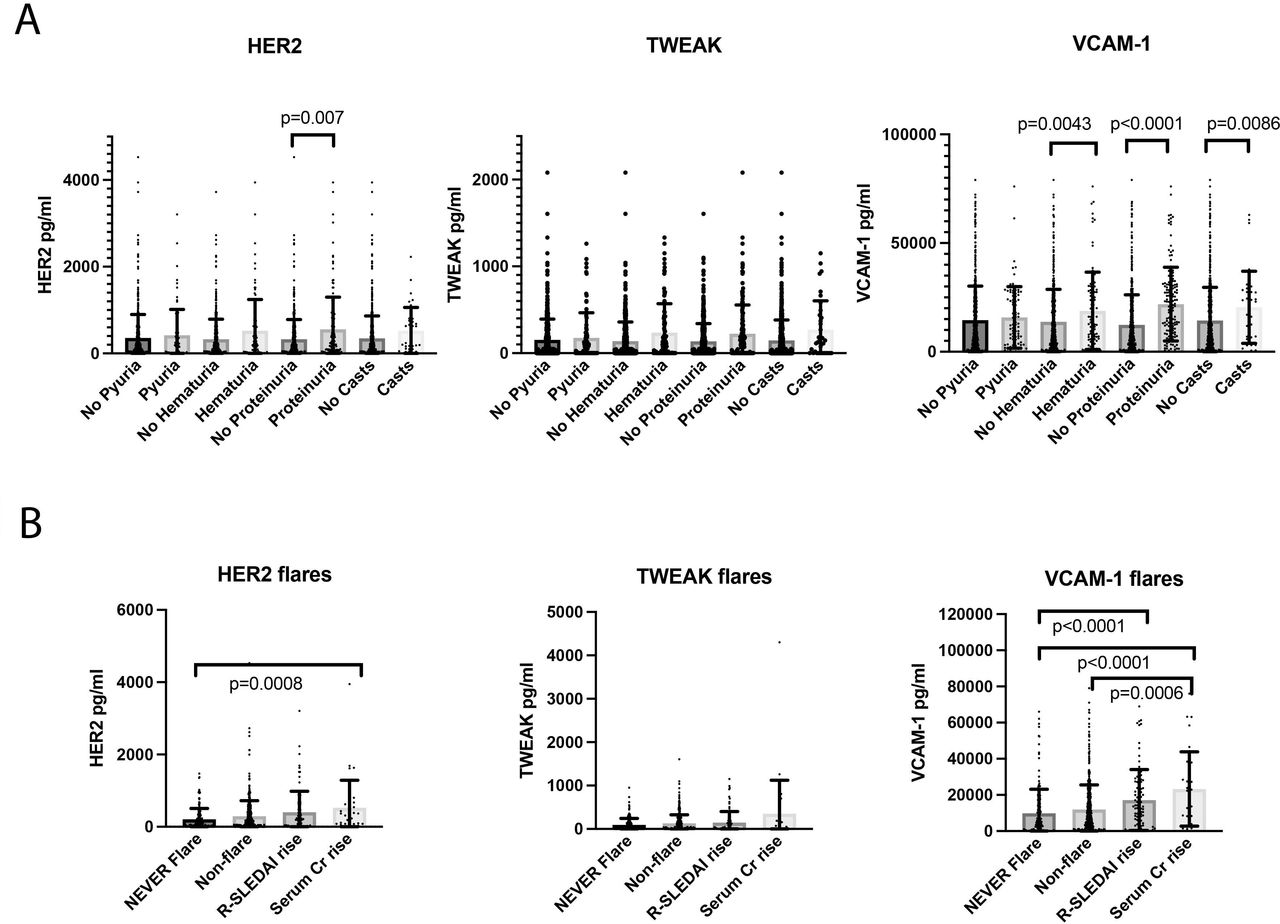
Urine biomarkers analysed according to disease characteristics. (A) Each separate component of the R-SLEDAI score was analysed cross-sectionally with respect to biomarker levels. Significance after Bonferroni correction was set at 0.0125. None of the biomarkers were statistically associated with pyuria but all three were associated with the other components of the R-SLEDAI. Individual p values are shown above the bars. (B) Biomarker levels were compared from visits at the time of a rise in R-SLEDAI or serum creatinine (Cr). Significance after Bonferroni correction was set at 0.0083. The comparator groups are patients who never flared (inactive) or non-flare time points across the entire cohort. Elevated HER2 levels were associated with time points with increased serum Cr compared with time points of patients who never had a flare. VCAM-1 levels were associated with time points with increased serum Cr compared with both patients who never had a flare and patients with inactive disease at time of urine collection. Furthermore, VCAM-1 levels were elevated in time points with R-SLEDAI rise when compared with time points of patients who never had a flare. The bars represent the mean and the error bars are SDs with each dot representing a single measure. HER2, human epidermal growth factor receptor 2; R-SLEDAI, renal Systemic Lupus Erythematosus Disease Activity Index; TWEAK, tumour necrosis factor-like weak inducer of apoptosis; VCAM-1, vascular cell adhesion molecule-1.
We used mixed-effects logistic regression to determine if biomarker levels were independently associated with disease activity defined by a rise in R-SLEDAI score or serum creatinine (table 2). All three biomarkers were associated with a rise in serum creatinine by this logistic regression analysis. Other than medications (online supplemental table 3) and time on study (p=0.001 for rise in creatinine and p=0.0002 for rise in R-SLEDAI), only the biomarkers reached significance. We evaluated sensitivity and specificity of each biomarker according to the two flare definitions. Sensitivity was not strong but specificity was >70% for HER2 and VCAM-1 (table 3). The specificity was 93% when restricted to cases with elevation of all three biomarkers.
Mixed-effects logistic regression analysis of biomarker levels*
Sensitivity and specificity of biomarkers
Proteinuria, a component of the R-SLEDAI, can reflect impaired renal function due to pre-existing disease or active LN. We therefore assessed new-onset proteinuria in 53 subjects and compared with inactive patients and time points without proteinuria (figure 3A). Of these patients with new-onset proteinuria, 32% had a subsequent rise in R-SLEDAI, 25% never resolved, 36% entered a remission defined by R-SLEDAI=0 and 3% had insufficient follow-up. All patients had a change in therapy related to the new-onset proteinuria, with 100% receiving corticosteroids in some form. There was a strong association of each biomarker with new-onset proteinuria, defined as proteinuria arising after at least one visit with negative protein in the urine. Analysing this as a secondary outcome measure using mixed-effects logistic regression, we confirmed the association of all three biomarkers with new-onset proteinuria (table 2). We similarly assessed sensitivity and specificity for new-onset proteinuria using ROC curves (figure 3B). All three biomarkers showed association with new-onset proteinuria.
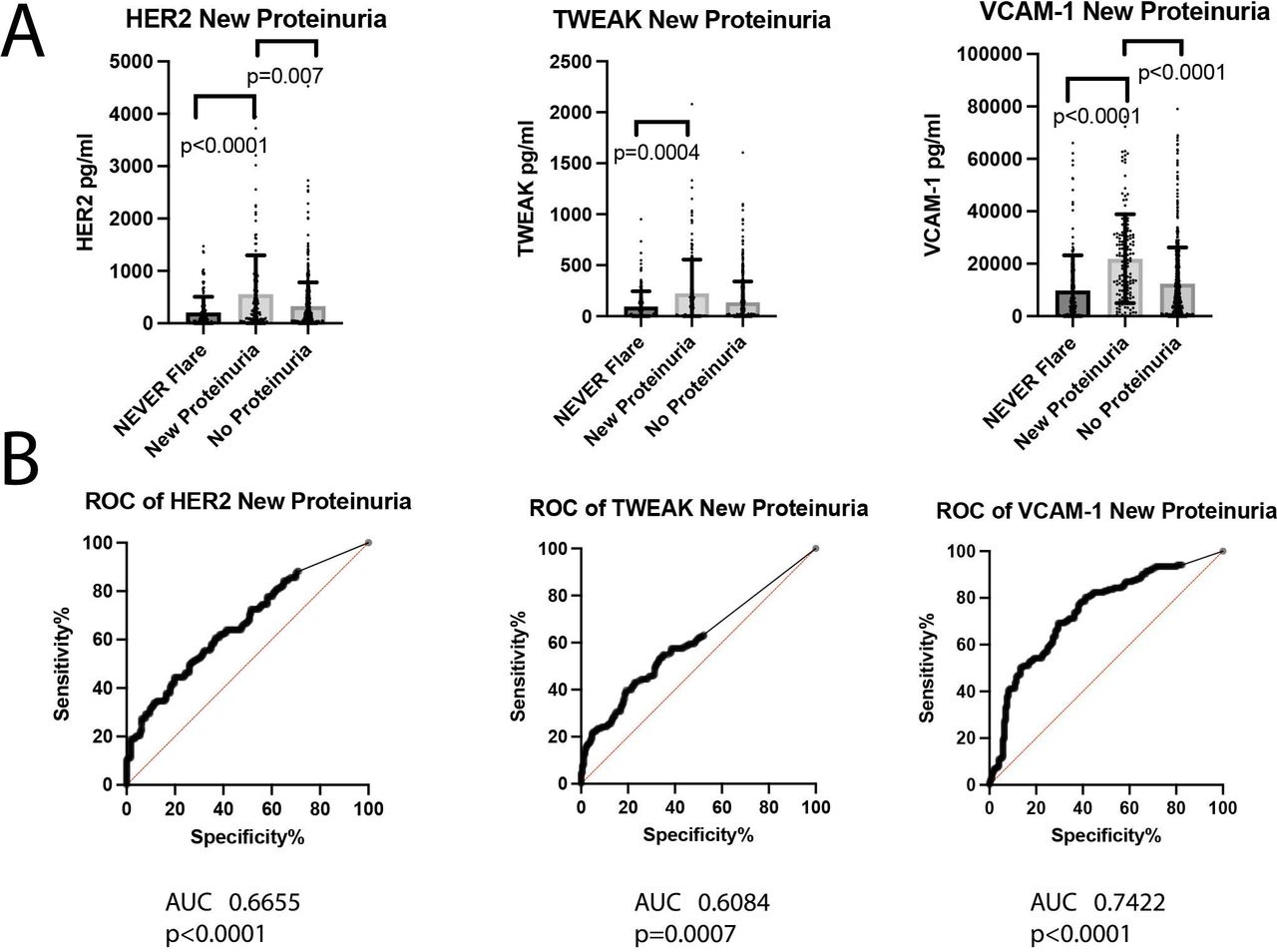
New-onset proteinuria. (A) We identified patient time points that had new-onset proteinuria, defined as the first visit with proteinuria (N=53). Biomarker levels were compared from those time points versus the biomarker levels from patients who never flared and time points without proteinuria. Significance after Bonferroni correction was set at 0.0167. All three biomarkers were significantly higher in the new-onset proteinuria time points. The bars represent the mean and the error bars are SDs with each dot representing a single measure. P values are indicated where significant. (B) ROC curves were used to display sensitivity and specificity. The area under the curve (AUC) and p values are displayed under each graph. HER2, human epidermal growth factor receptor 2; ROC, receiver operating characteristic; TWEAK, tumour necrosis factor-like weak inducer of apoptosis; VCAM-1, vascular cell adhesion molecule-1.
A common clinical question is distinguishing between renal damage related to illness or medications from LN. We therefore assessed whether AKI could lead to elevated urinary HER2, TWEAK and VCAM-1 levels. We had collected urine from 50 children undergoing a bone marrow transplant to identify biomarkers of AKI.28 AKI was defined as a 1.5-fold increase in serum creatinine. Urine levels of the three biomarkers were compared cross-sectionally in the cohort using time points with AKI and those time points without AKI. The children in this study were of comparable age (13 years in the AKI cohort compared with 15 years in the LN cohort). In this cohort, AKI was not associated with any change in biomarker levels (online supplemental figure 2). Thus, injury per se is not associated with increased urinary HER2, TWEAK or VCAM-1.
Biomarker levels and impending flare
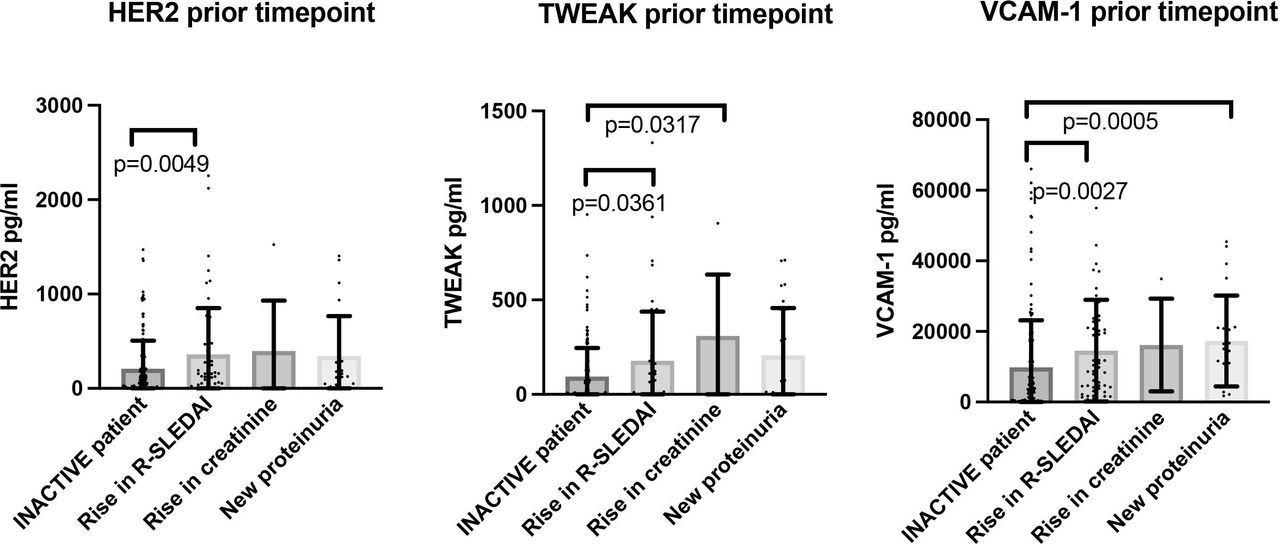
The data thus far indicate an association of the biomarkers in the urine with different measures of disease activity. The biomarkers were most strongly associated with new proteinuria which could be a marker of new renal insult.31 32 We leveraged the longitudinal nature of our study to examine whether the time point prior to the rise in R-SLEDAI, serum creatinine or new-onset proteinuria demonstrated higher levels of biomarkers compared with biomarker levels in those who never flared or time points without flare (figure 4). All three biomarkers were increased at time points preceding any activity defined by R-SLEDAI with HER2 and VCAM-1 demonstrating significance. Elevated VCAM-1 was seen at the time points preceding new-onset proteinuria.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Previous time point analysis of urine biomarkers. We analysed the samples prior to visits where patients had a flare defined by rise in serum creatinine, new proteinuria or a rise in R-SLEDAI. Significance after Bonferroni correction was set at 0.0083. Non-significant p values are shown in grey. All three biomarkers were increased at time points prior to a rise in R-SLEDAI. The bars represent the mean and the error bars are SDs with each dot representing a single measure. HER2, human epidermal growth factor receptor 2; R-SLEDAI, renal Systemic Lupus Erythematosus Disease Activity Index; TWEAK, tumour necrosis factor-like weak inducer of apoptosis; VCAM-1, vascular cell adhesion molecule-1.
Discussion
There is a need for improved detection of flare in LN.29 Undetected flares drive renal damage and untreated inflammation can lead to renal failure. We designed a study to exploit the availability of urine as a possible diagnostic approach. We included two well-studied biomarkers and a less studied biomarker, reasoning that they captured distinct pathological processes. HER2 is not an obvious biomarker and we initially identified it from an unbiased screen of micro-RNAs.33 It is better known as a biomarker for metastatic breast cancer34 35 and is thought to be central to proliferation,36 which is a key pathological mechanism in LN. We previously found overexpression of HER2 in the glomeruli and tubular compartments of the kidneys of patients with LN, but not in other proliferative glomerulonephritides, such as IgA nephropathy, post-streptococcal glomerulonephritis and granulomatosis with polyangiitis.33 This study found there was no association with AKI, further refining the specificity.
This prospective study of paediatric LN also examined urinary TWEAK and VCAM-1 as biomarkers. TWEAK is a pro-inflammatory cytokine primarily produced by monocytes and macrophages. Adult patients with SLE with active kidney disease have significantly higher urinary TWEAK levels.37 Levels rise at the beginning of a renal flare, peak at the time of diagnosis and progressively decrease after the resolution of the flare, leading to a study of a TWEAK inhibitor as therapy.38 VCAM-1 is expressed on endothelial cells and tubules and it participates in the migration and recruitment of leucocytes.39 VCAM-1 can distinguish active LN from inactive disease in adults and is sensitive to change in status.22 40 Our study found higher VCAM-1 in those patients with class V disease at entry. In another study, VCAM-1 in urine was also seen in the higher grades of LN (class IV and class V).41 A recent large analyte screen using SomaScan also found VCAM-1 levels to be significantly associated with active LN in adults.40 HER2 was not included in that study. High VCAM-1 may indicate risk for long-term renal function loss,42 however, it is not specific to LN, since it is elevated in other renal diseases, including ANCA-associated glomerulonephritis, focal segmental glomerulosclerosis and membranous nephropathy.41 These biomarkers were selected based on the strong foundational support for further testing in paediatric LN. The unique structure of this study allowed us to powerfully interrogate biomarker associations in a manner not previously performed in paediatric LN.
The most unique aspect of this study was its longitudinal nature. All three biomarkers were associated with new-onset proteinuria but only VCAM-1 was elevated prior to time points with new-onset proteinuria. All three biomarkers were increased at time points prior to the rise in R-SLEDAI.
This multicentre study also provides important clinical data on paediatric LN in the USA. The rate of flare was 56% over an average of 2 years of follow-up. This humbling statistic emphasises the unmet need for improved risk stratification and treatment for paediatric LN. This study had several strengths. It investigated populations of diverse racial and ethnic backgrounds and it is the largest prospective study of paediatric LN. We selected the study of paediatric LN because there is a critical need for additional information. Children with SLE are known to have more severe nephritis than adults and indeed our cohort had 71% proliferative LN (ISN class III or IV). The longitudinal nature of the study allowed us to identify changes in disease activity and analyse the biomarkers at the time of previous clinical visits. This was an important tool to understand the true predictive value of the biomarkers and, consequently, the clinical utility of their use. Nevertheless, these findings will require validation in additional cohorts and the use of the biomarkers in patients who have not yet developed LN remains to be studied. Our study does have weaknesses, however. A larger study of analytes could identify whether biomarkers identified at the time of flare are different than the biomarkers that precede a flare. The number of samples analysed for the prior visit analyses was comparatively low, thus a larger study will be required to confirm these findings. Collection of urine samples and clinical data every 3 months is a landmark in the field of paediatric SLE, however, more frequent sampling might reveal additional insights into the kinetics of each of these biomarkers. Our study was also limited by the inclusion of patients with known LN. Therefore, we cannot determine the utility of these biomarkers for new-onset cases. Increased HER2 and TWEAK were not seen in patients with high numbers of active non-R-SLEDAI components nor with RF+ JIA, suggesting that inflammatory disease on its own does not drive higher levels of these urine biomarkers.
Many biomarkers have been suggested in the last decades by exploring pathophysiological pathways associated with LN or by performing unbiased high-throughput screens. Yet, no single urinary biomarker has outperformed the estimated glomerular filtration rate or proteinuria as measures for diagnosis or for following disease activity. An ideal biomarker should be specific for renal involvement, predict impending flares, be useful for serial monitoring, be more sensitive than conventional approaches and be easy to perform. These biomarkers meet these requirements by rising at the time point that precedes a rise in R-SLEDAI, demonstrating specificity and using a readily available sample. Nevertheless, it is most likely that a single biomarker will not be enough to determine the activity of LN and only the combined analysis of several biomarkers that reflect different aspects of LN pathogenesis will be truly meaningful. One example of this strategy is RAIL (Renal Activity Index for Lupus), a non-invasive composite biomarker of LN. RAIL has been validated in both children and adults but requires a complex weighting of inputs for analysis.14 43 The SomaScan analysis also concluded that a composite of eight analytes offered the best association with active LN.40 In this regard, HER2 represents a potential addition to the biomarker options.
In conclusion, we showed that elevated urinary HER2, TWEAK and VCAM-1 levels are all strongly associated with new-onset proteinuria. Additionally, the three biomarkers were elevated at the visit prior to a rise in R-SLEDAI. This prospective paediatric study demonstrates that it is possible to identify biomarkers to predict disease activity in children. Early detection, prior to accumulation of renal damage, is central to improved treatment that minimises long-term accrual of damage and the evolution of end-stage renal disease.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information. Primary data are avaialble upon request.
Ethics statements
Patient consent for publication
Ethics approval
The study complies with the Declaration of Helsinki and the protocol was approved by the Institutional Review Boards of all the participating institutions after review by CHOP Institutional Review Board as study ID14-011429 (Children’s Hospital of Philadelphia, Duke Children’s Health Center, Lurie Children’s Hospital, Riley Children’s Hospital and University of California San Francisco Benioff Children’s Hospital). Patients provided written informed consent prior to enrolment.
Acknowledgments
The authors thank the Barlin family for their unwavering support and funding. The many study coordinators who participated in outreach, enrolment and sample collection are gratefully acknowledged here. This would not have been possible without Amy Rakestraw, Mariah Boncek, Brooke McCallum, Stella Protopapas, Bhupinder Nahal, Taylor Goldberg, Alexandra Martyniuk and Ca’Lecia Fleming.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors (PC-R, KM, MAP, DLE, XZ, WF, JB, KO, MSK-G, EvS, LES, KES) interpreted data, edited and revised the manuscript, approved the submitted version and are accountable for all aspects of the work. KES designed the study and WF and KES performed data analyses. Amy Rakestraw, Mariah Boncek, Brooke McCallum, Stella Protopapas, Bhupinder Nahal, Taylor Goldberg, Alexandra Martyniuk and Ca’Lecia Fleming performed critical data collection and data entry. KES is the guarantor.
Funding This work was supported by the Lupus Foundation of America. The Hopkins Lupus Cohort is supported by NIH RO1-AR069572. KES is also supported by the Wallace Chair of Pediatrics.
Competing interests LES is associate editor for Lupus Science & Medicine.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.